Tech Topic | November 2018 Hearing Review
Several “autoREMfit” systems have been developed to assist in hearing aid fittings. This article evaluates a new fit-to-target platform, Audioscan’s VerifitLINK, that could be integrated into any manufacturer’s software, and documents its performance in target matching during hearing aid fitting.
Routine verification of aided hearing aid responses using real-ear measurements (REM) is part of recommended practice,1-3 and failing to verify hearing aid fittings using this technique has been listed as the number one mistake made by clinicians.4 Research has revealed positive listening outcomes for patients fitted using best practice REM verification versus first-fit approaches in both lab-based and real-world environments.5-8
Yet, despite professional guidelines and research evidence, REM is not routinely performed by clinicians.9,10 This lack of use is attributed by some to the perceived complexity of the REM process and the limited time available to complete measurements on the part of the clinician.9
To address these concerns, a number of manufacturers have developed Closed Loop Fitting Systems (CLFS) or “autoREMfits.” While the details of each implementation may vary, at their core, these systems aim to automatically adjust hearing instrument parameter settings in the hearing aid fitting software to the supplied fitting formula targets via a comparison between measured and requested output levels across frequencies.11,12 (For an excellent review, see Mueller and Ricketts’ article “Will AutoREMfit Move the Sticks? 13).
Recently, Audioscan developed the automated fit-to-target tool, VerifitLINK, which allows direct communication between manufacturer’s hearing aid fitting software and Verifit systems. VerifitLINK has the potential to be integrated into any hearing aid manufacturer’s fitting software to allow automatic adjustment of hearing aid settings to match the fitting formula targets supplied by the Audioscan equipment. VerifitLINK and hearing aid software (in this study, Oticon Genie 2) exchange data while real-ear measures are conducted and adjustments are automatically made to the gain settings in the device based on the output of the hearing aid as measured by the Audioscan Verifit.
In a collaboration between Audioscan and the National Centre for Audiology, a validation study of Audioscan VerifitLINK, as implemented into Oticon Genie 2 software, was conducted. The study investigated the efficiency and accuracy of VerifitLINK compared to a clinician-driven fitting approach and the manufacturer’s first-fit to DSL v5.0 adult targets using real-ear measures with the Audioscan Verifit2. It should be noted that, although not presented here, VerifitLINK can also be used with validated generic DSL v5 child, NAL-NL1, and NAL-NL2 targets supplied by the Verifit and that, when appropriate, can be used to fit hearing aids to target in the test box rather than on the ear. VerifitLINK is also available for use with the Audioscan Verifit1 (serial numbers 2070 or higher).
Study Methods
Binaural Oticon Opn 1 hearing aids were fitted to 22 adult participants using the Audioscan Verifit2 (software version 4.13.38). The participants had sensorineural hearing loss which fell within the fitting range of the Oticon Opn 85 and 100 receivers (Figure 1).

Figure 1. Thresholds per frequency averaged across the left and the right ears of all 22 participants with the minimum and maximum threshold values per frequency.
In this study, three fitting protocols were used: VerifitLINK, Clinician Fit, and the Manufacturer’s First Fit. For all three fitting protocols, the participant’s audiogram and measured HA-1 foam tip real-ear-to-coupler difference (RECD) values were entered into the Oticon Genie 2 Software (software version 2018.1-4.0.784.31). For the Clinician Fit and Manufacturer’s First Fit protocols, the audiogram and measured HA-1 foam tip RECD values were entered into the Audioscan Verifit2, as well. The DSL v5.0 adult fitting formula was chosen in the Genie 2 software, and participants were fitted with the dome type recommended by the fitting software dependant on their hearing loss. Relative to experience level, “experienced” was chosen for all participants. As recommended by the manufacturer, for all fitting protocols, the hearing aids were initially first-fit to the target being used (in this case DSL v5.0 adult) after the participant and acoustic information were entered.
VerifitLINK, as integrated in the REM AutoFit feature within Oticon Genie 2 software, is a three-stage procedure. Figure 2 shows the initial setup screen where the measurement method (ie, On ear, Test box), Fitting rationale (eg, DSL adult, DSL child, NAL-NL2), Signal Type (eg, Speech-ISTS, Speech-Std(F), Speech-Std(M)) and RECD source (ie, Genie 2, Verifit Measured, Verifit Average) can be chosen. In this study, the following setup parameters were used: On ear, DSL adult, Speech-ISTS, and the RECD which had been entered into Genie 2.

Figure 2. The VerifitLINK setup screen as displayed in the Oticon Genie 2 software. In this screen, the measurement method, fitting rationale, signal type, and RECD source are chosen.
The participant was prepared for REM using Audioscan-recommended procedures, including placing the end of each probe tube within 5 mm of the tympanic membrane using otoscopy and the visually assisted positioning technique.14 Authors’ note: A review of probe-tube placement strategies for use with Audioscan equipment can be found on YouTube at: https://www.youtube.com/watch?v=m4VkK0OAbMw.
To remove the confounding factor of probe-tube placement differences, once the probe tube and hearing aids were placed in the participants’ ears, all fitting types were completed without moving the probe tube or hearing aids. The fitting type order was counterbalanced across the 22 participants.
