Tech Topic | November 2017 Hearing Review
A new otoblock has been designed to provide deeper impressions with greater comfort and safety. This field study compares impressions taken with the new EasyView OtoBlock (EVOB) to standard otoblocks.
Individual ear anatomy is unique (Figure 1).1 Therefore, it is vital for ear impressions to capture full information of the pinna and external auditory meatus extending past the second bend to enable optimal custom hearing solutions to be crafted.2

Figure 1. The individuality of ear anatomy.
Standard otoblocks are made from materials, such as cotton wool and foam, which are opaque, providing the clinician with no information past their medial tip during placement, especially regarding canal direction and distance from the eardrum.
The EasyView OtoBlock (EVOB) is a new innovation designed to support deeper impression taking. It utilizes a hollow symmetrical seal and has an angled window at the end, enabling visualization of the canal and eardrum beyond the medial tip of the OtoBlock during placement using an otoscope (Figure 2). Its hollow vent tube also mitigates any pressure vacuum, improving comfort during removal. Additionally, because the symmetrical seal of the EVOB has a cavity, it fills with impression material, expanding against the canal wall and becoming part of the ear impression—providing useful information for shell modeling and production (Figure 3).
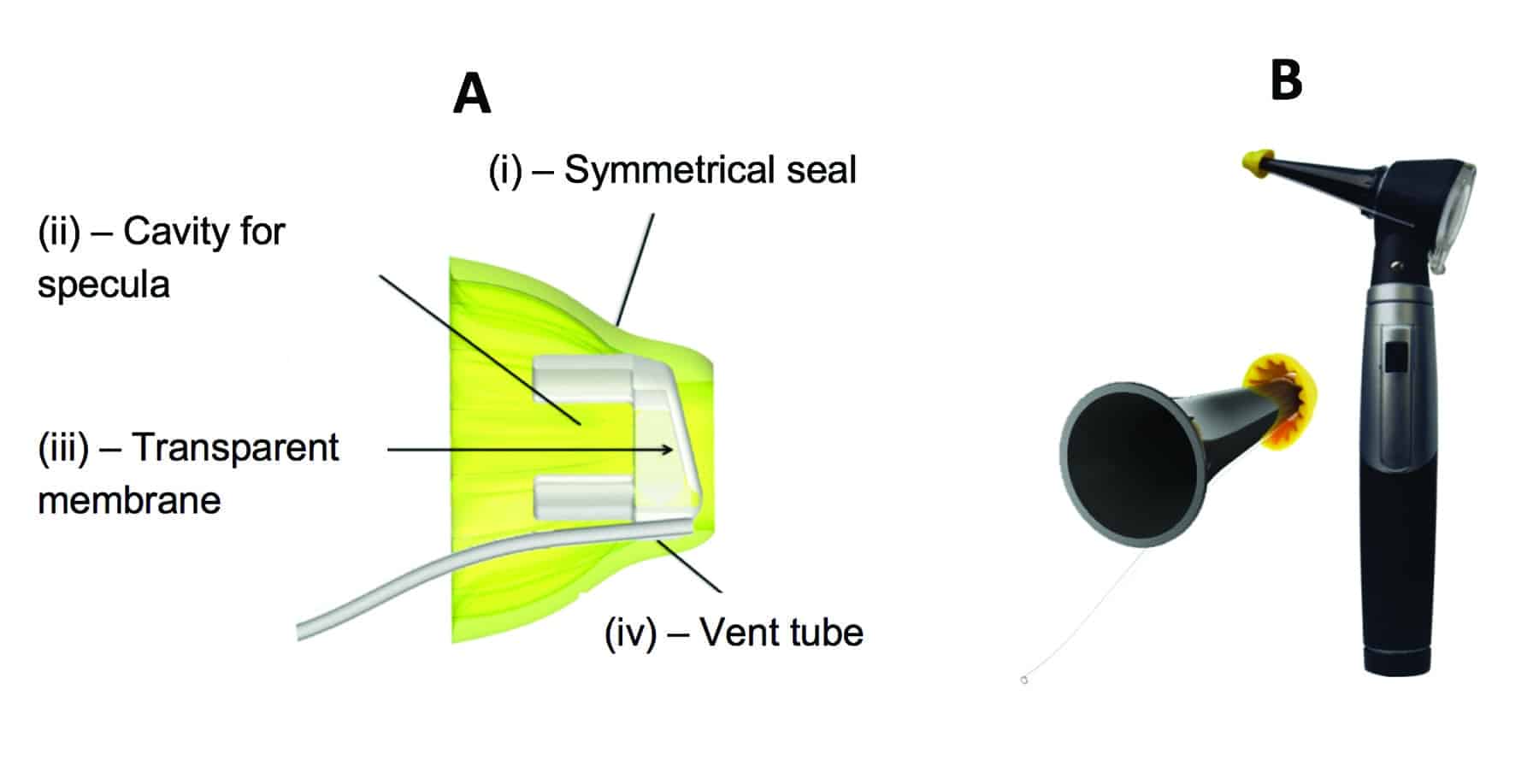
Figure 2a-b. Left: Anatomy of the EVOB showing: (i) Symmetrical seal; (ii) Hollow cavity for the specula; (iii) Transparent membrane (angled to prevent reflection), and (iv) Hollow vent tube. Right: Placement of EVOB on otoscope prior to insertion into the ear.

