Tech Topic | January 2022 Hearing Review
By Robert M. Traynor, EdD, MBA, FNAP
Practice differentiation is one of the most effective defensive methods available to the independent practitioner, and offering custom hearing aids, earmolds, and plugs is probably the one of the easiest and most effective ways to further differentiate your hearing care practice. Here’s how you can easily do this.
In a seemingly short time, the hearing industry has evolved through a series of stages into a developed industry. Developed industries are those that have evolved through horizontal and vertical integration. Horizontal integration (Figure 1, top) is when the companies buy up smaller, less efficient companies to gain access to their products, patents, engineering capabilities, personnel, or markets. Vertical integration (Figure 1, bottom) is when companies buy up supplier companies so that they can always obtain components for their products and keep the manufacturing process functioning without any difficulties or delays in supplies for their products.
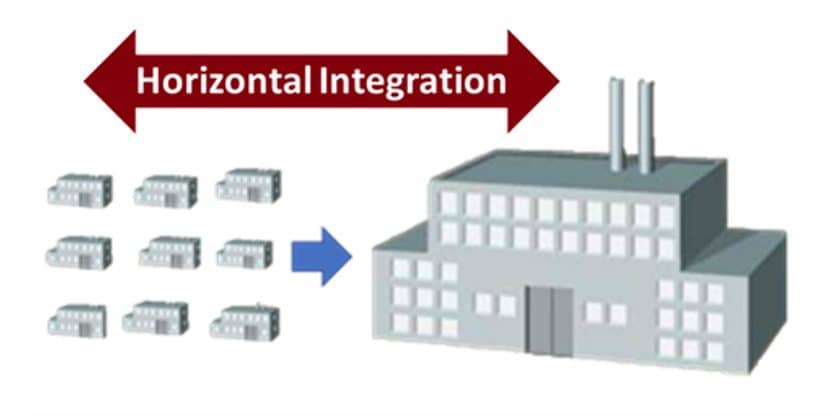
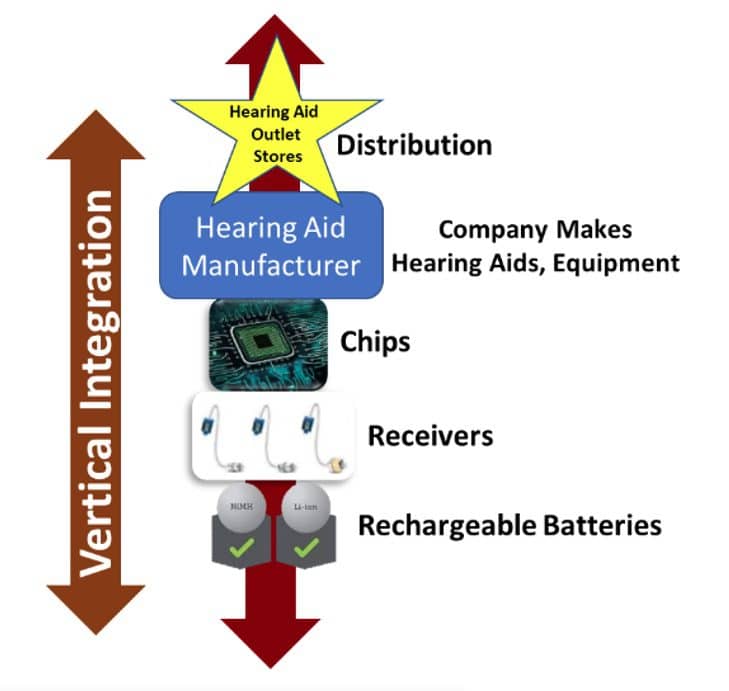
Figure 1. Horizontal integration versus vertical integration.
As part of vertical integration, companies also work to manipulate control of the distribution of their products to present them for sale directly to the consumer, increasing their profitability. While many industries begin with an altruistic orientation, as these businesses develop their vertical integration, they become more of a corporate machine with interests that compete with their legacy customers. As a side result, we also see the power in hearing care practices shifting from the practitioner/provider to the consumer who now has more choices for product acquisition than ever before.