During the Manufacturer’s First-Fit and Clinician-Fit conditions, real-ear aided responses (REARs) at inputs of 50, 65, 75 dB SPL overall RMS using the ISTS signal, and MPO were completed using the binaural link feature of the Audioscan Verifit2. In cases of difficulty with binaural equalization, the hearing aids were measured monaurally. Each of the fittings were timed starting at the presentation of the first test signal and stopping at the completion of the final MPO test signal.
Fitting Specifics:
- Manufacturer’s First Fit: There were no adjustments made to the gain of the hearing aids based on the Verifit2 results following the Manufacturer’s First Fit to the DSL adult fitting formula.
- Clinician Fit: The gain of the hearing aids was manually adjusted by an experienced audiologist in the Genie 2 software to match the DSL adult targets shown on the Verifit2.
- VerifitLINK: VerifitLINK, as integrated in Genie 2, measured and adjusted the hearing aids through its automatic procedure to match the DSL adult targets shown on the Verifit2. This process consisted of a series of four automatic monaural measurements: 1) initial measurements left; 2) initial measurements right; 3) gain-adjusted measurements left; 4) gain-adjusted measurements right.
Each measurement group included REARs at 50, 65, and 75 dB SPL. The MPO was measured at the end of the series in the manual mode of VerifitLINK. Figure 3 shows a representative screenshot of the Genie 2 software after the VerifitLINK procedure was completed.
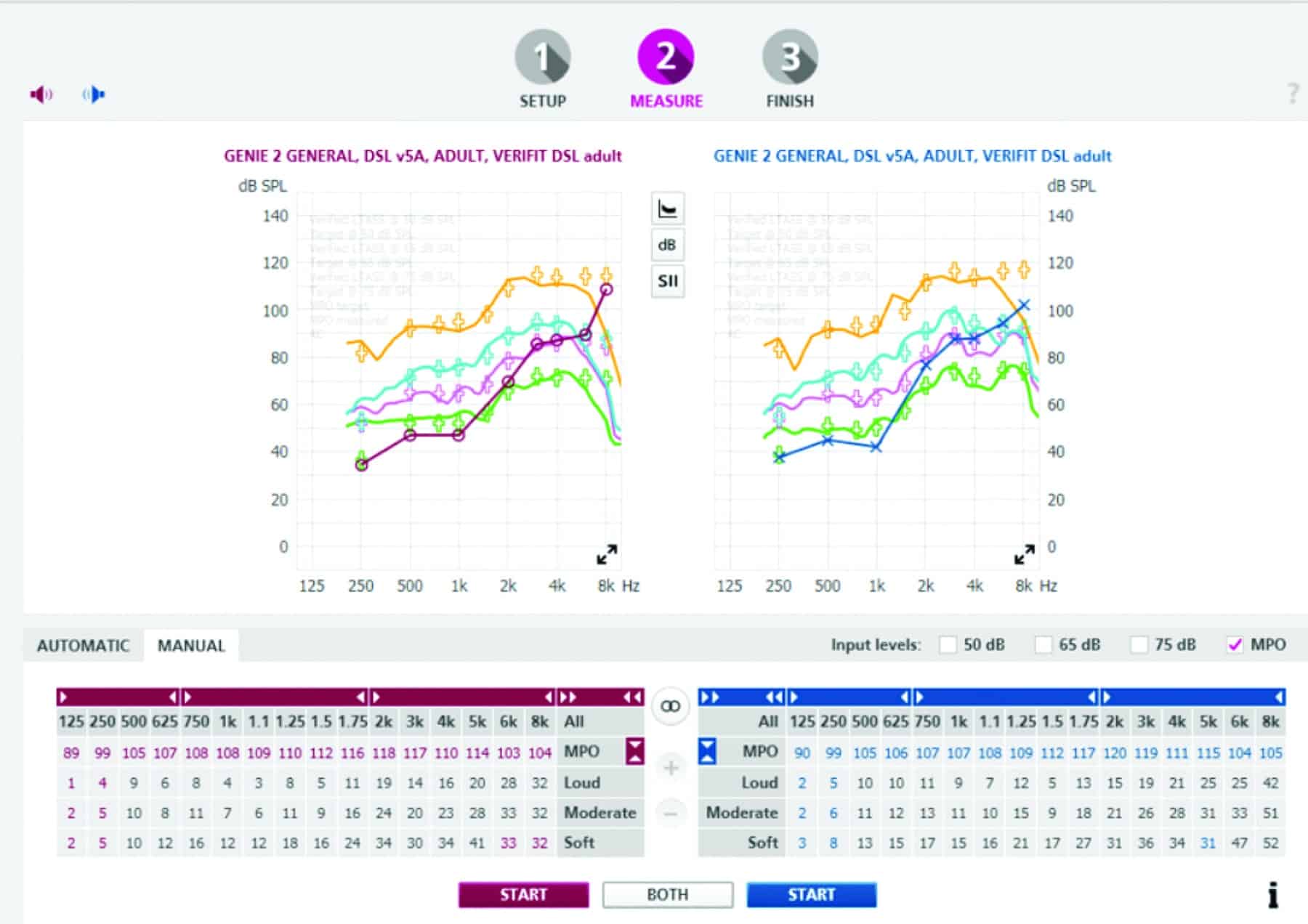
Figure 3. A screenshot of Genie 2 software after completing VerifitLINK real-ear aided responses (REARs) with 50, 65, and 75 dB SPL, and MPO inputs.
