Tech Topic | November 2017 Hearing Review
Makes people talk is the slogan of a humorous advertisement by Läkerol, a manufacturer of throat lozenges. However, it could also be a guideline and rallying call for our profession. Because that’s what it’s all about, isn’t it?
It doesn’t help to hear speech if you can’t understand and respond appropriately. Listening doesn’t make you socially active, communicating does. If you’ve been working in the hearing care profession, you’ve almost certainly encountered patients who stop socializing due to their hearing loss. We know there’s a link between social isolation and mental wellbeing.1,2 That’s why getting people talking and communicating should be one of the primary goals of hearing rehabilitation. As hearing loss remains untreated, social isolation becomes more common.
Acknowledging communication as a primary goal of audiological rehabilitation, the new Signia Nx hearing aids contain Own Voice Processing (OVP™) technology designed to identify when the wearer is speaking. In this way, OVP can employ dual processing for either “external” speech or own-voice conditions. The system simply adjusts the settings when the wearer is speaking, but maintains the prescribed amplification when he or she isn’t speaking, avoiding compromises to amplification, audibility, and noise reduction algorithms.
There have been several studies linking hearing impairment to mental wellbeing, and some even indirectly to dementia. The consequences of untreated hearing loss are a hot topic, and although hearing loss and cognitive decline do seem to be correlated, causation has not yet been established. What we do know is that reduced hearing certainly reduces socialization. It is also reasonable to say that, by improving hearing, the cognitive workload during conversations is lessened.3 This means that, for a person with reduced cognitive skills, it is probable that well-fitted hearing aids make communication easier by freeing cognitive resources.
At Johns Hopkins, Frank Lin and associates conducted a longitudinal study investigating this topic.4 In this study, volunteers with hearing loss, undergoing repeated cognition tests over 6 years, had cognitive abilities that declined 30-40% faster than in those whose hearing was normal. Levels of declining brain function were directly related to the amount of hearing loss. On average, older adults with hearing loss developed a significant impairment in their cognitive abilities 3.2 years sooner than those with normal hearing.
Possible explanations for this cognitive slide, according to Lin et al,4 include the ties between hearing loss and social isolation, with loneliness being well-established in previous research as a risk factor for cognitive decline.1 Degraded hearing may also force the brain to devote too much of its energy to processing sound, at the expense of energy spent on memory and thinking.3 The theory is that the cognitive decline starts when people stop participating and challenging themselves in everyday life. All of this reinforces the need to ensure people are talking and communicating optimally.
Facilitating Communication
We need to optimize, as best we can, the listening environment where people are socializing. First, for people to hear well and understand speech in noisy situations, it’s important to ensure a sufficiently positive signal-to-noise ratio (SNR). Second, if listening becomes too challenging, people experience listening fatigue, and possibly leave or reduce their participation in the conversation and/or social event. The solution for this is to reduce listening effort. Thus, SNR and listening fatigue are important for speech understanding because they directly influence the amount of a person’s social participation and communication. If you are uncertain of what was just said, you’re much less likely to enter into a conversation.
Another important factor is how you personally sound. Listening to our own voice is a stable reference and part of our identity. For hearing aid users, the more their hearing aid-processed voice deviates from their own voice, the less comfortable and natural the experience will be. For some, this even leads to them returning the hearing aids, derailing their entire treatment plan. We can’t underestimate confidence as part of social involvement.
To achieve necessary speech understanding, we need to provide appropriate audibility. Unfortunately, sufficient amplification often leads to reduced listening comfort. One common complaint is that the wearer perceives his/her own voice as loud or unnatural. In an attempt to solve the problem, the hearing care professional often reduces amplification to ensure that the hearing aids are used. This, of course, reduces the audibility of important speech signals.
