
These evidence-based clinical recommendations emphasizing holistic care provide actionable ways for hearing care professionals to address the complex relationship between hearing and cognition in their practices.
By Victoria Sanchez, AuD, PhD; Louise Hickson, PhD; Stacey Rich, MAud; Theresa Chisolm, PhD; Kristin Davis, AuD; Jennifer Deal, PhD; Matthew Fitzgerald, PhD; Nicholas Reed, AuD, PhD; Todd Ricketts, PhD; Jennifer Lister, PhD; Angela Pelosi, MAuD, MBA; Brandy Pouliot, AuD; Julia Sarant, PhD; Maren Stropahl, PhD
Introduction
The aging of the population brings an increasing prevalence of both hearing loss and cognitive decline in older adults. Understanding the relationship between these two conditions is essential for providing holistic hearing healthcare. Hearing and cognition have a dynamic and bidirectional relationship. Hearing loss can lead to reduced communication and increased cognitive load and social isolation, all of which may contribute to cognitive decline. Conversely, cognitive impairment can affect an individual’s ability to process auditory information, making effective communication more challenging. Cognitive impairment may also hinder hearing loss management.
Unmanaged hearing loss increases the risk of cognitive impairment and dementia on average in the population, but this risk varies between individuals, and whether the association is causal is unknown. Observational evidence suggests hearing aid use may decrease the risk of cognitive decline and dementia (e.g., Yeo et al., 2023; Cantuaria et al., 2024). For example, in a well-designed observational cohort study, ENHANCE, hearing intervention was found to support cognitive health which may delay decline for several years (Sarant et al., 2024). Furthermore, in the recent landmark randomized controlled trial, ACHIEVE, it was demonstrated that comprehensive hearing intervention with provision of hearing aids and assistive devices and regular audiology care including counseling, education, and self-management support slowed cognitive decline in some, but not all (Lin et al., 2023). While encouraging, more research is needed, and we do not have evidence that hearing aids prevent dementia at this time.
However, with increased awareness of the link between hearing loss and cognitive decline, some patients expect that their hearing care professional provide holistic care including promoting cognitive health (Muir et al., 2025). Recognizing and addressing the interplay between hearing loss and cognition allows hearing care professionals to develop more effective strategies for assessment, intervention, and patient support to improve overall health and quality of life for older adults. Here, we provide evidence-based clinical recommendations for hearing care professionals to address the complex relationship between hearing and cognition in their practices.
Assessment and Evaluation
1. Integrate Best Practices for Recognizing Cognitive Change.
Hearing care professionals occupy a unique position to observe and recognize cognitive and functional changes in patients. Although cognitive screening may be within the clinicians’ scope of practice, formal screening of asymptomatic adults is not recommended (e.g., United States Preventative Services Task Force; Canadian Task Force on Preventative Health Care), as there is insufficient evidence that this improves patient or caregiver outcomes. Conducting cognitive screenings before and after hearing intervention is also not recommended, as cognitive performance fluctuates over time and depends on many factors, not only hearing or cognitive ability. Increased performance on one occasion could lead to false hope of improvement, while decreased performance could lead to unwarranted anxiety. As hearing care professionals are not trained to interpret formal diagnostic cognitive assessments, conducting routine cognitive testing will place additional burdens of loss of time, fatigue, and cost on patients who may then be referred for further diagnostic evaluation.
