In this study, various audio and visual communication modalities were examined to identify which communication perspective could best benefit patients during a hearing aid fitting orientation appointment.
By Jonathan Mikhail, EdD, AuD, MS; Samantha Dewey, AuD; Samuel Christensen, AAS-HIS
For patients to get the most out of their hearing aids, it’s important that they understand and remember information related to the use, care, and maintenance of their devices. Therefore, it stands to reason that hearing care professionals (HCPs) would benefit from utilizing the forms of communication most effective for their patients when conveying this important information during hearing aid fitting orientation (HAFO) appointments. This is what our study sought to investigate.
Key Components of HAFO Appointments
Hearing aid fittings are routine for hearing care professionals in audiology clinics. To maintain a clear understanding of the technological and sociocultural evolution of hearing devices, HCPs continually adjust what they include in their HAFO appointments. Standard procedures during HAFO appointments include verifying and performing routine maintenance on devices, removing and reinserting the devices, and utilizing included accessories (e.g., Bluetooth connectivity, television streamers). Other practitioners may conduct additional testing (e.g., aided vs. unaided testing) or provide specialized instructions (e.g., tube changes) that are discussed further during the HAFO appointment.
Previous studies have explored how much information individuals retain at various stages of their hearing aid use, from the initial fitting to one month after the HAFO appointment.1 Adult patients can recall a significant portion of information (74%) upon immediate recall and even more (78%) after retesting a month later, which is linked to the familiarity they gain with the new devices. Furthermore, other studies have identified trends across audiology clinics regarding how hearing care providers conduct HAFO appointments.2 While specific practices are implemented in these clinics, including verification, rechargeable devices, and simple maintenance, the behavioral patterns of practitioners play a crucial role in all HAFO appointments and significantly influence what patients remember afterward.
Avoiding Returns
It is not uncommon for patients to return hearing devices if the HAFO appointment becomes overwhelming. Previous data indicate that hearing aid success derives from validation and verification; however, incomplete HAFO appointments can hinder a patient’s opportunity for validation and diminish the effectiveness of hearing devices in enhancing communication.3 Specific standards have also been developed, including a patient-centered approach to HAFO appointments, ongoing exposure to information related to hearing devices, reusable learning objectives (RLOs), and continued support for hearing devices, such as follow-up appointments.4
Hearing aid manufacturers have sought to alleviate the burden on hearing care professionals during HAFO appointments by incorporating tutorial videos. These videos are often accessible through the patient’s phone application when the patient uses the hearing device’s Bluetooth connectivity feature or can be previewed on an online streaming platform. However, if the patient does not utilize the Bluetooth feature, lacks a compatible phone, or is unfamiliar with streaming tutorial videos, they may not have access to the resources provided by the hearing aid manufacturer.
Study Focus
To understand what HAFO appointments should include, it is essential to consider the types of communication used. To determine the most effective method(s) of communication, this study aimed to evaluate a sample of patients being given instructions under various conditions, including audio-visual, visual-only, and auditory-only communication, to complete the filter change of a hearing device. Additionally, the study sought to determine whether gender or age influenced the outcomes of participants under different communicative conditions.
Methods and Materials
A third party not involved in audiological care pre-recorded a video with clear instructions to assess patients’ ability to retain information from their HAFO appointment. The video and audio guided each participant in changing the wax guard on a specific manufacturer’s receiver-in-the-canal (RIC) hearing aid. Throughout the video, participants received guidance to complete additional tasks, such as unpacking an alcohol swab, using a tissue, and removing or replacing a dome, which was used to monitor their attention during the assessment. Each participant was required to sign a waiver indicating that this was for research purposes only.
To quantify participants’ evaluation completion, they were assessed using the Practical Hearing Aids Skills Test-Revised (PHAST-R).5 The revised scale categorizes scores into a three-point system. In this study, a score of “2” indicated full task completion, encompassing all steps presented in the video and audio. A score of “1” showed that the participant could complete the tasks but required the test administrator to repeat a step, pause the video or audio, or ask additional questions. A score of “0” was assigned if the participant could not complete the task.
