Part 2: Addressing business and clinical concerns for hearing care professionals
Practice Management | October 2021 Hearing Review
By Carrie Meyer, AuD
While provider participation in managed care remains optional, managed care is now an integral part of US healthcare, and hearing care as a supplemental benefit continues to grow in private and public health plans. Part 1 (published in September) of this 3-part series was a primer on health insurance and managed care. In Part 2, we investigate the recent growth of managed care and the expansion of supplemental benefits such as dental, vision, and hearing care and common perceptions and criticisms of managed care among hearing healthcare providers.
The growth of managed care and how to deal with it has become perhaps the biggest concern among today’s hearing care professional, supplanting fears about big-box retail competition and the new, upcoming class of over-the-counter (OTC) or direct-to-consumer (DTC) hearing devices. While Medicare provisions for hearing aids are also a real legislative concern for many providers, the steady proliferation of Medicare Advantage (MA) plans—driven by our aging population, the prevalence and damaging effects of hearing loss, and the necessity for reducing healthcare costs—are testing the business models under which hearing care professionals have traditionally operated.
This article investigates the recent growth of managed care and the expansion of supplemental benefits such as dental, vision, and hearing care. It also addresses common perceptions and criticisms of managed care among hearing healthcare providers.

Figure 1. Total Medicare Advantage enrollment from 1999 to 2020. Enrollment has been increasing since 2004. Adapted from Kaiser Family Foundation, 2020.3
Key Managed Care Facts and Statistics
- Enrollment in MA has doubled in the last decade.1 The average Medicare beneficiary in 2021 has access to 33 Medicare Advantage plans, the largest number of options available in the last decade.2
- As shown in Figure 1, the percentage of Medicare beneficiaries who have enrolled in a Medicare Advantage program has tripled in the 15 years from the end of 2005 to 2020.3
- Almost 3 out of 4 (72%) Medicare Advantage enrollees have access to hearing aid benefits not covered by traditional Medicare.3 Since 2010, the share of MA enrollees in plans that provide some hearing aid benefits has increased by 37%.
- The 2019 MarkeTrak 10 survey shows that having insurance would be the single biggest motivator to non-owners to consider purchasing a hearing aid sooner.
With hearing aid adoption rates hovering just under 35% for the adult population that could benefit from amplification (Figure 2), managed care plans are seeking to make hearing aids more affordable and accessible for many patients.4-6
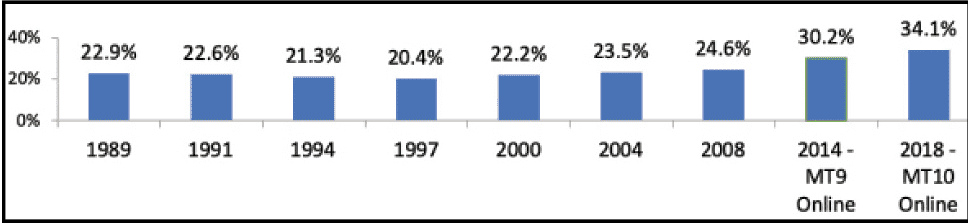
Figure 2. Hearing aid adoption rates in the United States, 1989-2018. Despite steady growth since 1997, hearing aid adoption rates have increased by only 11.2% over almost 3 decades. Source: MarkeTrak data, Hearing Industries Assn.
The training and expertise of audiologists and hearing aid specialists are focused on the evaluation and treatment of hearing loss. Hearing aids are the most common treatment option for most adults with hearing loss. So, if managed care plans can improve the likelihood that patients with hearing loss will pursue and purchase amplification, why is participation in managed care viewed as a detriment rather than a benefit? Let’s address some of the most-common concerns.
Concern #1: Participation with a managed care plan means lower revenue.
Because managed care plans pay providers a fixed fee for their services, many providers are understandably concerned that seeing patients with managed care benefits will reduce their revenue stream. There are some managed care plans that will not be a good fit for your practice, and you should not sign up for every plan simply because more patients are being seen in your office with managed care benefits. Reimbursement rates and practice revenues are paramount in keeping your doors open, so every contract needs to be thoroughly read, assessed, and understood. There are several articles (eg, see the point-counterpoint by Singleton & Green7 and Cavitt8 in the Jan 2018 HR) and resources for assessing the pros and cons of third-party administrators (TPAs) and hearing aid referral networks who market and offer provider driven care. Part 3 of this series explores ways to build a successful and sustainable practice while participating in managed care.
Acknowledging the above, it should also be remembered that any hearing aid fitting—whether it is funded by an insurance benefit or private pay—has more financial components than just the fitting fee. A patient referral from a managed care plan occurs at no cost to the participating provider. In a managed care plan, patients with a hearing benefit will be referred to a network provider in their specific geographic area. There are no advertising or marketing costs for these referrals. For a private practice clinic, marketing can cost several hundred dollars per patient to generate an appointment that results in a hearing aid fitting. In addition, with a managed care patient there can be additional referrals generated by high quality care. A patient who is satisfied with their hearing aid fitting, whether a managed care or private-pay patient, can potentially generate referrals by recommending their provider or clinic to friends, neighbors, coworkers, and family members.