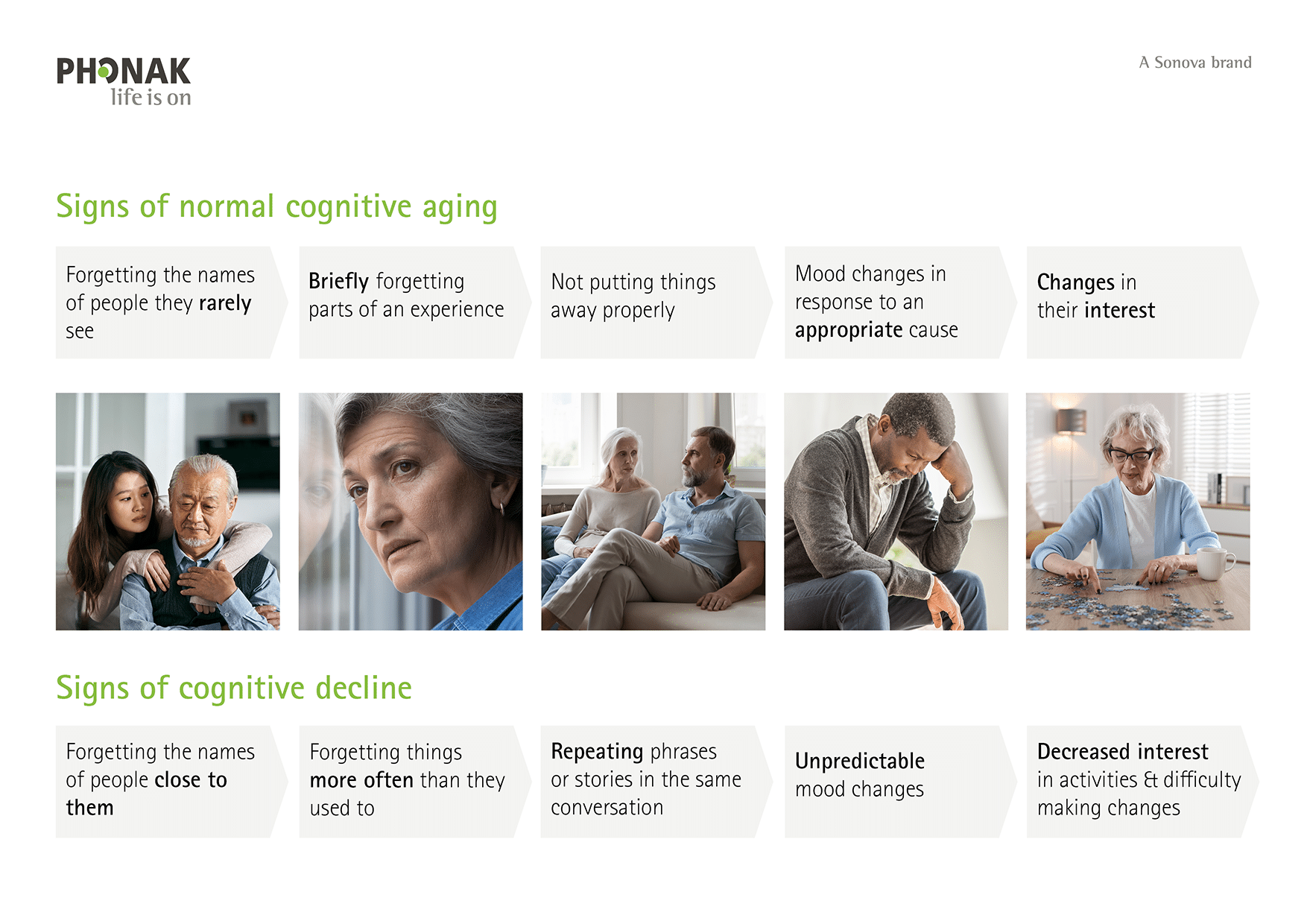
Instead, hearing care professionals should be informed about signs of cognitive decline and how these differ from those of normal cognitive aging so they can recognize when cognitive factors may be impacting a patient’s hearing assessment or treatment outcomes and know when to refer to specialists (Figure 1).
Hearing care professionals should monitor patient behavior and interaction through active listening and observation, combined with taking notes in client records for later follow-up. Explicitly asking about, and then following up with patients and their care partners on any reported cognitive problems and concerns is important. A screening question such as “During the past 12 months, have you experienced confusion or memory loss that is happening more often or getting worse?” could be used (The Gerontological Society of America, 2020). If hearing care professionals have concerns about suspected cognitive decline in patients, they should refer to other professionals who are dementia specialists and are extensively trained in these areas (e.g., geriatricians, psychologists, neurologists).