Recruitment and Sample Overview
Participants were recruited from a single location: the Area Hearing and Speech Clinic Inc. in Joplin, Missouri. This exploratory study involved 30 participants: 12 females and 18 males. To qualify for the study, participants had to be between 18 and 85 years old and have received their first pair of hearing devices within the past year. Prior to this study, participants had not received instructions on how to change the filter of a hearing device. The brand of hearing device fitted to the participant did not influence eligibility for the study, provided the individual met the other participation criteria.
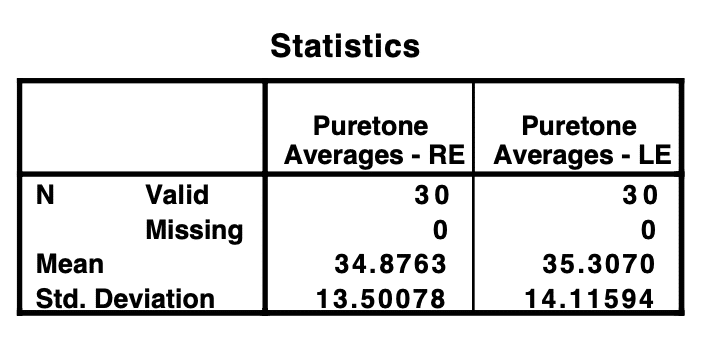
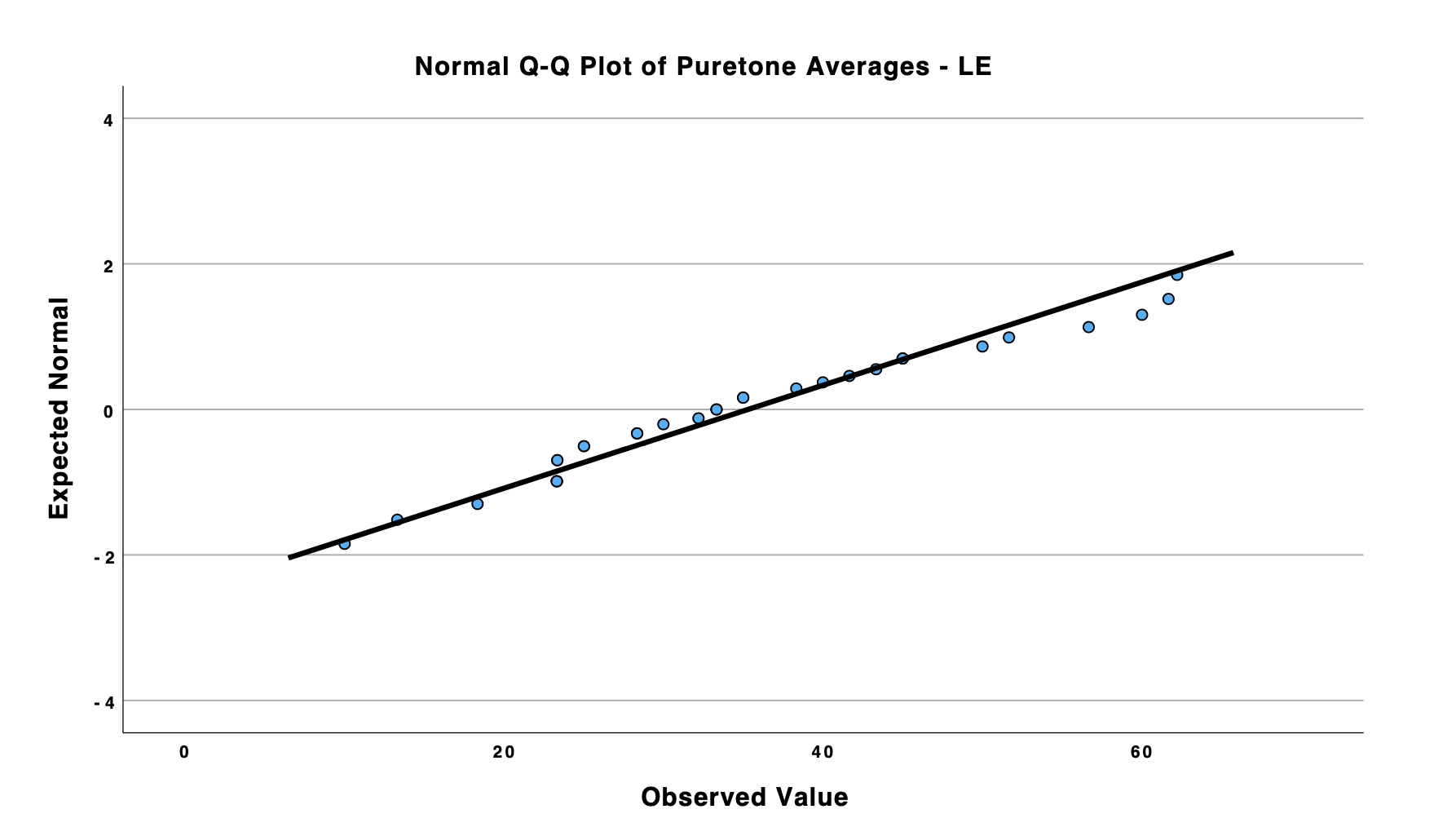
Furthermore, participants were required to confirm that they did not have a diagnosis of arthritis, other dexterity issues, or cognitive impairments that could create variability during the testing process. All participants had to exhibit bilateral, symmetrical, mild to severe/profound sensorineural hearing loss (mean PTAs RE: 34.87; mean PTAs LE: 35.30). Prior to participating in the experiment, all hearing aids were fitted into the participants’ ears.