Figure 3. Ear impression taken with the EVOB showing full anatomy and good information beyond the second bend, in addition to how the EVOB becomes part of the impression which can be scanned and used for modeling.
Previous validation data collected by Schwarzlos Sooprayen3 from 22 participants in 2017 indicates an average improvement in ear canal length of 5.52 mm with EVOB versus standard otoblocks. In the following study, we sought to verify these recent findings using a larger group of participants, and to investigate whether there is any relationship between the length of impressions taken with each otoblock.
Methods
Workshops with experienced clinical audiologists were conducted when Phonak launched the EVOB in New Zealand. A total of 44 of the clinicians who attended took impressions of the same ear using both a standard otoblock and the EVOB (ie, total of 88 ear impressions for analysis). Clinicians were free to choose which ear they took the impressions from and which block they used first. Impressions were taken according to standard clinical guidelines in New Zealand.4 Welch Allyn otoscopes were used. Impression material was either Otoform A softX used with a Dreve impression gun or Otoform Ak X and a standard ear impression syringe. Otolights were used for standard otoblock placement. Welch Allyn pediatric speculae (Ø 2.4-3 mm) were used for EVOB placement.
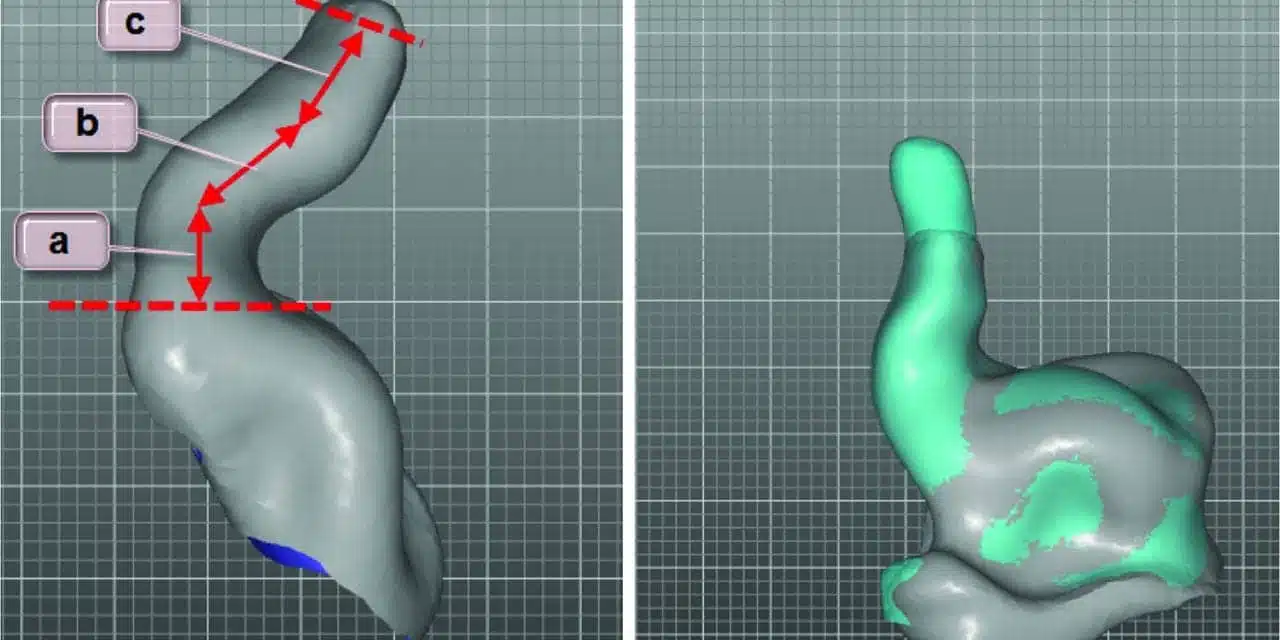
Ear impressions were scanned, then aligned and compared in our rapid shell modeling software application in order to measure the ear canal depth with the standard otoblock and the EVOB (Figure 4a-b).