2. Adopt a Holistic Hearing Health Approach for Assessment.
Routine assessment should extend beyond pure-tone audiometry to include hearing and communication symptom questionnaires, speech-in-noise tests, and hearing-related psychosocial health measures [see recent recommendations, (National Academies of Sciences & Medicine, 2025)]. Consider the cognitive demand of the different auditory assessments and interpret results appropriately. Be mindful of the hearing-cognition relationship and appreciate both how hearing loss affects cognition, how cognitive status impacts auditory function and hearing assessment outcomes, and how both hearing and cognition change over time.
Intervention
3. Talk about Proven Benefits of Hearing Interventions.
Anchor individual hearing needs and goals to well-established benefits of hearing interventions – improved communication, quality of life, social engagement, and reduced listening effort— rather than using unsubstantiated claims about dementia prevention. The importance of hearing health to brain health should not be ignored but should not be the leading recommendation for hearing intervention uptake. Specifically, never use the association between hearing loss and dementia to encourage hearing aid use for patients. This is a professional ethics issue. Discuss proven benefits and limitations in a balanced manner without causing unnecessary fear or anxiety. Discuss the evidence supporting the benefits of hearing interventions for increased social engagement and decreased loneliness (Reed et al, 2025), improved overall communication (Sanchez et al, 2024), and reduced risk of falls (Goman et al, 2025); all of which also support good physical and brain health.
4. Provide Comprehensive Best-Practice Patient- and Family-Centered Hearing Interventions.
Provide evidence-based, gold standard hearing interventions. The intervention should be guided by a functional and communication needs assessment including family and communication partners as much as possible (Hickson et.al., 2014; Singh et.al., 2015). Most interventions will include technological solutions (e.g., hearing aids, cochlear implants, assistive devices) as well as therapeutic solutions (e.g., communication education, counseling, self-management training). Regular check-in sessions are needed to ensure patient and family goals are met as needs change over time.
5. Adapt Audiology Services for Patients with Cognitive Impairment.
A recent US study found that almost 80% of adults aged 71 years or older with dementia had significant hearing loss (Nieman et al, 2024). In this cohort, only 21.7% used hearing aids. It is important to prioritize identifying and treating hearing loss in this population to improve quality of life, support independence (Hougaard et.al., 2016), and reduce symptoms related to hearing loss (Holman et.al., 2021), including depression (Zhang et al, 2024).
Intervention approaches should be adapted for patients with cognitive impairment using modified assessment techniques, simplified instructions, visual supports, and cues. Family and caregivers should be actively engaged to support intervention adherence and should be educated on the benefits of improved communication that can help with mood and neuropsychiatric symptoms such as depression, aggression, and anxiety. Relationships with inter-disciplinary professionals (such as gerontologists or neuropsychologists) will facilitate the exchange of information about patients’ cognitive status, enabling subsequent tailoring of individual hearing intervention programs.
Communication and Ethics
6. Tailor Communication and Clinical Recommendations Based on Patient and Family Factors.
Not all patients and/or families need to discuss cognition with their hearing care professional. It is important to meet patients “where they are,” recognizing that auditory and cognitive factors vary by age, sex, race, ethnicity, and education level, requiring individualized approaches. For patients asking about hearing and cognition concerns, providers can indicate that conclusive evidence is not yet available to answer questions about how hearing intervention impacts a specific patients’ cognition or dementia risk. However, it may be shared that the existing evidence indicates that hearing intervention for patients with multiple risk factors including older age, physical function limitations, and other co-morbidities may facilitate the greatest benefits.