Although it may seem like this development occurred overnight, industry development actually occurs slowly over time. The result of hearing industry development through these integrative movements are big-box stores, manufacturers owning their own retail operations, direct-to-consumer (DTC) marketing, and other strategies that allow manufacturers to maximize their profits—often placing themselves in direct competition with their traditional customers, the independent hearing care professionals (HCPs).
HCPs now work in a developed industry. So, how can they successfully compete in it?
Key Elements of Practice Differentiation
Practice differentiation is one of the most effective defensive methods available to the independent practitioner. Differentiation is a strategy that seeks to present the practice as unique in its market, offering a dimension or dimensions that are widely valued by consumers.
Porter1 indicated that technology has a serious impact on the differentiation of a business, its role, and its product in the consumer’s value chain. He also stated that clinics achieving and sustaining this market differentiation will perform at a significantly higher financial level than those that do not differentiate.
While many independent practices already offer significant value to consumers, here are some key added benefits from a differentiated practice that can be viewed as most valuable to consumers:
- Unique product configurations, performance, and features;
- A variety of products and product accessories offered;
- The level of professional service, best practices, and technology used to provide these products;
- The delivery time to obtain these products.
- The atmosphere in which the products are provided.
- Convenient procedures for scheduling initial and follow-up appointments.
- On-site repairs/maintenance, and a variety of options for financing, warranties, and other services.
While most independent practices strive to achieve these goals, consider that the reintroduction of custom products—especially deep-canal instruments—meet almost all of Porter’s criteria. Custom products are a product configuration unique to every patient. In the deep-canal format, they are essentially a stigma-proof invisible configuration offering substantial performance benefits.
Consumers perceive that devices designed according to the size and shape of their ear and configured for their individual hearing loss are a “special” part of the hearing rehabilitative process conducted just for them. With technology-reduced delivery time offered in a professional atmosphere, reintroducing custom instruments—especially the deep-canal versions—certainly differentiates an independent hearing care practice.
Following Porter’s logic, Amlani et al2,3 contends that independent hearing care practices are the highest cost providers; thus, as expensive providers they must offer the highest, unexpected value to consumers to be successful.4 At a time when most of the proposed over-the-counter (OTC) and/or DTC products appear to be receiver-in-the-canal (RIC) or a modular in-the-ear (MITE) style, differentiation by product style and technology type provide for this unexpected value.
Reintroduction of Custom Products
Differentiating a practice around the availability of custom hearing devices, especially deep-canal fittings such as CIC/IIC, sets a hearing healthcare practice apart from the stores and other clinics in the marketplace offering RIC devices that all look the same with no custom design around the patient. Working to achieve the best hearing result by catering to cosmetically sensitive consumers is now a differentiation technique whose time has resurfaced to the advantage of clinicians.
There was a time in the not-so-distant past when custom products made up the major portion of hearing aid styles sold in the United States (Figure 2). Some custom styles, however, such as in-the-ear full shell (ITE), in-the-canal (ITC), and their variations, have lost their luster due to size and visibility since their 1990’s heyday. ITE and ITC hearing aids constituted 81% of the 1991 US hearing aid market and traditional behind-the-ear (BTE) hearing aids made up the rest of the market at 19%.5 For many reasons—not the least of which are visibility, enhanced technology, and personal preference—current sales data supports the market dominance and popularity of RIC products at the expense of traditional custom devices in the full-shell to mini-canal ITE styles. While CIC and IIC instruments are still desirable for many patients, long-standing fabrication issues continue to haunt clinicians, manufacturers, and their patients, shrinking their sales each year.