Figure 4a-b. Left: Technique for measuring the absolute canal length in the current study. a + b + c = canal absolute canal length with standard otoblock. Right: Align and compare of impression taken with the standard otoblock (grey) and the EVOB (light blue). In this case, the EVOB has enabled an additional 7 mm canal depth. (Note: grid lines are 1 mm.)
Results
A total of 64% of the clinicians spontaneously chose to take impressions from the right ear. Results show that ear impressions taken with the EVOB were, on average, 3.2 mm (~30%) longer than those taken with the standard otoblock (Figure 5). A paired sample t-test indicates that impressions taken with the EVOB were significantly longer that those taken with the standard otoblock (P < .001).
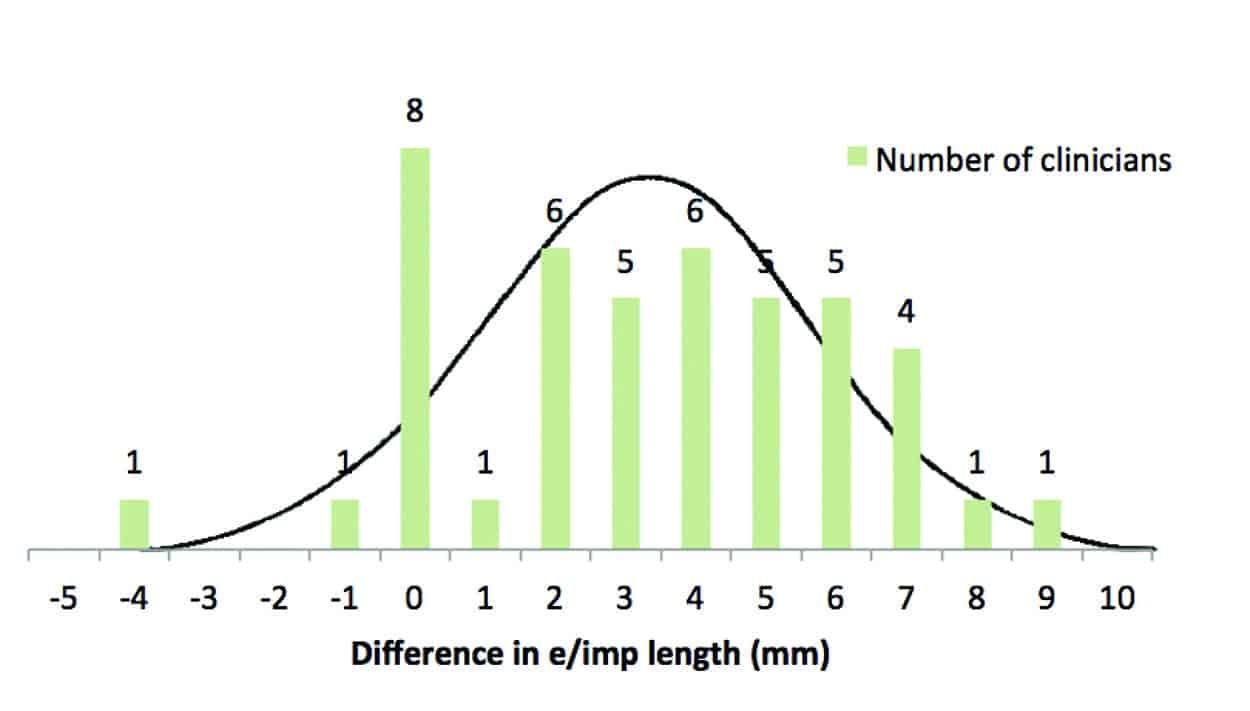
Figure 5. Histogram showing the difference in ear impression length (mm) for the 44 clinicians at the workshop.
A regression analysis comparing the length of impressions taken with the EVOB versus standard otoblock indicates a positive, significant correlation (p <.001). Figure 6 shows that, when the linear regression best fit is compared to unity, in general the additional length provided by the EVOB was greater when the impression taken with the standard otoblock was shorter. Eight participants took equal-length impressions with the EVOB and standard otoblock, of which 6 (75%) took impressions that were longer than the average taken with the standard otoblock.