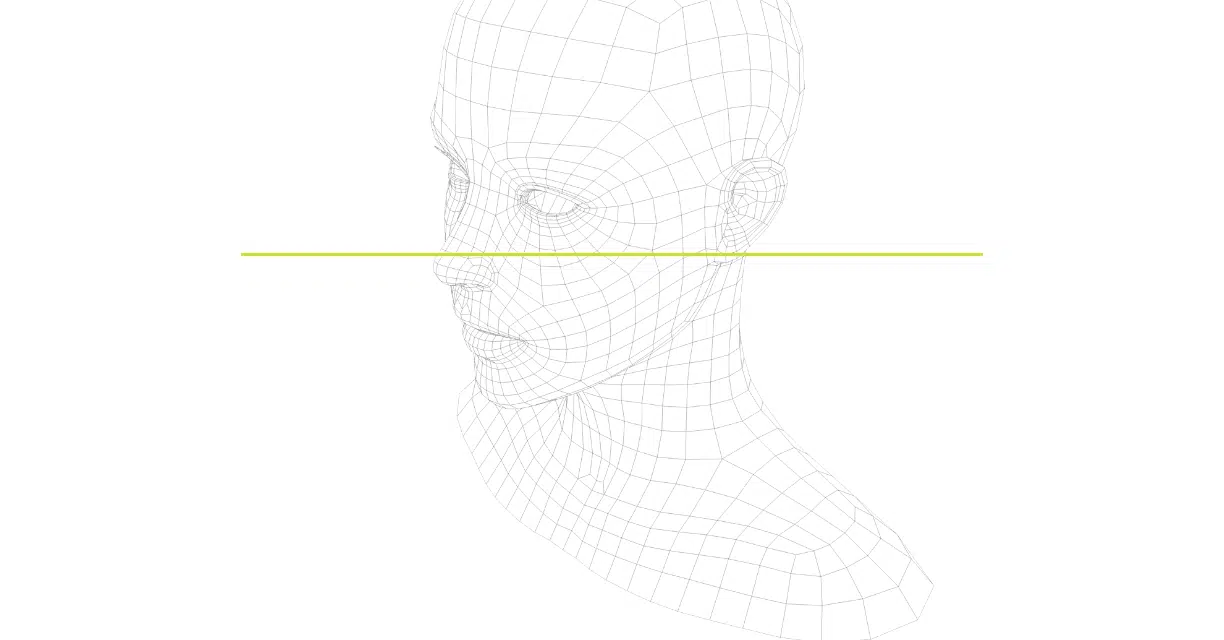
A great tool for understanding the importance of audibility is Killion and Mueller’s “Count-The-Dots” audiogram (Figure 1).5,6 By plotting the patient’s aided thresholds onto this sheet, you can count the dots below the threshold line and obtain an estimate of speech audibility. If there are 70 dots below the line, the articulation index is 70%; in other words, the patient can theoretically hear 70% of speech. As shown in Figure 1, reducing the amplification by only 3-4 dB leads to a reduction of almost 10 dots, or a 10% reduction in speech audibility. This is why, as professionals, we should strive to maintain the gain as close as possible to the prescriptive target, as well as validate the output in the real ear.
Figure 1. The Killion and Mueller Count-The-Dots audiogram for estimating the Speech Intelligibility Index (SII).6 Shown on the chart are representative-aided thresholds for a prescriptive fitting and the resulting aided thresholds when gain is reduced by 3 dB.
As most hearing care professionals know, fitting to the prescriptive target is not always accepted by the user—especially a new hearing aid wearer. The wearer’s own voice is often perceived as metallic, tinny, loud, or unnatural. One common solution is to lower the frequency-specific and level-dependent gains until the patient’s own voice sounds more natural. Considering the “Count-The-Dots” audiogram in Figure 1, it’s easy to see the disadvantage of this approach with respect to speech audibility. In fact, it often is necessary to lower gain more than 3 dB to solve the “own-voice” problem, causing an even greater audibility deficit.