The participant was seated at a table that closely resembled the visual representation in the pre-recorded video. If the participant was in the auditory-only condition group, the pre-recorded instructor would guide each individual through the supplies. The same hearing healthcare provider arranged the table to ensure consistency among participants, regardless of their assigned group. The prepared table included one tissue, a packaged alcohol wipe, hearing aids from a single manufacturer, and the specific filter used by that manufacturer. Participants with hearing aids from manufacturers not involved in the study were also included. The hearing care professional provided a verbal instruction, directing the participant to follow the modality of the selected group (e.g., audio-visual, visual, or auditory-only).
Data Analyses
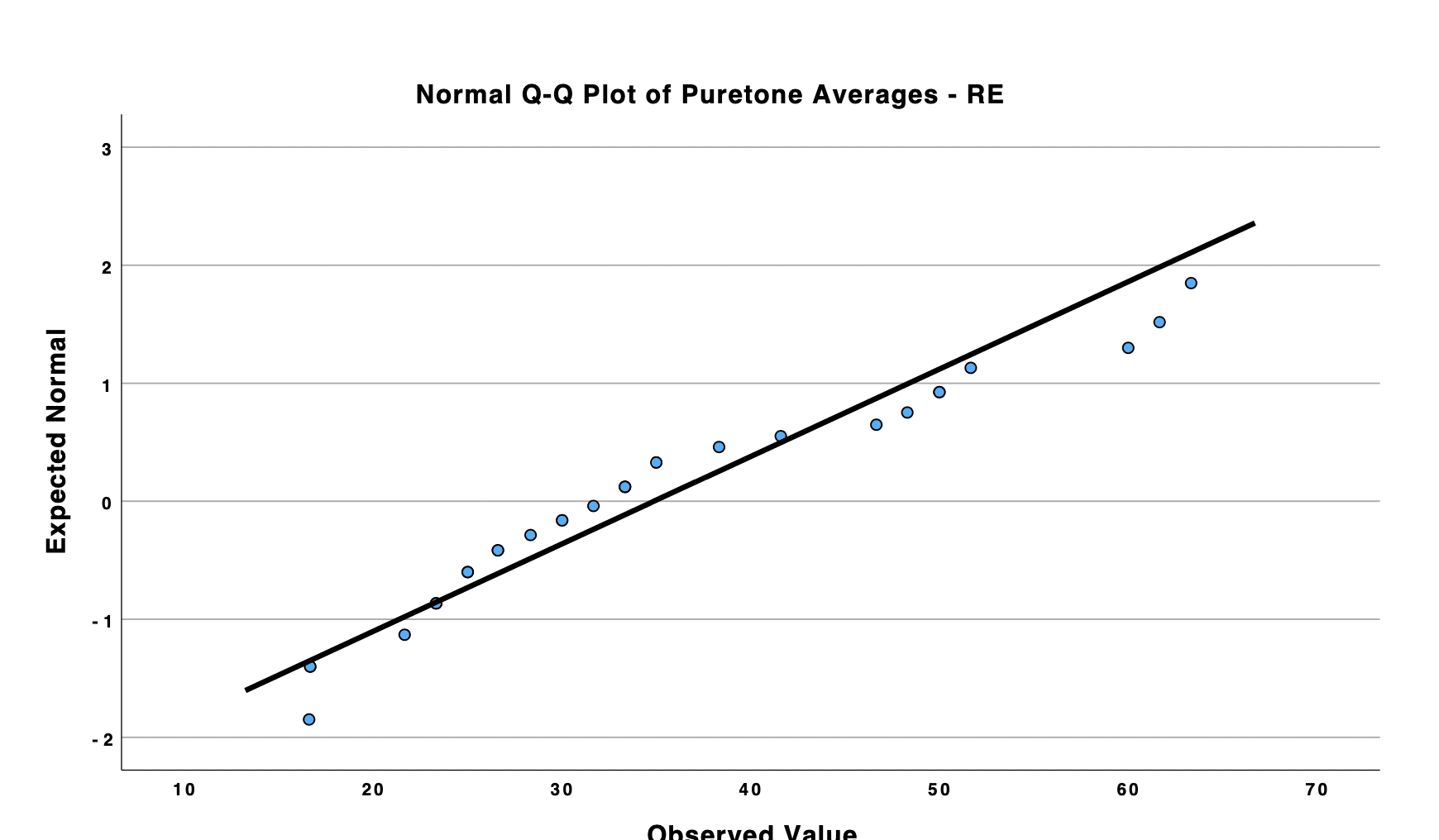