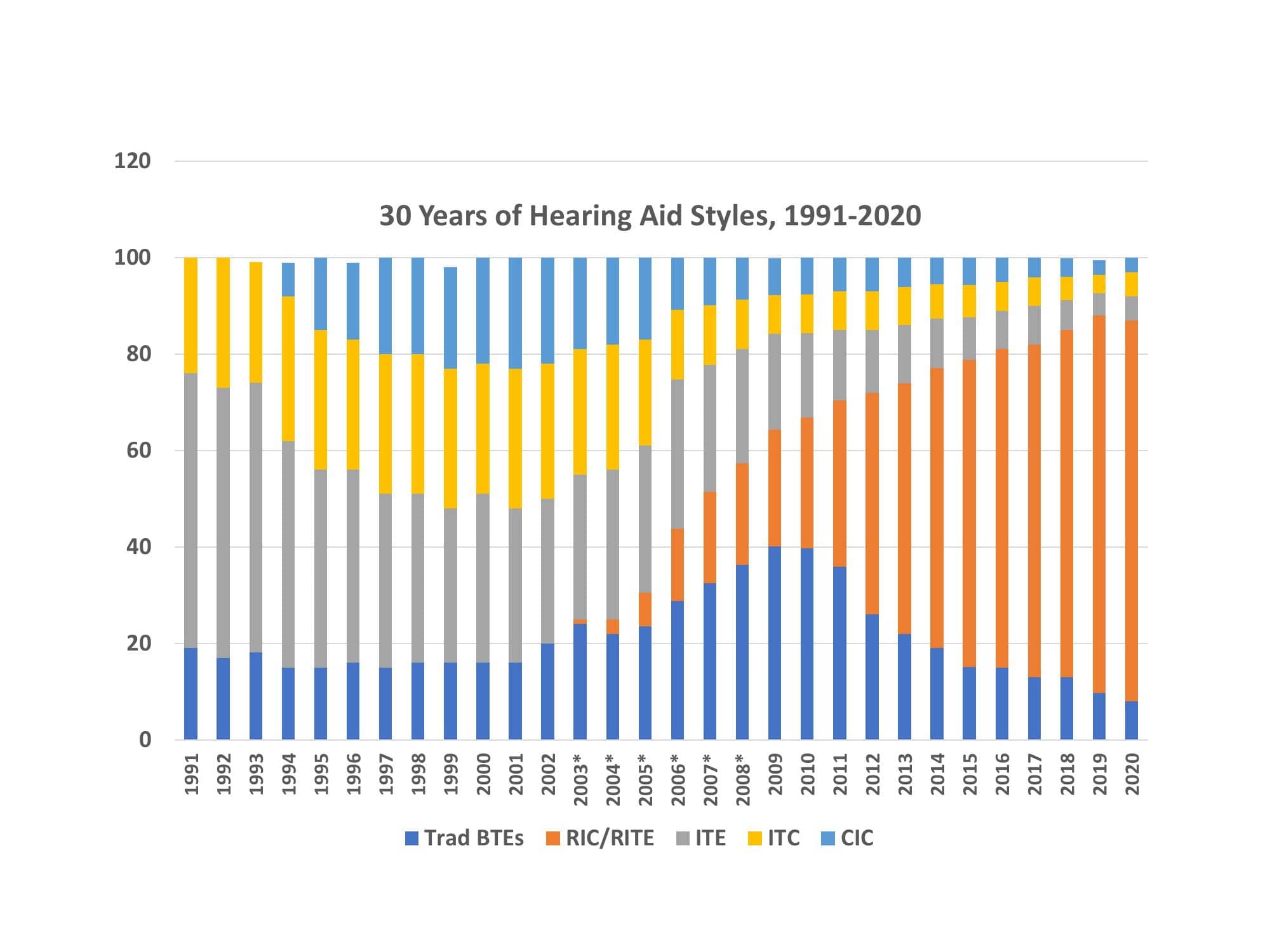
Figure 2. Trends in hearing aid styles as drawn from Hearing Industry Association statistics and HR estimates.5
Strom,6 in his yearly inventory of hearing aid unit sales, reported that in 2020 only 13% of the total US hearing aid market was custom devices and, within that figure, deep-canal devices (CIC and IICs) with the most potential for practice differentiation, were only 3% of the total market (Figure 3). Of course, some of this reduction in custom devices in 2020 is likely due to the reluctance of patients to visit clinics during the pandemic, especially for close personal procedures such as ear impressions.