Another concern for providers considering managed care participation is aftercare. Many hearing healthcare plans offer members aftercare at no cost for a set period. Aftercare is included in the cost of the hearing aid for the patient, and because the hearing aid and fitting costs are usually bundled, there is a single reimbursement to the provider. This is also a very common service delivery model for private-pay patients, with the dispensing fee, devices, and aftercare combined into a single cost for the patient. While follow-up appointments are critical to patient success with hearing aids, some hearing care professionals express concern that managed care patients may over-utilize their aftercare program and potentially impact their practices both financially and in use of additional clinic appointments.
With both managed care and private-pay patients, there is potential for overuse of follow-up visits. Use of clinical best practices can improve patient satisfaction and reduce excessive use of professional time. In recent studies, it was found that use of real-ear verification measurements as part of routine hearing aid fittings improved patient satisfaction, which could reduce the number of return visits and decrease hearing aid returns (Figure 3).9-11 With less than half of dispensing audiologists using real-ear verification consistently, both managed care and private-pay patients will continue to clog clinic schedules with follow-up visits seeking to improve their less-than-optimal hearing aid fittings.11

Figure 3. Clinical best practices, such as real-ear verification measurements, can improve patient satisfaction and reduce excessive use of professional time.
Use of best practices for every patient seen will improve patient outcomes, increase patient satisfaction, and enhance practice efficiency, freeing clinic schedules for more appointments.
Concern #2: Participation with a managed care plan means lower quality patient care.
A 2013 study from Johns Hopkins Bloomberg School of Public Health investigated if patient payment status resulted in delayed care, restricted care, and less access to newer technology.12 The study found that the quality of patient care varied based on insurance status (ie, insured, uninsured, private insurance, public insurance). With the growth of supplemental benefits in hearing healthcare, the potential for poorer quality patient care is a concern. However, from a practical standpoint, there should be no difference in effort or time spent with any patient if patient care protocols incorporate practices that focus on optimizing patient outcomes.
There are several tactics often neglected by hearing care practices that can substantially increase workflow efficiency. Health and medication history forms can be provided to patients before their visit, so valuable appointment time can be spent talking directly with the patient about their hearing needs and concerns. Verifying hearing aid fittings ensures that hearing aid fittings are accurate and appropriate for the patient’s hearing loss, reducing the likelihood of multiple follow-up visits. Using a patient communication needs assessment tool (eg, COSI) can target individual patient communication challenges and help the clinician use appointment time more effectively.
With the known health impacts of untreated hearing loss—including increased risk for depression, dementia, falls, etc—it is critical to focus on hearing aid adoption rates which have increased by little more than 10% in the last 30 years (Figure 2).5,14 Today’s hearing aids are more capable, more versatile, and easier to use than ever before. Yet less than 40% of adults with hearing loss are currently wearing hearing aids.4-6 While cost is not the only issue affecting hearing aid use, coverage with a managed care plan can reduce the barriers to hearing aid adoption and improve the likelihood that patients who need amplification will seek help.4,6,14
Concern #3: Participation with a managed care plan interferes with provider-patient relationships.
Another provider concern is that a managed care plan disrupts the important connection between provider and patient. While hearing aids are an important part of treatment for hearing loss, the line has become blurred between the device itself and patient care.
The internet has become a major source of information about hearing loss and hearing aids, and it is common for consumers to conclude that hearing aids will restore normal hearing. While there are many excellent hearing loss resources available, patients may be investigating treatment options and hearing devices without professional guidance. Managed care plans support hearing healthcare providers by creating member education programs focused on hearing loss, associated health conditions and hearing aids that guide the member to seek evaluation from a network provider.
The hearing aid is only one part of the overall treatment plan for any patient with hearing loss. The patient history and evaluation, hearing aid fitting and verification, and patient instruction and counseling are far more important to patient success than the brand or technology tier of the hearing aid.16-18
Hearing loss has deep emotional impact. It can evoke feelings of shame, embarrassment, anger, hopelessness, and grief. When a patient is attempting to process and understand these difficult emotions but is also confronted with the need to pay for hearing aids, it can be overwhelming. Managed care plans can provide support and reduce this financial burden by assisting the patient with funding for the hearing aids and the professional services associated with the devices.
Concern #4: Participation with a managed care plan takes too much time.
Amid the ongoing pandemic, efficient use of clinic time has become even more difficult. Many practices are experiencing significant staff shortages which directly impact patient care. When faced with the administrative time required to participate with managed care, many providers are unwilling to make the additional effort. Recognizing that quality providers are the key to their success, many TPAs have worked hard to make the credentialing and plan participation process easier.