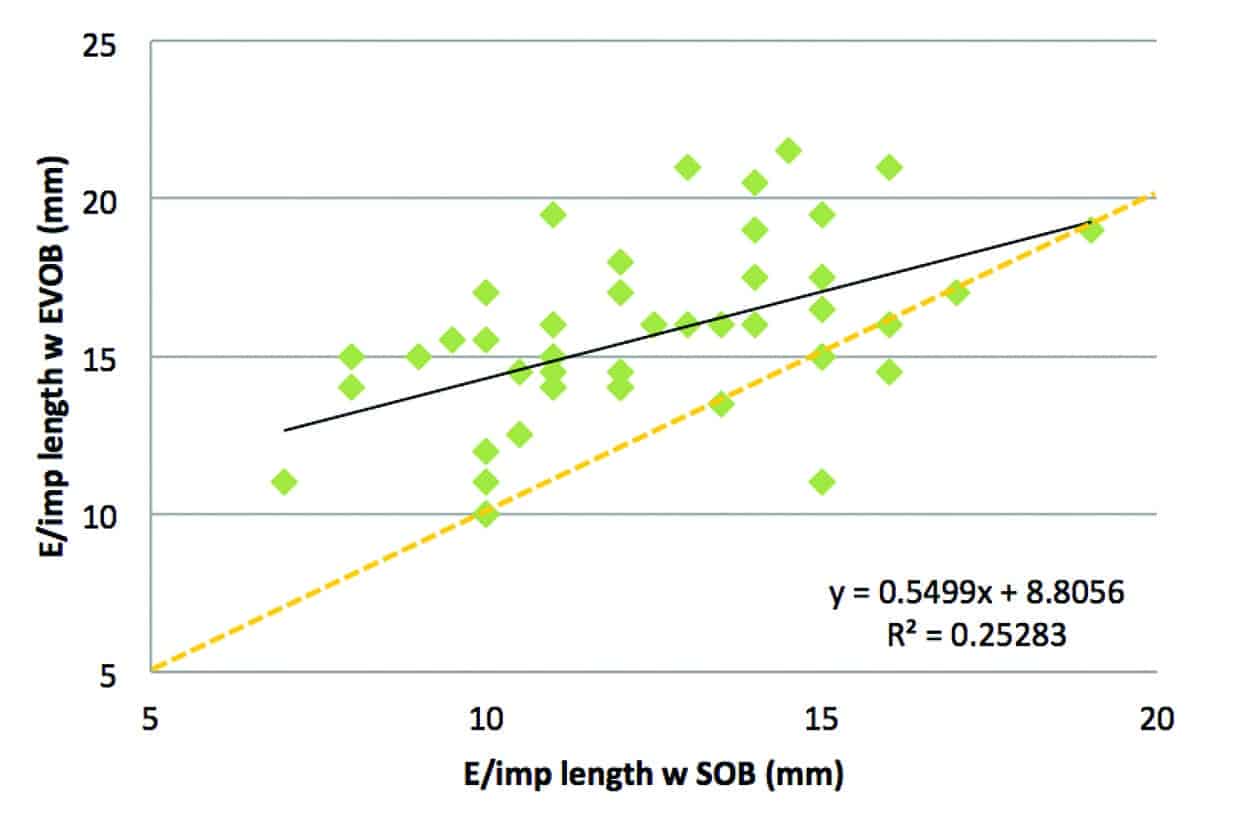
Figure 6. Regression analysis of impression length with EVOB versus standard otoblock (SOB). Plot line (black) shows best fit from linear regression (p <.001) and orange dashed line shows unity.
The benefits provided by the EVOB compared to standard otoblock are not only about additional length; impressions taken with EVOB provide more information about the sound path to the eardrum (Figure 7), and were rated as more comfortable by a number of clinicians when they were undergoing ear impressions.