Figure 3. Use of hearing aid styles in 2020. From Strom, 2021.6
While RIC devices offer an ease of fitting and follow up never seen before, the nearly exclusive use of these products have both advantages and limitations. A practice routinely using RIC devices can be stocked, taking less acquisition and fitting time, as well as virtually no modification during and after the original fitting. For many hearing losses, the best fittings are with RIC devices, but certainly not every fitting—and almost certainly not for 80% of all patients. By not utilizing custom products (which can also include custom earmolds for RICs), hearing healthcare practices are failing to stand out in the crowded market of big box stores, DTC marketing, internet retailers, manufacturer retailers, drugstores, and other distribution points vying for the hearing aid marketplace with dome-fit RIC devices.
While limited in their Bluetooth capability, a practice that designs a program to offer invisible, well-fit CIC and IIC devices sets their clinic apart from the myriad of RIC products on the market, particularly for cosmetically sensitive first-time users.
Patient Advantages from Deep Canal Fittings
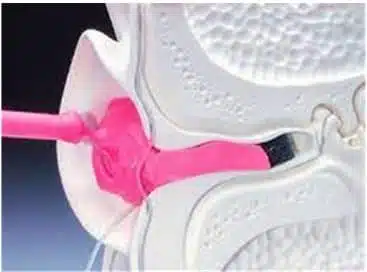
By definition, a deep-canal hearing aid offers a microphone recessed into the ear canal and positions the medial tip of the shell past the second bend into the osseous (bony) portion of the ear canal extremely close to the eardrum. Branda7 summarized several benefits derived from well-fit deep-canal hearing aids, including:
1) Increased gain and output;
2) Diminished occlusion effect;
3) Reduced acoustic feedback, and
4) Maintained directionality.
Van Vliet and Galster8 indicated in their study comparing BTE and CIC/IIC fittings that deep-canal microphone placement improves sound quality when compared to BTE and CIC hearing aid fittings. Likewise, front-to-back localization ability is improved with IIC and CIC hearing aids when compared to BTE hearing aids. They further stated that correctly fit deep-canal hearing aids, such as the IIC, offer patients a customized invisible hearing solution that leverages the unique acoustic benefits of the pinna and ear canal. These are distinct, natural advantages over RIC devices. Several studies in the last 25 years have looked at the proven benefits of CICs and IICs.9
All these well-documented benefits from a unique product class that is difficult to dispense outside the professional channel—and yet CICs are currently used only 3% of the time in hearing aid fittings. If these products are to be reintroduced into today’s market, the obvious question is: What caused their waning popularity in the first place?
Clinical Issues with Deep-canal Hearing Aid Fittings
Although most seasoned clinicians realize the advantages of the deep-canal devices, they also remember that CIC/IIC products have historically had fitting, remake, and return issues at levels that arguably created much of their demise. Clinician error in taking traditional ear impressions has been identified as a major problem with the fabrication of these devices, creating guesswork for the shell lab technicians during the fabrication process.
In many clinics, particularly those not used to taking traditional deep-canal impressions, there is often a “tradeoff” between comfort and performance. When a deep-canal impression is of concern, the manufacturer usually requests a new ear impression, which may be better or worse than the existing impression due to provider error. The fabrication tradeoff is usually an educated guess, choosing between comfort or performance based upon many factors, none of them scientific. If comfort is chosen, often performance is lacking with greater chance of feedback due to microphone placement, length, receiver angles, and other important fitting issues; if performance is chosen, it may be uncomfortable in its extension into the isthmus of the canal and/or other areas. Either of these concerns can lead to higher incidence of modifications, remakes, and/or returns.