Some managed care plans have partnered with the Hearing Network Alliance (https://aapan.org/hna) to streamline the credentialing application process. Use of online secure portals makes hearing aid ordering and claims submissions quicker and more accurate. Health-plan sponsored patient websites and blogs are designed to educate patients about hearing loss and provide them with specific information on their health plan benefits and hearing aid coverage.
With more seniors enrolling in Medicare Advantage plans, health plans are promoting the supplemental benefits included in their health plan coverage. When patients contact their health plan to investigate coverage, their benefits are reviewed with them, and they are referred to a participating provider near them. Patients are directed to information that they can access prior to their first hearing healthcare appointment to prepare them to participate in their care and better understand their provider’s hearing aid recommendations.
Summary: Leverage Managed Care to Best Serve Your Practice and Your Patients.
Participation in managed care is new to many hearing healthcare practitioners. It can be difficult to fully understand the benefits and limitations of health plan participation. Just as every hearing care practice is unique, every managed care plan is different, and some may be an excellent fit for your patients and your business—others may not be. As a network provider, patient referrals occur at no cost to your practice. These referrals can lead to better visibility for your practice with both patients and physicians in your area. Asking critical questions and fully investigating managed care plans will lead you to make the best decisions for your practice, your patients and yourself. The next and final article in this series will explore ways to build a successful and sustainable practice while participating with managed care and highlight the benefits of participation.
References
- Freed M, Biniek JF, Damico A, Neuman T. Medicare Advantage in 2021: Enrollment update and key trends. Kaiser Family Foundation website. https://www.kff.org/medicare/issue-brief/medicare-advantage-in-2021-enrollment-update-and-key-trends. Published June 21, 2021.
- Biniek JF, Freed M, Damico A, Neuman T. Medicare Advantage 2021 spotlight: First look. Kaiser Family Foundation website. https://www.kff.org/medicare/issue-brief/medicare-advantage-2021-spotlight-first-look. Published October 29, 2020.
- Freed M, Damico A, Neuman T. A dozen facts about Medicare Advantage in 2020. Kaiser Family Foundation website. https://www.kff.org/medicare/issue-brief/a-dozen-facts-about-medicare-advantage-in-2020. Published Jan 13, 2021.
- Powers TA, Rogin CM. MarkeTrak 10: Hearing aids in an era of disruption and DTC/OTC devices. Hearing Review. 2019;26(8):12-20.
- Carr K. 20Q consumer insights on hearing aids, PSAPs, OTC devices, and more from MarkeTrak 10. AudiologyOnline. https://www.audiologyonline.com/audiology-ceus/course/20q-consumer-insights-on-hearing-34404. Published March 16, 2020.
- Valente M, Amlani AM. Cost as a barrier for hearing aid adoption. JAMA Otolaryngol Head Neck Surg. 2017;143(7):647-648.
- Singleton A, Greene P. Managed care: Threat or opportunity? Hearing Review. 2018;25(1):24-26.
- Cavitt K. Managed care: Some caveats and common sense for hearing care professionals. Hearing Review. 2018;25(1):28-29.
- Amlani AM, Pumford J, Gessling E. Improving patient perception of clinical services through real-ear measurements. Hearing Review. 2016;23(12):12-21.
- Amlani AM, Pumford J, Gessling E. Real-ear measurement and its impact on aided audibility and patient loyalty. Hearing Review. 2017;24(10):12-21.
- Jorgensen LE. Verification and validation of hearing aids: Opportunity not an obstacle. J Otol. 2016;11(2):57-62.
- Mueller GH, Picou EM. Survey examines popularity of real-ear probe-microphone measures. Hear Jour. 2010;63(5):27-32.
- Spencer CS, Gaskin DJ, Roberts ET. The quality of care delivered to patients within the same hospital varies by insurance type. Health Affairs. 2013;32(10):1731-1739.
- Mahmoudi E, Basu T, Langa K, et al. Can hearing aids delay time to diagnosis of dementia, depression, or falls in older adults? J Am Geriatr Soc. 2019;67(11):2362-2369.
- Gallagher NE, Woodside JV. Factors affecting hearing aid adoption and use: A qualitative study. J Am Acad Audiol. 2018;29:300-312.
- Humes LE, Herring C, Kinney DL, Main AK, Quigley TM, Rogers SE. The effectiveness of hearing aids and two service-delivery models in older adults: A randomized double-blind, placebo-controlled clinical trial. Hearing Review. 2017;24(4):12-19.
- Tecca JE. Are post-fitting follow-up visits not hearing aid best practices? Hearing Review. 2018;25(4):12-22.
- Johnson J, Xu J, Cox R. Choosing hearing aid technology for older adults: Examination of user outcomes. Audiology Now [newsletter of Audiology Australia Ltd]. 2015;61:10-13.
CORRESPONDENCE can be addressed to HR or Dr Meyer at: [email protected].
Citation for this article: Meyer C. How to manage in managed care. Hearing Review. 2021;28(10):24-27.