The Kolmogorov-Smirnov (K-S) and Shapiro-Wilk (S-W) tests indicated that the participants’ characteristics followed a normal distribution.
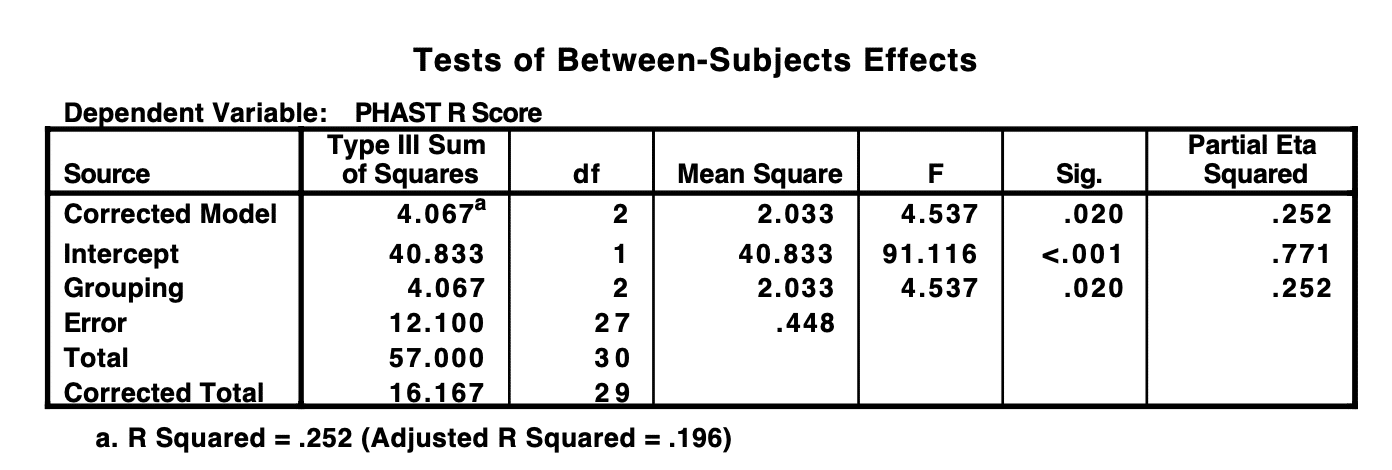
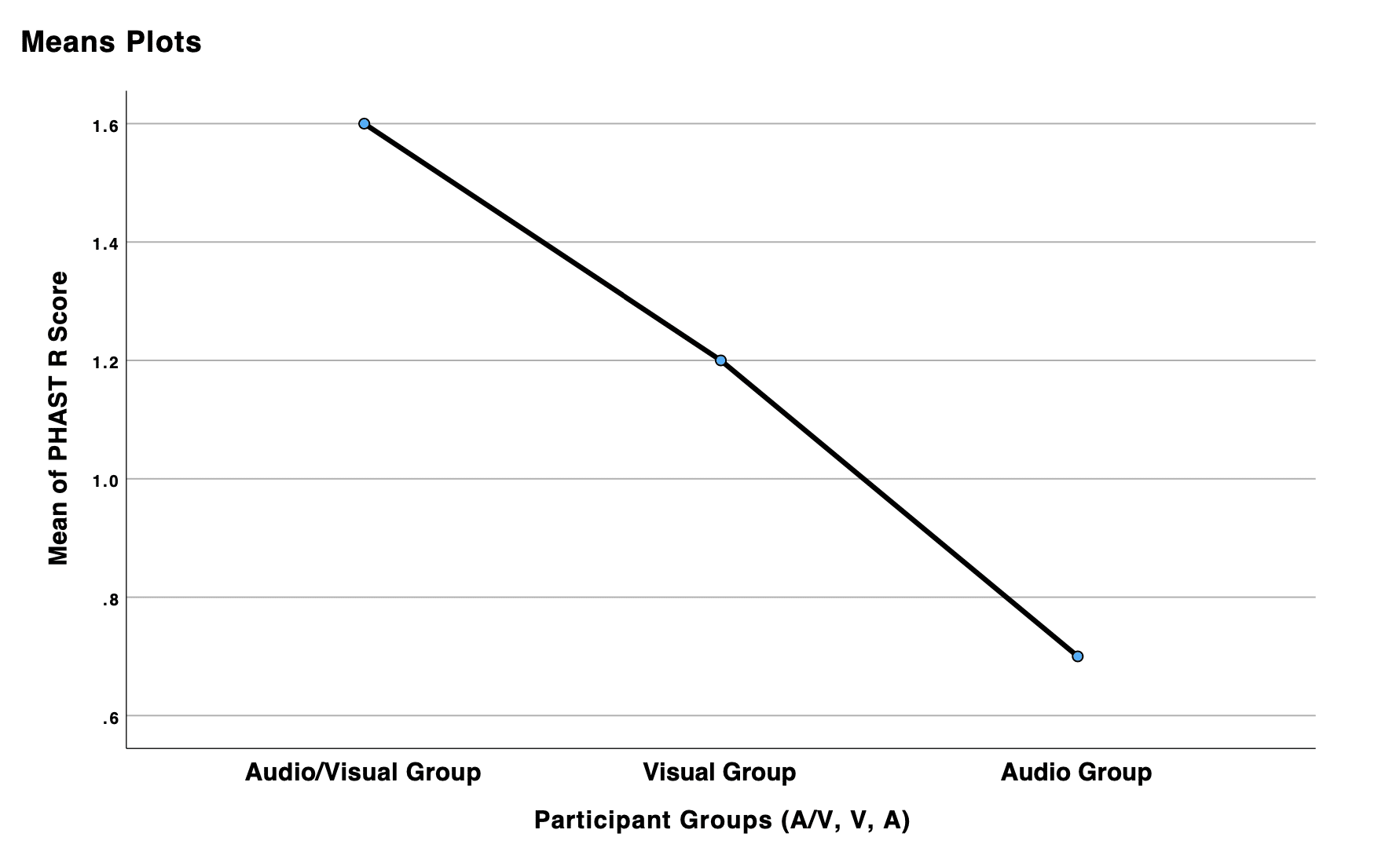
A one-way ANOVA was carried out to analyze the data across all three testing conditions. A clinically significant difference was identified between two of the groups: the audio-visual group and the auditory-only group (p-value = 0.020). However, no clinically significant differences were observed between the audio-visual and visual-only conditions, or between the visual-only and auditory-only conditions (p-value = 0.388; p-value = 0.235). Post-hoc tests also confirmed these results across all groups.
An independent samples T-test was conducted to evaluate whether gender influenced the participants’ results. Statistical analysis indicated that gender did not have a clinically significant impact on the participants’ results (p-value = .207). Additionally, an independent samples T-test was performed to determine if age played a clinically significant role in the experiment’s outcomes. Age was not a factor among all 30 (p-value = .626).
Discussion
This observational study examined the effects of audio/visual, visual, and auditory cues during a HAFO appointment. It found that participants who utilized audiovisual cues, as opposed to auditory-only cues, demonstrated a clinically significant improvement in their ability to complete tasks during a HAFO appointment. While a difference was noted between the audio/visual and auditory-only groups, no statistical difference was identified between the visual-only group and the other conditions explored in this study.