The Audioscan Verifit2 sessions were saved for each of the fitting types from all participants for analysis. Fit-to-target accuracy, SII scores, as well as the time taken to complete the fitting were compared for the three fitting types. Because the gain adjustments of the automated real-ear (VerifitLINK) procedure implemented in Genie 2 software are based on target deviation calculations with the average (65 dB SPL) input signal, it was also of interest to evaluate the match-to-target impact with soft (50 dB SPL) and loud (75 dB SPL) speech inputs.
Results
Group data were analyzed for the 22 participants. Repeated Measures Analysis of Variance (ANOVA, GLM SPSS v24) was used to evaluate measurement differences between fitting types for: 1) Fit-to-target accuracy; 2) Speech Intelligibility Index (SII), and 3) Time to complete fitting. If significant differences were revealed, post-hoc paired comparisons were completed with Bonferroni corrections.
Fit-to-target accuracy. One method to determine how well hearing aids have been fitted is to calculate the root mean square error (RMSE) from target15 using the difference between the measured output at a defined group of frequencies and the target SPL at those frequencies. In this study, the RMSE from 500-6000 Hz was calculated for each of the three fitting types (Figure 4). Within-subjects variables of ear, test level, and fitting type were evaluated. Overall, the average Manufacturer’s First-Fit deviation was 6.7 dB RMS from target, which is outside the 5 dB recommendation found in the literature.15 VerifitLINK and Clinician-fitted conditions had 4.3 dB RMSE and 3.8 dB RMSE, respectively.

Figure 4. The root mean square error (RMSE) from 500-6000 Hz with standard deviation are presented for the three fitting types at three input levels (50, 65, 75 dB SPL). The RMSE when hearing aids were fit with VerifitLINK were not significantly different than those obtained when the hearing aids were manually fit by an experienced audiologist (Clinician Fit), but both VerifitLINK and the Clinician Fit were significantly different than the Manufacturer’s First Fit as indicated by the asterisks.