In the beginning history of CIC hearing aids (circa 1992-1993), clinicians have horror stories involving the early liquid silicone “deep-canal” impressions. While these impressions offered detail and length, even in specially trained hands the removal process was delicate, sometimes painful to the patient, and even dangerous. Eventually, better silicone impression materials became available, and the use of these new materials have evolved into our current “deep-canal ear impression techniques” (eg, see Chester Pirzanski’s series of articles at HearingReview.com). When the process is conducted properly, it accurately captures ear canal characteristics well into and often past the isthmus.
The process does require unusual attention to block placement.7,10,11 If not placed with care, it’s possible for impression material to migrate farther into the canal, causing issues with removal. Even with today’s advanced silicone impression material, removal problems, canal detail, canal length, and isthmus abrasion issues still complicate the fabrication process. A perfect deep-canal impression (Figure 4) presents the essential information regarding size, shape, length to manufacturers to fabricate a comfortable, high performance, deep-canal product with no occlusion or feedback issues. As indicated earlier, since the ear canal is dynamic12 and most deep-canal traditional silicone ear impressions regularly present imperfections in length, canal, and isthmus detail, manufacturers often must guess about fabrication details. These fundamental impression problems are well documented in the literature as well as the archives of manufacturer returns for credit, significantly contributing to the decreased popularity of these valuable deep-canal products.
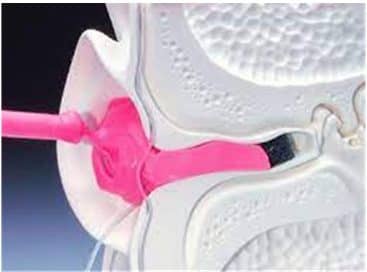
Figure 4. A “perfect impression” using silicone and traditional impression-taking techniques remains one part skill and technique, and one part art.
The Cure for the Fabrication Problem of CIC/IIC Devices
Business scholars agree that technology has a large impact on business differentiation and represents a key determinant in consumer-perceived value. There is now new technology available to facilitate the fabrication of custom products and virtually eliminate the problems discussed above.
Although an initial investment in business differentiation, a system like the Otoscan 3D digital ear scanner becomes a reasonable choice in overcoming the issues associated with CIC/IIC product fabrication and reintroducing them into your practice. These virtual impressions can be taken in half the time with more ease, safety, and precision, alleviating the necessity for modification, remakes, and returns for either comfort or performance issues. Now the best of both worlds is available through the ultimate accuracy of 3D digital ear scanning.
Over the years, 3D digital scanning has been applied for many procedures in medicine and dentistry, but the ear has remained uncharted territory due to its size, shape, and the types of surfaces to be scanned. There have been challenges in scanning the ear for the data acquisition systems to assess all surfaces for size and shape from the full pinna to past the second bend of the ear canal and as far as 4 mm from the tympanic membrane.
The digital ear scanner not only results in better-fitting custom hearing aids, but also for earmolds and custom receiver tips for RIC devices. The use of this 3D digital scanning process brings ear impression technology from the 1950s into the 21st century with a technique circumventing traditional deep-canal imperfections by reducing provider error and removing potential medico-legal problems related to impression material.13 Further, in assessing patient candidacy for these deep-canal fittings, the Otoscan 3D digital ear scanner has the capability to consider the status of the dynamic ear canal’s temporomandibular joint, canal elasticity, and other salient factors that are not available from even the best traditional deep-canal impression.
As we move to a post-pandemic economy, hearing care practice owners and clinicians in a highly competitive market should consider the following issues to differentiate their practice by product and technology:
- OTC, DTC, online, and competitive hearing aids from big-box and manufacturer-owned stores are mostly of the RIC type, and CIC/IIC hearing aids offer differentiation to independent clinics.
- Stigma is still a significant reason for first-time users reluctance to adopt hearing aids. CIC/IIC products are an inroad for cosmetically conscious consumers seeking a variety of options.
- When custom devices have been fabricated with the precision of a scanner, less modifications may be required, and better performance can be expected.
- Rechargeable custom products are now entering the market which will eliminate the issue of low battery life for these instruments.