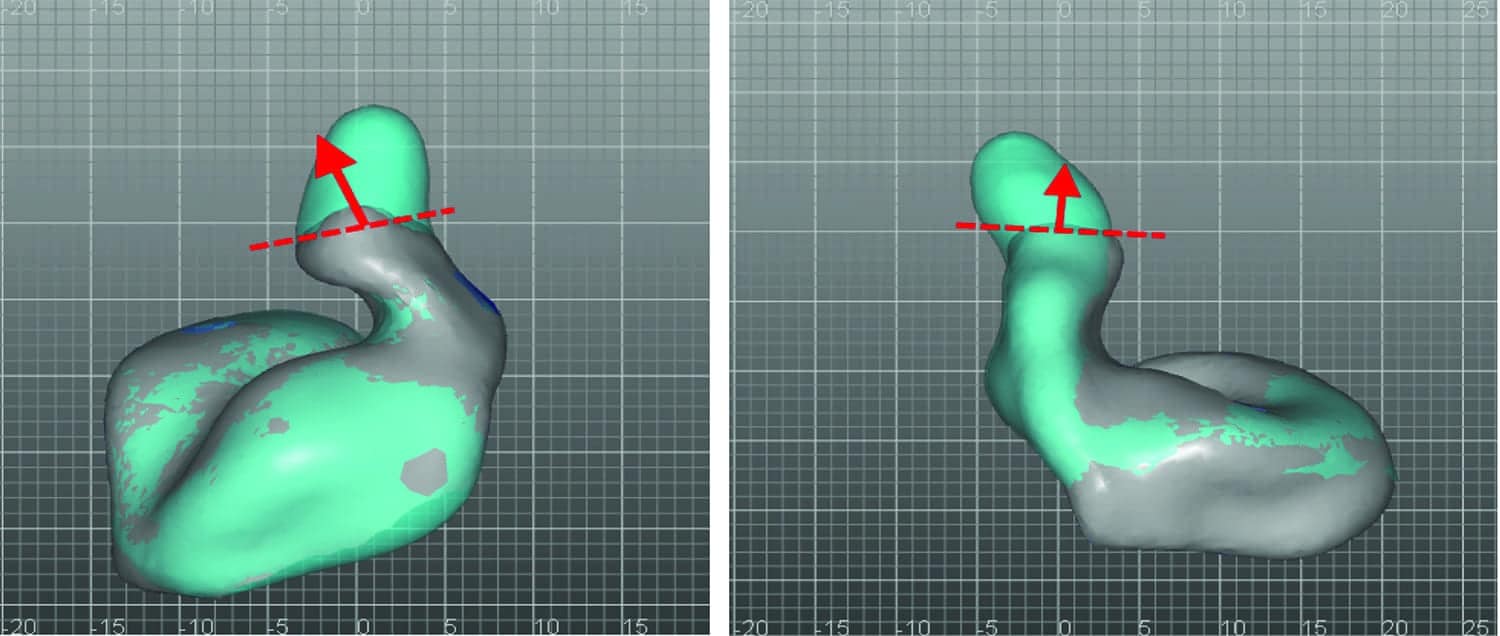
Figure 7a-b. Alignment and comparison of ear impressions taken with a standard otoblock (grey) and EVOB (light blue). These two examples illustrate how the extra information provided by the EVOB enable more accurate placement of the sound bore following the path towards the eardrum.
Discussion
Results show a significant average improvement in impression length of 3.2 mm with the EVOB, consistent with the findings of Schwarzlos Sooprayen.3 The average improvement in the current study is less than the average 5.52 mm reported by Schwarzlos Sooprayen, which may be due to a combination of factors such as their smaller sample size, different measurement technique (from base of impression, we estimated length from ear canal opening), and a significant outlier in their data (15 mm improvement).
The finding that additional length provided by the EVOB was greater when the impression taken with the standard otoblock was shorter is perhaps due to the increased visibility the EVOB window provides, increasing confidence, or due to the fact that for already deep impressions, there is less room for additional length gains.
Conclusions
Overall, the results indicate the EVOB supports clinicians taking deeper impressions that are safer and more comfortable for the client, enabling the modeling and production of more accurate custom products for higher first fit success.
Correspondence can be addressed to HR or David Crowhen at: [email protected]
Original citation for this article: Crowhen D. An innovative otoblock that enables deeper impression taking. Hearing Review. 2017;24(11):24-28.
References
-
Oliveira R, Babcock M, Venem M, Hoeker G, Parish B, Kolpe V. The dynamic ear canal and its implications. Hearing Review. 2005;12(2):18-19,82.
-
Pirzanski C. Earmolds and hearing aid shells: A tutorial part 2: Impression-taking techniques that result in fewer remakes. Hearing Review. May 2006. Available at: https://hearingreview.com/2006/05/earmolds-and-hearing-aid-shells-a-tutorial-part-2-impression-taking-techniques-that-result-in-fewer-remakes
-
Schwarzlos Sooprayen JK. Deeper ear impressions with EasyView Otoblock. Stafa, Switzerland: Phonak AG;March 2017. Available at: https://www.phonakpro.com/content/dam/phonakpro/gc_hq/en/resources/evidence/field_studies/documents/fsn_easyview_otoblock.pdf
-
New Zealand Audiological Society. Professional Practice Standards, Part B: Clinical Practice. Available at: https://www.audiology.org.nz/Userfiles/file/ProfessionalPracticeStdrds/NZAS%20Professional%20Practice%20Standards%20Part%20B%20Clinical%20Practice%20July%202015.pdf