Of note, the ANOVA found that “test level” was not a significant factor, indicating an acceptable target match across multiple input levels. Thus, while the automated target match for this manufacturer’s implementation was based on the 65 dB SPL input, using the manufacturer’s recommended approach to first fit to the fitting formula that will be used in VerifitLINK resulted in the appropriate input/output function for the DSL adult prescription.
There was an overall effect of fitting type (F(1.647, 34.6)=.957, p<.001, ?2=.725). There was a significant interaction between test level and fitting type (F(1.089, 61.524)=3.978, p=.012, ?2=.159). Pairwise comparisons indicated a significant difference between the Manufacturer’s First Fit and both the Clinician Fit (p<.001) and VerifitLINK (p<.001), but no significant difference between the Clinician Fit and the VerifitLINK.
To illustrate the differences in average output for the three different fitting conditions evaluated in this study, the mean REARs for each of the three input levels (50, 65, and 75 dB SPL) for each of the fitting types are presented in Figure 5. In general, measurements show that the Manufacturer’s First Fit to DSL adult targets resulted in lower REARs across frequencies for each input level than both the Clinician Fit and VerifitLINK fittings, in addition to underfitting the DSL adult REAR targets.
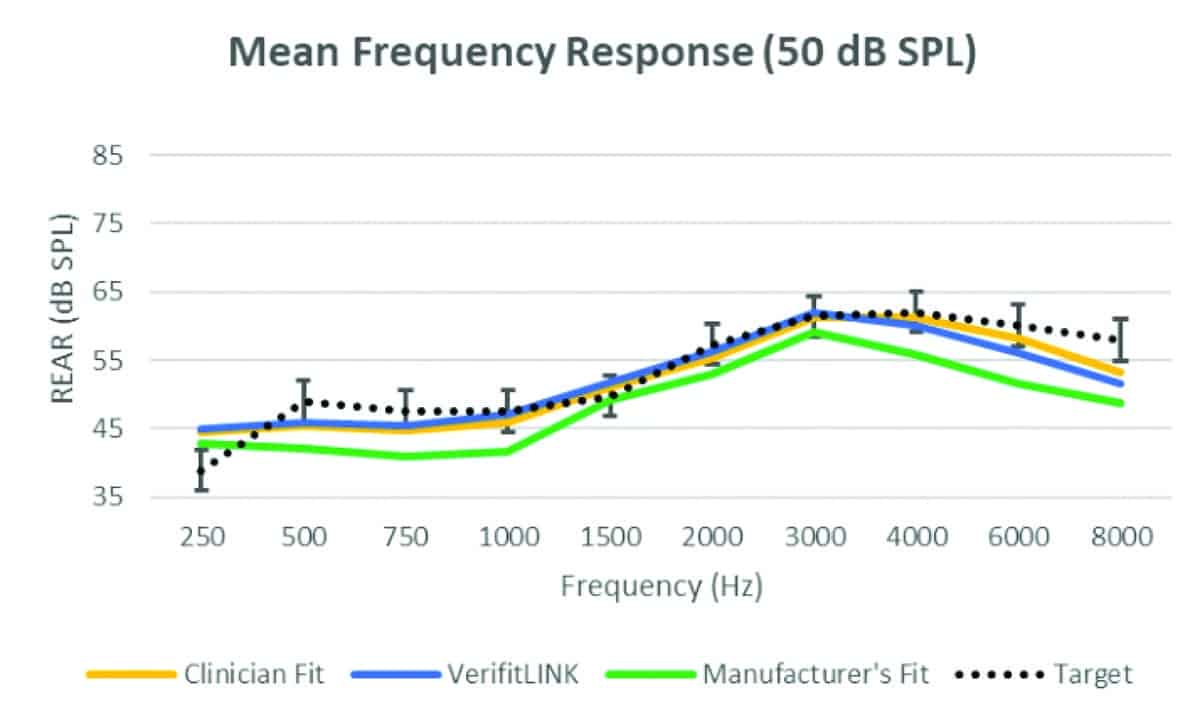

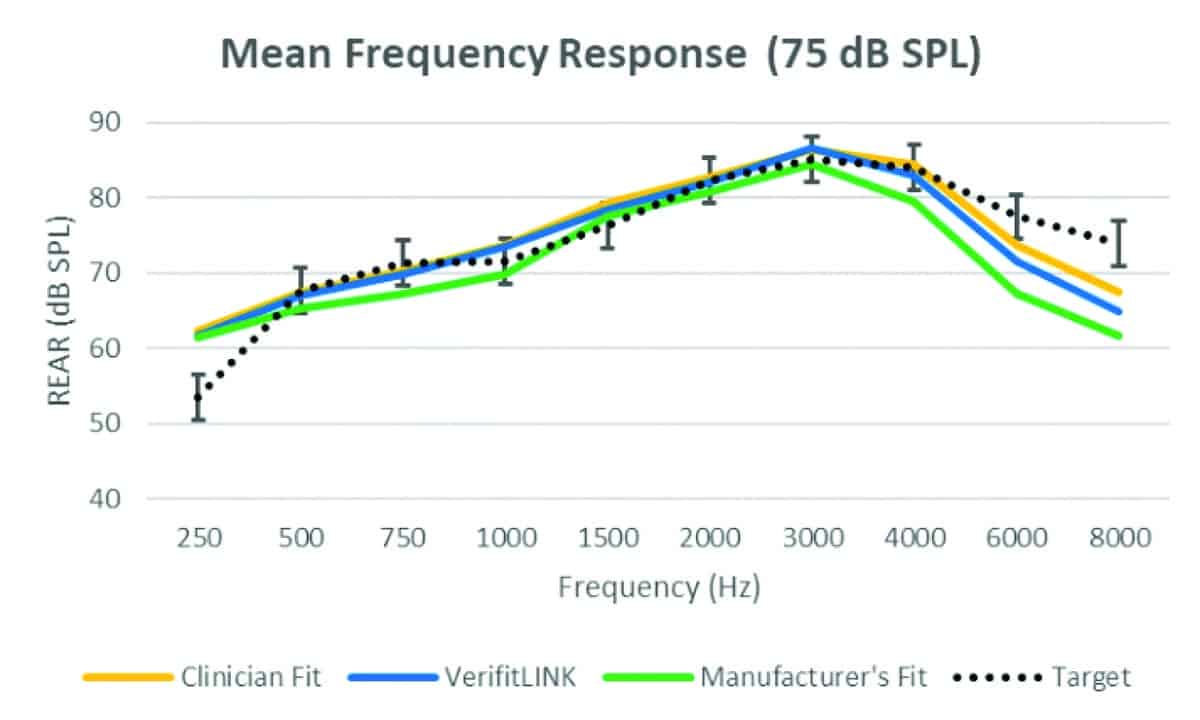
Figure 5. Real-ear aided responses (REARs) measured from 44 ears for 50, 65, and 75 dB SPL inputs for the three fitting types. The mean targets with ±3 dB error bars have been added for reference.
Speech intelligibility (SII).The SII, which is shown on the Audioscan Verifit1 and Verifit2 Speechmap screen as a number between 0 and 100, is an indicator of the intelligibility of speech provided by the frequency gain response of the hearing aid fitting at that specific test level.16 Within-subjects variables of ear, level, and fitting type were evaluated (Figure 6). As expected, there was an overall effect of level (F(2,26.627)=347.77, p<.001, ?2=.943). In addition, there was an overall effect of fitting type (F(2, 22.699)=21.019, p<.001, ?2=.637), and an interaction between level and fitting type (F(1.518, 31.874)=44.16, p<.001, ?2=.678). Pairwise comparisons indicated a significant difference between the SII obtained using the Manufacturer’s First Fit and both the Clinician Fit (p<.001) and VerifitLINK (p<.001), but no significant difference between the SII obtained in the Clinician Fit compared to VerifitLINK.