Trade-offs in Open Fittings
Improvements in feedback canceling systems have made it possible to fit more people with open-fit systems. While reducing occlusion usually provides more comfort, the open fit has its natural downside as well. First, it’s recommended for people with near-normal, low-frequency hearing, since the acoustic seal is not closed enough for substantial low-frequency amplification. Secondly, as mentioned, many own-voice problems of “tinny” and “not natural” are caused by high-frequency gain, which essentially is the same in open fittings as in closed. Finally, the great advantages of modern binaural beamforming, directional microphones, and noise reduction technologies are diminished with an open fitting. In noisy environments, the external sound going directly into the ear canal masks the filtered “cleaned-up” signal from the hearing aid, thereby reducing the effect found in more closed fittings. Up to 1500?Hz, the direct sound in an open-fitted hearing aid usually dominates the result. In other words, the hearing aid’s signal processing has little or no influence up to this frequency.7 So there are obviously good reasons to approach better sealing of the ear canal, especially for those struggling in environments with background noise.
Listening Comfort and Satisfaction
With a high amount of open fittings, we might expect people to be quite satisfied with their own voice. Are there data to support this?
To answer this question, we conducted a survey of hearing aid users who had acquired new hearing aids in the past 3.5 years. The survey was conducted in both the United States and Germany, with a total of 384 participants, 78% of them being experienced users (>2 years of usage). The participants were asked to self-rate their hearing loss. A total of 46% of them reported their hearing loss as mild to moderate, and 39% as severe to profound (the remaining 15% answered “unknown”). The participants also rated their satisfaction on a 5-point scale (1=Very Dissatisfied to 5=Very Satisfied). The somewhat surprising result was that only 41% were satisfied with the sound of their own voice.
This is a high dissatisfaction rate, considering that the patients who were surveyed had been through follow-up adjustments and the majority were experienced users. The results indicate that occlusion and/or the occlusion effect is not the only issue related to own-voice satisfaction. Negative perceptions of own voice are still reported by a large number of open-fit hearing aid users.
The Solution
The Signia Nx, the latest generation of hearing aids from Signia, directly addresses the own-voice problem. With a new technology called Own Voice Processing (OVP), the wearer’s own voice is detected and processed separately, while external sounds remain unaffected.8 This means that, whenever the wearer is speaking, the hearing aids detect the situation and apply a dedicated setting different from when only external sounds are present. In this way, the general gain setting for speech understanding remains untouched and the own-voice issue can be dealt with separately by the new OVP technology. Using this technology, the hearing care professional no longer has to compromise by lowering gain—and therefore audibility—to accommodate own-voice problems.
To have two separate gain strategies, it is necessary to have a very fast system that is smart enough to differentiate when the wearer is speaking versus when someone else is speaking. In the new Signia hearing aids, this is accomplished by training the hearing aids to recognize the wearer’s voice, which requires about 10 seconds of live speech from the user while wearing the hearing aids. The hearing aids “scan” the acoustic path of their own placement relative to the wearer’s mouth (Figure 2). Based on this analysis, the hearing aids are able to detect when speech is coming from the wearer versus his/her surroundings, even if speech is coming from a conversation partner situated directly in front of the wearer. Additionally, if the wearer’s voice changes for some reason, the detection remains precise, because it scans the unique sound propagation pattern as sound travels from the wearer’s mouth to the hearing aid microphones, rather than the frequency characteristics of the wearer’s voice.
Figure 2. When fitting Signia Nx, the hearing aids will run an acoustic “scanning” where the acoustic path of the user’s voice is calculated. The wearer’s head shape and mouth placement relative to the hearing aids is part of the sculpturing to create an accurate detection.
Research Evidence
In a study conducted at Hörzentrum in Oldenburg, Germany, this new OVP technology was clinically investigated. There were 42 participants with bilateral sensorineural hearing loss (PTA = 48.4 dB HL) fitted binaurally with Signia Nx hearing aids using the Nx fitting rationale. They were asked to make judgments regarding their perception of the sound of their own voice. Without OVP activated, 20 of the 42 subjects (48%) were dissatisfied with their own voice, stating it sounded muffled, metallic, reverberant, too loud, or unnatural. After applying Own Voice Processing (OVP) to the “unsatisfied group,” 75% experienced a noticeable improvement in their own-voice quality. Thereby, an increase in the total number of subjects satisfied with their own voice improved from the initial 52% (22/42) to 88% (37/42). For these wearers, they could now benefit from the full potential of the hearing aids without being troubled with an unnatural, disturbing own-voice processing or reduced amplification (Figure 3).