In this pilot study, gender differences were examined to determine whether sex influenced task completion across various communicative conditions. No significant gender-related differences were found among the 18 males and 12 females participating in the study. Age was also considered. While the age range for the observational research spanned from 18 to 85, the participants were aged between 23 and 83, and none had known issues with dexterity or mental acuity at the time of participation. Of the 30 participants, age did not have a clinically significant impact on task completion, regardless of the communicative condition.
Recommendations
As hearing aids evolve into more complex medical devices, HAFO appointments should also adapt accordingly. Audiology has consistently embraced evolution and adaptation, and HAFO appointments are no exception. While fundamental trends define HAFO appointments, such as verification, aided versus unaided testing, cleaning and maintaining devices, recharging capabilities, and Bluetooth connectivity, numerous studies have shown that no single standard has emerged.2,4 RLOs are crucial for patients to retain the information received during HAFO appointments.
Studies like this one highlight the importance of improved HAFO protocols and standards throughout audiology. This research did not aim to dictate what should or shouldn’t be used in HAFO appointments; rather, the data suggested that various communication methods could help participants retain information, thereby saving hearing care professionals valuable clinical time during follow-up appointments.
If clinics begin to consider the information presented in this observational study, a clinic-focused approach to HAFO appointments with specific standards can be established for each hearing care professional in the clinical setting to ensure consistent care for all hearing-aid-wearing patients.
Furthermore, if clinics adopt HAFO standards for hearing device users, these standards, whether written or digital, should be available in multiple languages to serve patients from all ethnic backgrounds. As communication science clinicians, HCPs should implement HAFO standards that address the needs of the general population, including terminology that is accessible and easily understood by laypeople. This should encompass both pediatric patient demographics and the guardians of children fitted with hearing devices.
Hearing care professionals should consider the aging population and identify which modes of communication will be most effective for this demographic. This is particularly significant for individuals with caretakers, those residing in assisted living facilities or nursing homes, as well as those with cognitive impairments and other dexterity challenges. HAFO resources should be customized for this population to ensure consistent care and security in patients’ ability to use hearing devices effectively, including whether the individual has others providing routine at-home maintenance for their hearing devices.
Lastly, incorporating audio and visual cues in HAFO appointments can benefit patients, HCPs, and clinics. This creates a standard for HAFO appointments while giving patients practical information to take away and practice with their hearing devices outside of the clinical setting. Patients can begin developing questions for follow-up appointments to enhance their skills and learn more about hearing devices, how they function, and the mechanisms of the devices.
About the Authors:
Jonathan Mikhail, EdD, AuD, MS, is an audiologist and health scientist at the Area Hearing & Speech Clinic in Joplin, Missouri, and an adjunct faculty member in the Doctor of Audiology program at Wichita State University. He also serves as the director of the audiology residency program at the Area Hearing & Speech Clinic.
Samantha Dewey, AuD, is a senior clinical and vestibular audiologist at the Area Hearing & Speech Clinic in Joplin, Missouri.
Samuel Christensen, AAS-HIS, is a clinical hearing instrument specialist at Area Hearing & Speech Clinic in Joplin, Missouri.
References
1. Reese JL, Hnath-Chisolm T. Recognition of hearing aid orientation content by First-Time users. Am J Audiol. 2005;14(1):94-104. doi:10.1044/1059-0889(2005/009)
2. Barker F, Mackenzie E, De Lusignan S. Current process in hearing-aid fitting appointments: An analysis of audiologists’ use of behaviour change techniques using the behaviour change technique taxonomy (v1). Int J Audiol. 2016;55(11):643-652. doi:10.1080/14992027.2016.1197425
3. Jorgensen LE. Verification and validation of hearing aids: Opportunity not an obstacle. J Otol. 2016;11(2):57-62. doi:10.1016/j.joto.2016.05.001
4. Phelan J, Lee JJ. Hearing aid fitting orientation and the APSO standard. Semin Hear. 2022;43(2):094-098. doi:10.1055/s-0042-1748875
5. Doherty KA, Desjardins JL. The Practical Hearing Aids Skills Test—Revised. Am J Audiol. 2012;21(1):100-105. doi:10.1044/1059-0889(2012/11-0019)
Featured image: Dreamstime