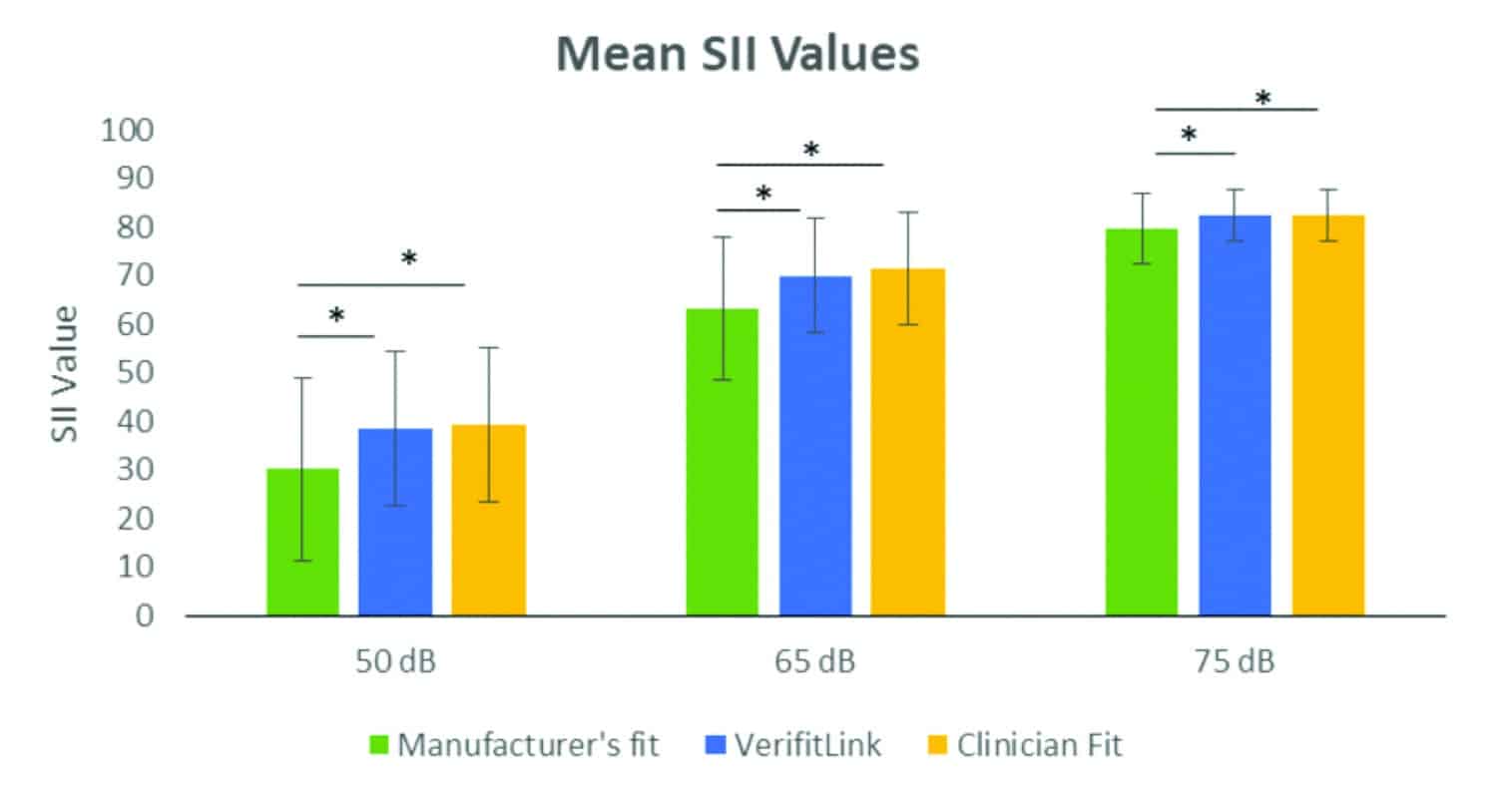
Figure 6. The mean speech intelligibility index (SII) values with standard deviations are presented for the three fitting types at three presentation levels (50, 65, 75 dB SPL). Analysis showed that the SII values obtained using VerifitLINK were not significantly different than those obtained when the hearing aids were fitted by an experienced audiologist, but both VerifitLINK and the Clinician Fit were significantly different than the Manufacturer’s First Fit as indicated by the asterisks.
The level by fitting type interaction was a result of significant differences between the Manufacturer’s First Fit and the other two fitting methods at all three levels. There was no significant difference in SII scores between the VerifitLINK and Clinician Fit at any of the three levels.
Test-retest. A total of 7 participants were run through the test protocol twice in order to measure the test-retest of the three different fitting types. Following the completion of the main protocol measures, the Verifit2 was restarted and the data within the system was erased. The probe tube was not moved out of the ear canal to ensure that probe-tube placement was not a variable in any measured differences between the initial and retest measures. The procedure was then repeated starting with the detection of the hearing aids. The real-ear aided response (REAR) differences between the first and second sets of measures were found at the audiometric frequencies between 250 and 8000 Hz for each of the three test levels for each of the fitting types. Test-retest values were below 2.5 dB for each of the fitting types across frequencies (Figure 7).