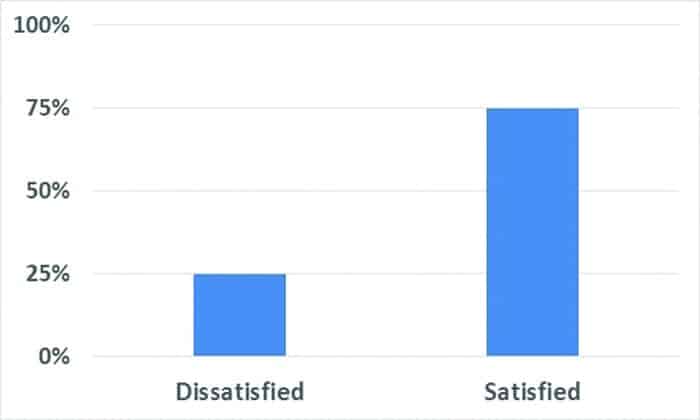
Figure 3. A total of 15 of 20 previously dissatisfied participants (75%) were satisfied with their own voice after applying the OVP feature.
In a second study, also conducted at Hörzentrum Oldenburg, 32 participants (PTA=51.8 dB HL) were given the option in the lab to experience the hearing aids both with and without OVP during various tasks of listening to their own voice. The participants were divided into three groups with different acoustic couplings: 10 people were fitted with open domes, 11 with closed, and the remaining 11 with vented domes. After the lab trial, the participants chose their preferred setting. Only 5 (15%) preferred the “Off” setting for OVP (Figure 4).

Figure 4. Shown are the percent of participants who chose to have OVP on or off. When making judgements concerning their own voice, 25 of 32 subjects (78%) preferred to have the OVP function activated after lab trial.
As most clinicians know, making hearing aids sound more comfortable for the wearer’s voice is not, in itself, a difficult task. By simply turning down the amplification enough, most people will find the sound comfortable. The big difference with OVP technology is that it does not have any effect on the amplification for any “external” sounds, including speech from conversation partners. The system simply reacts when the wearer is speaking. As previously discussed, this allows the user to maintain the amplification required for optimum audibility, without the compromise of reducing amplification for own-voice comfort.
Summary
To encourage people to talk and stay active, we should strive to give them the advanced amplification they need, and, most importantly, not compromise on audibility or limit the advanced noise-reduction algorithms. By providing sufficient gain and increasing spontaneous acceptance, people are less likely to place their hearing aids in the drawer or return them, and more likely to participate actively in social activities. The Signia OVP technology is designed to help people adapt to their hearing instruments more easily, provide them with sufficient amplification, and better equip them for a socially active life.
Correspondence can be addressed to HR or Eric Harry Høydal at: [email protected]
Original citation for this article: Høydal EH. A new own voice processing system for optimizing communication. Hearing Review. 2017;24(11):20-22.
References
-
Leigh-Hunt N, Bagguley D, Bash K, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. November 2017; 152:157-171.
-
Kuiper JS, Zuidersma M, Oude Voshaar RC, et al. Social relationships and risk of dementia: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Research Reviews. July 2015; 22:39-57.
-
Hornsby BWY. The effects of hearing aid use on listening effort and mental fatigue associated with sustained speech processing demands. Ear Hear. 2013;34(5):523-534.
-
Lin FR, Yaffe K, Xia J, et al. Hearing loss and cognitive decline among older adults. JAMA Intern Med. 2013;173(4):293–299.
-
Mueller HG, Killion MC. An easy method for calculating the articulation index. Hear Jour. 1990; 43(9):1-4.
-
Killion MC, Mueller HG. Twenty years later: A NEW Count-The-Dots method. Hear Jour. January 2010; 63(1):10-17.
-
Dillon H. Hearing Aids. 2nd ed. Turramurra, Australia: Boomerang Press; 2012.
-
Signia. Signia OVP feature in brief. 2017. Available at: https://www.signia-pro.com/scientific_marketing/ovp-sound-quality