7. Use Appropriate Evidence-Based Language.
Avoid statements like “hearing loss causes dementia” or “hearing aids will prevent you from acquiring dementia.” Current evidence does not support these statements, but there is some evidence in population-based studies and clinical trials linking hearing care and brain health. Use statements like ‘Hearing aids can help you hear and communicate better, all of which can encourage many positive health benefits.” Discuss the benefits of treating hearing loss beyond hearing better: “Taking action to hear better can support healthy aging and overall well-being.” Let patients know that they will also benefit from person-centered goal setting and counselling and that using hearing aids helps to maintain social connections and to keep the brain stimulated.
8. Ensure Marketing Materials Are Evidence Based.
Marketing materials for hearing devices and services must not indicate any causative association between hearing loss and dementia and must not promote hearing aids as dementia prevention tools. All communications should be grounded in evidence and neither over- nor under-stated.
Care Coordination and Policy
9. Establish Multidisciplinary Care Pathways.
Develop robust referral pathways between audiology and cognitive services, fostering interdisciplinary collaboration between audiological and dementia specialists to provide appropriate counseling and support for patients with both hearing and cognitive concerns.
10. Advocate for Policy Change & Joint Development of Practice Standards.
Given the magnitude of health benefits and the minimal medical risk of hearing interventions, hearing care professionals are encouraged to support policy that addresses hearing loss. Hearing intervention and treatment of hearing loss are essential for overall healthy aging, and even more so for older adults with multiple risk factors that impact physical and cognitive health. Hearing care professionals with memberships in professional organizations should request that their organization participates in the development of formal practice guidelines and position statements to further guide clinical practice on the interconnected hearing and cognition relationship.
These recommendations emphasize a holistic, patient- and family-centered approach that considers the interconnected relationship between hearing and cognition while maintaining ethical standards and evidence-based practice.
Author Bios and Disclosures of Affiliation and Compensation:
Author’s name, degrees, place(s) of employment and title(s) are reported in addition to any financial or non-financial disclosures or possible conflicts of interest over the 12 months (prior to February 2026).
Victoria Sanchez, AuD, PhD, is an associate professor in the Department of Otolaryngology and chief of Audiology at the University of South Florida. She reports salary and research support to the Auditory Rehabilitation & Clinical Trials Laboratory at the University of South Florida. She also reports industry funding related to consulting or research support from Sensorion, Sonova Holding AG, and Phonak USA. She has received funding to the University of South in the form of grants from the National Institute of Health (R01AG075083, R01AG076518, R01DC019408). Hearing aids, hearing assistive technologies, and related materials used in recent studies were provided at no cost to the researchers or the participants from Sonova/Phonak LLC.
Louise Hickson, BSpThy(Hons), MAud, PhD, is emeritus professor at The University of Queensland in Australia. She reports research support from the Australian Research Council, the Medical Research Future Fund, the National Health and Medical Research Council, and consulting and research support from Sonova AG. She is on the Executive Board of the International Society of Audiology.
Theresa Chisolm, PhD, is a professor at the University of South Florida. Portions of her salary to the University of South are currently supported by the National Institutes of Health (NIA R01AG076518, NIDCD R01DC019408). She has received indirect support from Sonova/Phonak LLC via provision of hearing aids, hearing assistive technologies, and related materials at no cost to the researchers or the participants in NIH-funded studies.
Kristin C. Davis, AuD, is a Distinguished Practitioner Fellow in Audiology of the National Academies of Practice and the owner of Davis Audiology in Greenville, S.C. She has no additional pertinent disclosures.
Jennifer A. Deal, PhD, is an associate professor in the Department of Epidemiology, Cochlear Center for Hearing and Public Health, Johns Hopkins Bloomberg School of Public Health. She reports grant funding from the National Institute on Aging, serving as an Associate Editor for the Journals of Gerontology: Medical Sciences, and acting as the interim director of a public health research center funded in part by a philanthropic donation from Cochlear to the Johns Hopkins Bloomberg School of Public Health.