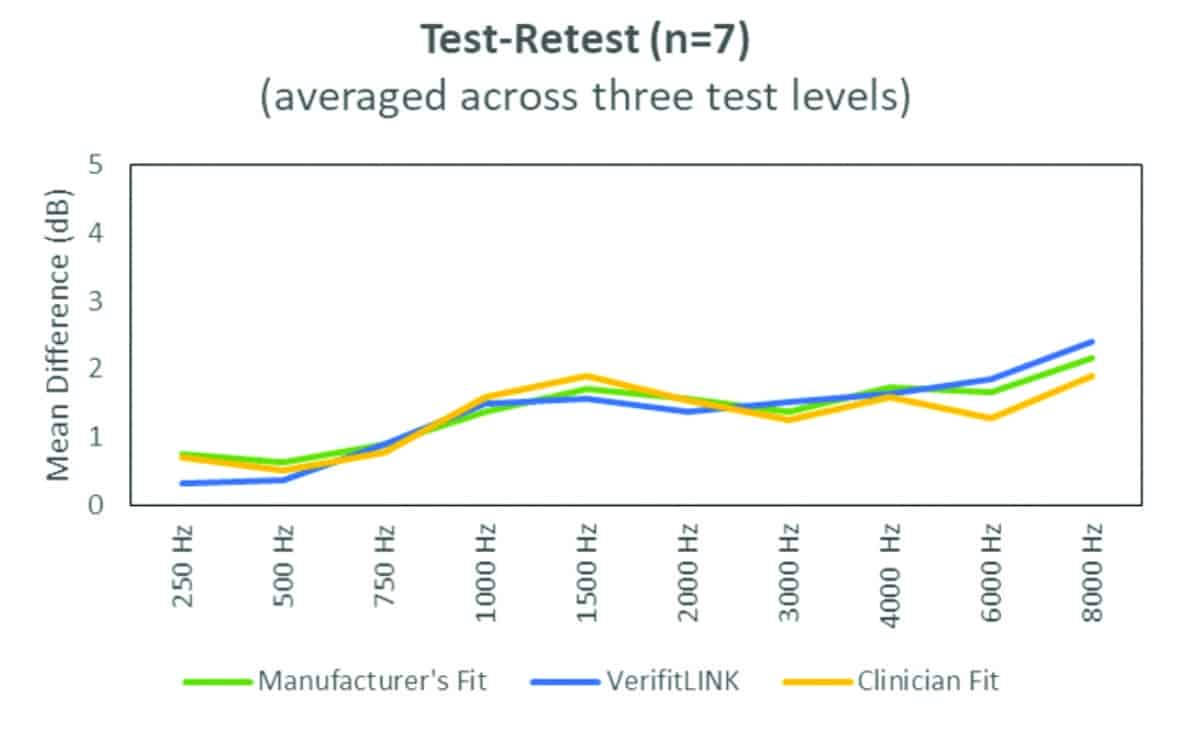
Figure 7. The mean test-retest values from seven participants averaged across three presentation levels (50, 65, 75 dB SPL) for the three fitting types. Test-retest was below 2.5 dB at all audiometric frequencies for all fitting types.
Time to complete the fitting. The time to complete REARs at 50 dB, 65 dB, 75 dB, SPL, and MPO inputs binaurally was measured for each of the fitting types, using simultaneous measurement whenever possible and sequential bilateral measurement otherwise. Durations were calculated in the following manner:
1) For the Manufacturer’s First Fit: When the fit-to-target icon was clicked until completion of all four REAR measures binaurally;
2) For the VerifitLINK: When the start button was clicked in Stage 2 of the VerifitLINK screen until completion of all four REAR measures binaurally; and
3) For the Clinician Fit: When the first stimulus was presented until completion of all four REAR measures binaurally.
As shown in Figure 8, mean times to achieve fit-to-target were: Manufacturer’s First Fit: 2 minutes and 2 seconds; VerifitLINK: 4 minutes 41 seconds; Clinician Fit: 7 minutes 16 seconds. The ANOVA revealed a significant overall effect of time(F(1.175,24.668)=74.296, p<.001, ?2=.780). Pairwise comparisons with Bonferroni corrections were completed and indicated the time to complete the fitting for each of the three methods were significantly different from each other (p<.001).