No matter how much hype and popularity RIC products have received over the past few years, not all patients prefer them; instead, they have accepted them as a necessity (or perhaps “necessary evil”) to achieve their goal of better hearing. Companies offering DTC devices have found that patients still appreciate the cosmetics of invisible CIC hearing aids—even if the devices are not custom fit and sacrifice comfort. We should own this market.
Summary
There have been substantial, but predictable, changes in the hearing industry over a prolonged period resulting in both horizontal and vertical integration. Along with other events and evolving technology, this has created a highly competitive market for independent audiology practices. Differentiation is fundamental to success, and 3D digital ear scanning technology offers a new solution to widen success in the fabrication of deep-canal hearing aids by eliminating the deep impression dilemma (ie, tradeoffs in comfort and performance). Ear impressions in the 21st century should be accomplished through ear scans—an important technology to incorporate into practice that provides efficiency, reduced remakes, creates a true reproduction beyond the isthmus of the ear canal, enhances safety standards, reduces impression material waste in addition to product waiting time, while greatly enhancing the overall patient experience.
Laja14 contends that “sameness” is the combined effect of companies being too similar in their offers, poorly differentiated in their branding, and indistinct in their communication; the language they use is vanilla, the products/service offerings are like any other, and the marketing message is identical to that of their competition. The Otoscan 3D digital ear scanner helps eliminate this sameness and differentiates a practice from all others in the market, opening the door for offering ease-of-fit CIC/IIC products for the cosmetically sensitive patient.
CORRESPONDENCE to Dr Traynor at: [email protected].
Citation for this article: Traynor RM. Practice differentiation by reintroducing custom hearing products. Hearing Review. 2022;29(1):20-24.
References
- Porter ME. On Competition. 2nd ed. Harvard Business Review Press;2008.
- Amlani AM, Taylor B, Levy C, Robbins R. Utility of smartphone-based hearing aid applications as a substitute to traditional hearing aids. Hearing Review. 2013;20(12):16-23.
- Amlani AM, Smaldino J, Hayes D, Taylor B, Gessling E. Feasibility of using a smartphone-based hearing aid application to improve attitudes toward amplification and hearing impairment. Am J Audiol. 2019;28(1):125-136.
- Traynor R. Are you ‘clued-in’ to offer the ultimate patient experience? Hearing Review. 2019;26(7):25-27.
- Strom K. A brief history of hearing aid styles: 1991-2020. Hearing Review. https://hearingreview.com/hearing-products/hearing-aids/a-brief-history-of-hearing-aid-styles. Published June 4, 2021.
- Strom K. Hearing aid sales fall by 18% in 2020. Hearing Review. https://hearingreview. com/practice-building/marketing/surveys-statistics/ hearing-aid-sales-fall-by-18-in-2020. Published January 18, 2021.
- Branda E. Deep canal fittings: Advantages, challenges, and new approach. Hearing Review. 2012;19(4):24- 27.
- Van Vliet D, Galster JA. Invisible in-the-canal hearing aids. Starkey White Paper. https://starkeypro.com/pdfs/technical-papers/WTPR0008-00-EE-ST.pdf. Published 2010.
- Kochkin S. Customer satisfaction and benefit with CIC hearing aids. Hearing Review. 1995;2(4):16-26.
- Crowhen D. An innovative otoblock that enables deeper impression taking. Hearing Review. 2017;24(11):24-28.
- Garcia H, Staab W. Solving challenges in deep canal hearing aid fittings: Parts 1. Hearing Review. 1995;2(1):34-40.
- Oliveira R, Babcock M, Venem M, Hoeker G, Parish B, Kolpe V. The dynamic ear canal and its implications. Hearing Review. 2005;12(2):18-19,82.
- Traynor RM. Medico-legal considerations with 3D digital ear scanning. Hearing Review. 2021;28(6):20- 22.
- Laja P. Differentiation strategy: What it is, why it’s critical, and how to get it right. CXL website. https://cxl.com/blog/differentiation-strategy/. Published June 2, 2020.