Matthew B. Fitzgerald, PhD, is an associate professor and chief of Audiology at Stanford University School of Medicine. He reports salary support from Stanford University. He currently receives research support from the Stanford Center for Digital Health, and from a donation to the Stanford Initiative to Cure Hearing Loss (SICHL). He is also a co-investigator on grants from NIH DC020698 (P.I. Tilak Ratnanather), and Starkey Inc. (P.I. Kristen Steenerson).
Jennifer Jones Lister, PhD, is a professor in the Department of Communication Sciences and Disorders and senior associate dean of the College of Behavioral and Community Sciences at the University of South Florida. She is currently funded by the Preventing Alzheimer’s with Cognitive Training (PACT) clinical trial (NIH/NIA, R01AG070349) and the USF Optimal Aging and Brain Health Initiative.
Angela Pelosi, MAuD, MBA, is senior director of Global Audiology and Clinic Success at Sonova AG. She is a salaried Employee of Sonova AG.
Brandy Pouliot, AuD, is director of Audiology and Education at Sonova US. She is a salaried employee of Sonova US.
Nicholas Reed, AuD, PhD, is vice president of Audiology Research and Innovation at Amplifon SpA and holds adjunct faculty appointments at the Cochlear Center for Hearing and Public Health in the Department of Epidemiology at the Johns Hopkins Bloomberg School of Public Health and at the Department of Otolaryngology-Head & Neck Surgery at NYU Langone Health He reports employment from Amplifon and grant funding from the National Institutes of Health (NIA, NIDCD). He has received indirect support from Cochlear via a philanthropic donation to the Johns Hopkins Cochlear Center for Hearing and Public Health and Sonova via providing hearing aids and related technologies at no cost to participants in NIH funded studies.
Stacey Rich, MAud, is senior manager of Audiology Thought Leadership and Education at Sonova AG. She is a salaried employee of Sonova US Corporate Services.
Todd A. Ricketts, PhD, is a professor and vice chair of Graduate Studies, Thomas L. and Jane Wilkerson Yount Endowed Chair in Hearing & Speech Sciences, at Vanderbilt University Medical Center. He reports support in part by: NIH NOT-AG-18-039 DC015997-01A1 (P.I. Yu-Hsiang Wu) and device support from Sivantos (now WS Audiology).
Julia Z. Sarant, PhD, is a professor in the Department of Audiology & Speech Pathology at The University of Melbourne in Australia. She reports no industry funding for hearing aid related work over the 12 months prior to February 2026 but received some funding prior to this from Sonova AG.
Maren Stropahl, PhD, is senior director of Holistic Hearing Care at Sonova AG. She is a salaried employee of Sonova AG.
References
Alzheimer’s Association. 2023. 10 warning signs of Alzheimer’s worksheet [PDF]. Alzheimer’s Association. https://www.alz.org/getmedia/15db9fd4-81c7-449d-a4a8-1db2b9f8707b/alzheimers-dementia-10-warning-signs-worksheet.pdf
Cantuaria ML, Pedersen ER, Waldorff FB, et al. Hearing Loss, Hearing Aid Use, and Risk of Dementia in Older Adults. JAMA Otolaryngol Head Neck Surg. 2024;150(2):157-164. doi:10.1001/jamaoto.2023.3509. https://doi.org/10.1001/jamaoto.2023.3509
Gerontological Society of America. (2020). The GSA KAER toolkit for primary care teams: Supporting conversations about brain health, timely detection of cognitive impairment, and accurate diagnosis of dementia (Fall 2020 ed.). https://pa-foundation.org/wp-content/uploads/GSA_KAER-Toolkit_2020_Final.pdf