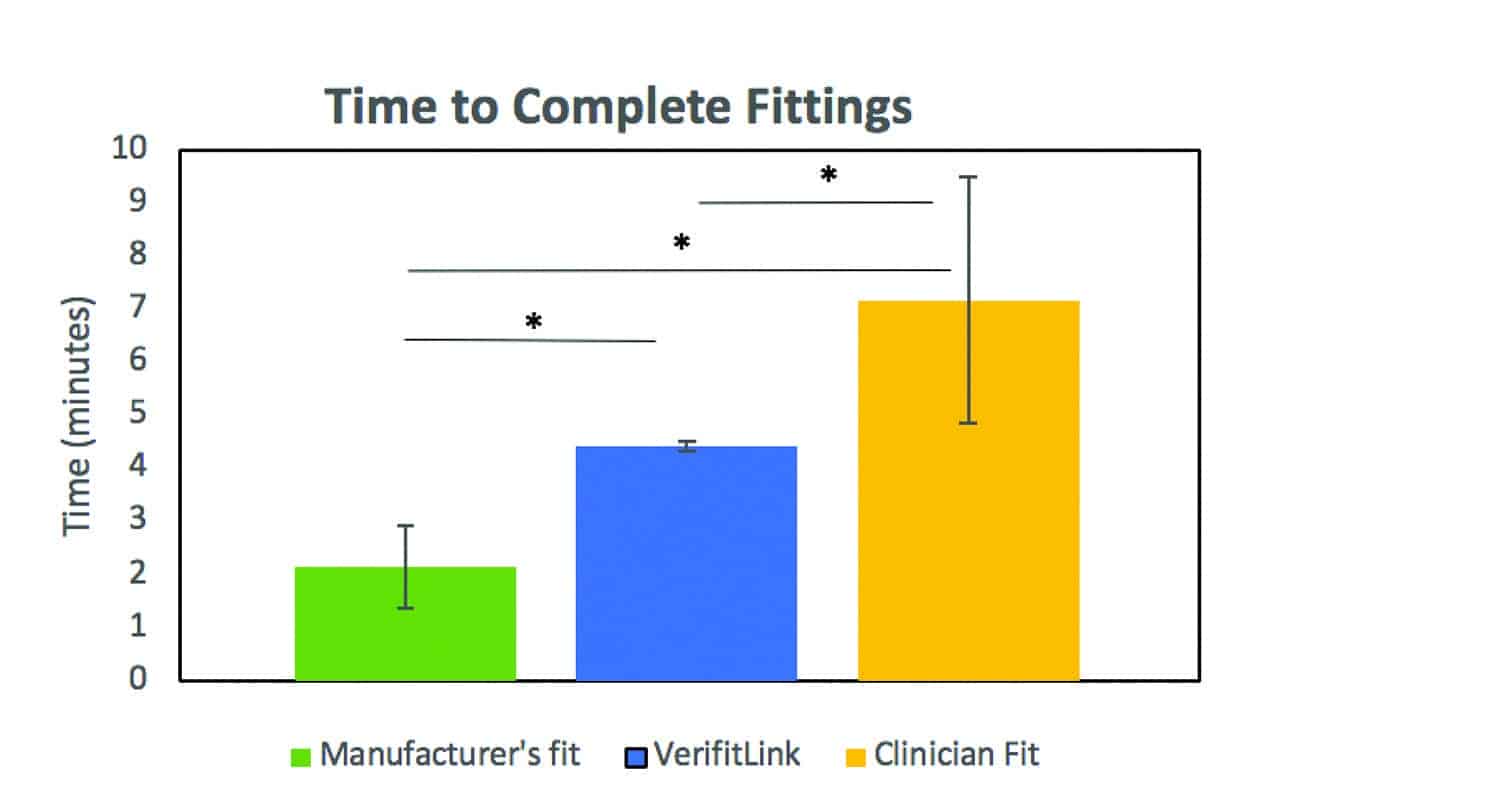
Figure 8. Each hearing aid fitting was timed and the mean times until completion are presented. Analysis showed a significant difference between all three fitting types.
Example: On-Ear Fittings Using the Three Fitting Methods
Figure 9 shows a representative sample case in which both VerifitLINK and Clinician Fit provided closer fits-to-target and improved SII scores compared to the Manufacturer’s First Fit. RMSE deviation from target is calculated from 500-6000 Hz and is largest with the Manufacturer’s First Fit. The time-to-match target for the VerifitLINK was under 4 minutes 30 seconds. The time-to-match target during the clinician fitting was 9 minutes and 17 seconds for all four levels and both ears.
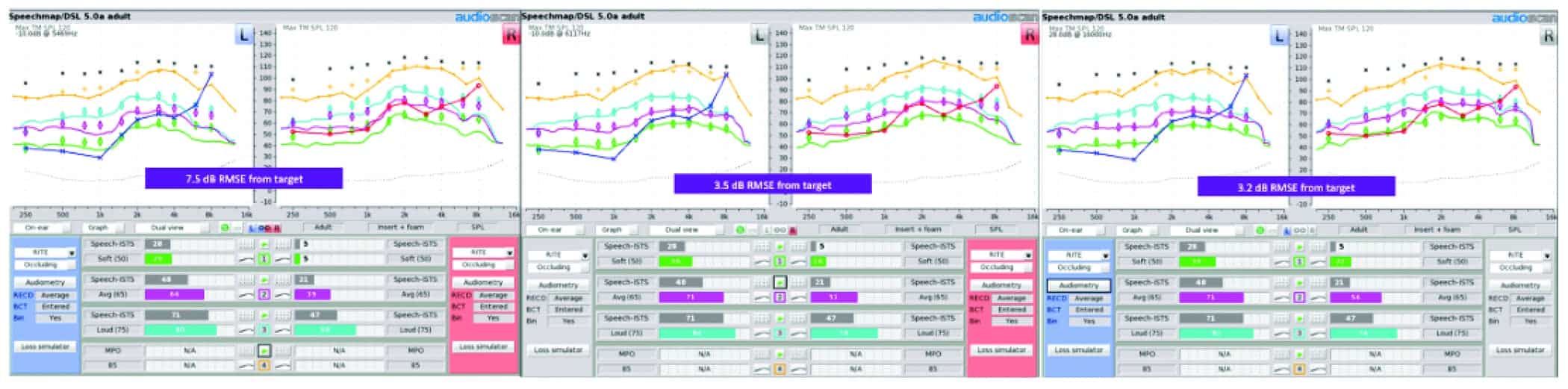
Figure 9. Verifit2 screen shots of the real-ear aided responses (REARs) of the three fitting protocols for one subject (from left to right): Manufacturer’s First Fit, VerifitLINK, Clinician Fit.