Goman AM, Tan N, Pike JR, et al. Effects of hearing intervention on falls in older adults: findings from a secondary analysis of the ACHIEVE randomised controlled trial. Lancet Public Health. 2025;10(6):e492-e502. doi:10.1016/S2468-2667(25)00088-X. https://doi.org/10.1016/S2468-2667(25)00088-X
Hickson L, Meyer C, Lovelock K, Lampert M, Khan A. Factors associated with success with hearing aids in older adults. Int J Audiol. 2014;53 Suppl 1:S18-S27. doi:10.3109/14992027.2013.860488
Holman JA, Drummond A, Naylor G. Hearing Aids Reduce Daily-Life Fatigue and Increase Social Activity: A Longitudinal Study. Trends Hear. 2021;25:23312165211052786. doi:10.1177/23312165211052786. https://doi.org/10.1177/23312165211052786
Hougaard S, Ruf S, Egger C, Abrams H. Hearing Aids Improve Hearing–and A LOT More. Hearing Review.2016;23(6):14. https://hearingreview.com/inside-hearing/research/hearing-aids-improve-hearing-lot
Lin FR, Pike JR, Albert MS, et al. Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial. Lancet. 2023;402(10404):786-797. doi:10.1016/S0140-6736(23)01406-X. https://doi.org/10.1016/S0140-6736(23)01406-X
Muir L, Lo CY, Russo FA, Singh G. Client and Clinician Perspectives on the Roles and Responsibilities of Hearing Care Practitioners in Addressing Health Domains Beyond Hearing. Am J Audiol. 2025;34(3):632-641. doi:10.1044/2025_AJA-24-00256. https://doi.org/10.1044/2025_AJA-24-00256
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Committee on Meaningful Outcome Measures in Adult Hearing Health Care. Measuring Meaningful Outcomes for Adult Hearing Health Interventions. Washington (DC): National Academies Press (US); July 22, 2025. https://doi.org/doi:10.17226/29104
Reed NS, Chen J, Huang AR, et al. Hearing Intervention, Social Isolation, and Loneliness: A Secondary Analysis of the ACHIEVE Randomized Clinical Trial. JAMA Intern Med. 2025;185(7):797-806. doi:10.1001/jamainternmed.2025.1140. https://doi.org/10.1001/jamainternmed.2025.1140
Sanchez VA, Arnold ML, Garcia Morales EE, et al. Effect of hearing intervention on communicative function: A secondary analysis of the ACHIEVE randomized controlled trial. J Am Geriatr Soc. 2024;72(12):3784-3799. doi:10.1111/jgs.19185. https://doi.org/10.1111/jgs.19185
Sarant JZ, Busby PA, Schembri AJ, Fowler C, Harris DC. ENHANCE: a comparative prospective longitudinal study of cognitive outcomes after 3 years of hearing aid use in older adults. Front Aging Neurosci. 2024;15:1302185. Published 2024 Jan 31. doi:10.3389/fnagi.2023.1302185. https://doi.org/10.3389/fnagi.2023.1302185
Singh G, Lau ST, Pichora-Fuller MK. Social Support Predicts Hearing Aid Satisfaction. Ear Hear. 2015;36(6):664-676. doi:10.1097/AUD.0000000000000182
Yeo BSY, Song HJJMD, Toh EMS, et al. Association of Hearing Aids and Cochlear Implants With Cognitive Decline and Dementia: A Systematic Review and Meta-analysis. JAMA Neurol. 2023;80(2):134-141. doi:10.1001/jamaneurol.2022.4427. https://doi.org/10.1001/jamaneurol.2022.4427
Zhang L, Yu J, Zhang H, Chen S. Association between the hearing aid and mental health outcomes in people with hearing impairment: A case-control study among 28 European countries. J Affect Disord. 2024;361:536-545. doi:10.1016/j.jad.2024.06.085. https://doi.org/10.1016/j.jad.2024.06.085



This article is most welcome in confirming the statements made in the position statement published by the British Society of Audiology in November 2024. We’re pleased to see that the recommendations are very similar. The guidance is freely available at: https://www.thebsa.org.uk/wp-content/uploads/2024/11/Position-statement-HL-and-dementia-a-guide-for-hearing-professionals-Nov-2024.pdf.