Summary
The current study investigated a recently developed automated match-to-target verification platform that integrates Audioscan Verifit systems with hearing instrument fitting software; in this case, Oticon Genie 2. As revealed in the findings above, this approach has the potential to provide multiple clinical benefits. In addition to being a timesaving method for target matching, these results are encouraging for those clinicians who may be unfamiliar with the process of adjusting hearing aids using REM. In the cases that have been evaluated, the VerifitLINK provides a fit to DSL v5.0 adult targets that is not significantly different than a fitting completed by an experienced audiologist in significantly less time. For these benefits to be realized, proper procedures for hearing aid fitting and real-ear measures (eg, appropriate probe tube placement in the ear canal) are required for accurate fitting results regardless of fitting method. Positive outcomes with amplification no doubt require a holistic (re)habilitative approach that considers multiple factors beyond simple target matching. As outlined above, the automated match-to-target approach provides clinicians with the opportunity to use their time for other aspects of clinical practice while supporting the use of best practice verification procedures during the hearing aid fitting process.
References
-
Valente M, Abrams H, Benson D, et al. Guidelines for the audiologic management of adult hearing impairment. American Academy of Audiology. https://audiology-web.s3.amazonaws.com/migrated/haguidelines.pdf_53994876e92e42.70908344.pdf. October 30, 2006.
-
College of Audiologists and Speech-Language Pathologists of Ontario (CASLPO). Practice standards for the provision of hearing aid services by audiologists.http://www.caslpo.com/sites/default/uploads/files/PS_EN_Practice_Standards_for_the_Provision_of_Hearing_Aid_Services_By_Audiologists.pdf. October 18, 2016.
-
Valente M, Bentler R, Kaplan HS, et al. Guidelines for hearing aid fittings for adults. Am J Audiol. 1998;7:5-13.
-
Kochkin S, Beck DL, Christensen LA, et al. MarkeTrak VIII: The impact of the hearing healthcare professional on hearing aid user success. Hearing Review. 17(4):12-34.
-
Valente M, Oeding K, Brockmeyer A, Smith S, Kallogjeri D. Differences in word and phoneme recognition in quiet, sentence recognition in noise, and subjective outcomes between manufacturer first-fit and hearing aids programmed to NAL-NL2 using real-ear measures. J Am Acad Audiol. 2018;29(8):706-721.
-
Amlani AM, Pumford J, Gessling E. Real-ear measurement and its impact on aided audibility and patient loyalty. Hearing Review. 24(10):12-21.
-
Abrams HB, Chisolm TH, McManus M, McArdle R. Initial-fit approach versus verified prescription: Comparing self-perceived hearing aid benefit. J Am Acad Audiol. 2012;23(10):768-778.
-
Leavitt RJ, Flexer C. The importance of audibility in successful amplification of hearing loss. Hearing Review. 2012;19(13):20-23.
-
Mueller HG. 20Q: Real-ear probe-microphone measures—30 years of progress? Lecture presented at: AudiologyOnline; January 12, 2014.
-
Mueller HG, Picou EM. Survey examines popularity of real-ear probe-microphone measures. Hearing Journal. 2010;63(5):27-32.
-
Koehler ED, Kulkarni S. Fast and easy fitting and verification with integrated real-ear measurement. Hearing Review. 2014;21(10):36-40.
-
Beck DL, Crowe N. Easy, fast, and accurate: Hearing aid fittings via an automated REM system using IMC 2. Hearing Review. 2017;24(4):30-31.
-
Mueller HG, Ricketts TA. 20Q: Hearing Aid Verification—Will autoREMfit move the sticks? Lecture presented at: AudiologyOnline; July 9, 2018.
-
American National Standards Institute (ANSI). Methods of measurement of real-ear performance characteristics of aids (ANSI/ASA S3.46-2013). https://webstore.ansi.org/Standards/ASA/ANSIASAS3462013.
-
McCreery RW, Bentler RA, Roush PA. Characteristics of hearing aid fittings in infants and young children. Ear and Hearing. 2013;34(6):701-710.
-
Scollie S. 20Q:Using the Aided Speech Intelligibility Index in hearing aid fittings. Lecture presented at: AudiologyOnline; September 10, 2018.
Paula Folkeard, AuD, is Research Audiologist/Project Coordinator at Western University’s National Centre for Audiology in London, Ontario; John Pumford, AuD, is Director of Audiology and Education at Audioscan, Dorchester, Ontario; Parvaneh Abbasalipour, MSc, is a PhD candidate, and Nicole Willis is an MClSc candidate at Western University; and Susan Scollie, PhD, is a Professor at Western University and a researcher at the National Centre for Audiology.
Correspondence can be addressed to Dr Folkeard at: [email protected]
Citation for this article: Folkeard P, Pumford J, Abbasalipour P, Willis N, Scollie S. A comparison of automated real-ear and traditional hearing aid fitting methods. Hearing Review. 2018;25(11):28-32.