

|

|
| This article was submitted to HR by Carol A. Sammeth, PhD, senior regulatory/clinical specialist for Cochlear Americas and adjunct associate professor of audiology at the University of Colorado-Boulder; and George Cire, AuD, clinical manager of Bone Anchored Solutions for Cochlear Americas, Centennial, Colo. Correspondence can be addressed to [email protected], , or . | |
Both objective and subjective data reported in the research literature, as well as the case study presented in the sidebar of this article, support the contention that the Baha is a satisfactory and beneficial option for those patients with SSD who are seeking help.
Single-Sided Deafness (SSD) is specifically defined for the purpose of this paper as a profound sensorineural hearing loss in one ear, with normal hearing thresholds (<20 dBHL) in the opposite (“normal-hearing”) ear. The unilateral deafness may be present at birth due to congenital malformation, later acquired as sudden idiopathic deafness, or due to acoustic neuroma removal, viral illnesses, or head trauma. Although in the past SSD was sometimes perceived as not producing much handicap, there is in fact fairly substantial evidence that many patients with SSD do experience significant problems.1-3
A person with SSD can usually understand conversation well when listening in quiet, as long as sounds are loud enough. However, speech understanding becomes difficult when they are surrounded by several people talking and trying to listen to someone from the deaf-ear side or in adverse listening situations such as a noisy restaurant (ie, “cocktail party” situation). With only one ear, localization (directional hearing) ability is also lost, so it is impossible to know which way to turn when someone is calling, or, more seriously, from which direction street traffic is coming.
People with SSD who lead an active and busy life are increasingly looking for treatments that may assist them to communicate better in difficult listening situations, miss less of the world around them, and identify from where sounds are coming.
Treatment Approaches for SSD
CROS. The earliest viable treatment approach for SSD was the Contralateral Routing Of Signals (CROS) air-conduction hearing aid.4,5 CROS aids have been available over the years in a number of configurations, including eyeglass frames and behind-the-ear (BTE) or in-the-ear (ITE) hearing aids, with a unit placed on each ear. Sound is picked up by a microphone placed on the deaf ear (transmitter side), and then sent by either hard wire or FM signal to the opposite normal-hearing ear (receiver side) to provide better awareness and understanding of speech and other sounds occurring on the deaf-ear side.
Although some people do well with a CROS, there are some distinct disadvantages and limitations of these hearing aids. They are cosmetically unappealing because they can be bulky and unsightly, and they can be uncomfortable to wear. Further, if the receiver side is too occluding, it can limit direct incidence sound to the normal-hearing ear. Finally, since they are air-conduction amplifiers, they can introduce distortion into the signal that reduces the quality of the sound. Thus, many SSD patients either cannot successfully wear or refuse to wear a traditional CROS aid.
ITE T-CROS. In the late-1980s and 1990s, the transcranial-CROS (T-CROS; or “internal CROS”)6 concept was introduced as an alternative to the traditional CROS aid for SSD patients. In this approach, a high-power air-conduction ITE hearing aid,7,8 or in-the-canal (ITC) or completely-in-the-canal (CIC) hearing aid,9,10 is placed deeply into the canal of the deaf ear. If the aid is set to produce high enough levels of output, the microphone and receiver components will produce physical vibration energy that can be transmitted via bone conduction through the deep portion of the ear canal, transcranially across the skull to the normal-hearing cochlea.
An advantage of T-CROS is that nothing needs to be placed on or occluding the normal ear, and with a deep ITC/CIC fitting there is no unsightly component. However, there are also some clear problems with this approach. In order to get adequate power transmission without feedback, a very deep, closed fitting of the hearing aid casing is required, which is difficult to achieve in practice and can cause significant discomfort and acoustic feedback with jaw movement (such as chewing, yawning, or talking). In addition, there is limited control over the precise amount of sound transmitted, given that the physical fit can vary across ears, and the frequency response/gain of an air-conduction hearing aid is not maximized for this purpose. Finally, ITCs and CICs are often prone to breakdown due to cerumen occluding the microphone inlet, which is particularly a problem with deeper canal fittings. As a result of these limitations, the T-CROS approach never really gained much favor as a treatment approach for SSD.
BTE T-CROS. In 2005, a new device called the “TransEar,” which also uses a T-CROS approach, was marketed for use with SSD patients. This device has a BTE casing with a cord leading to a custom shell that is inserted deep into the ear canal. It works on the same principle as that of a deeply fitted high-power ITC except that the oscillator is intentionally designed into the canal piece to send the transduced mechanical energy transcranially, and the signal processing is reportedly adjusted to maximize bone-conduction transmission. However, to the knowledge of these authors, there have to date been no clinical data published using this device so it is unclear if it provides any greater benefit than the use of a deeply fitted ITC or CROS.

|
| FIGURE 1. The Baha® Auditory Osseointegrated Implant System, showing the titanium implant, abutment, and sound processor. |
In any case, it comes with some of the same potential cosmetic disadvantages of CROS and other T-CROS approaches due to the BTE component, and it may produce wearing discomfort since it also requires a tight and deep ear-canal fitting.
Bone-anchored implant. A final treatment option for these patients, and the topic of this paper, is the Baha® auditory osseointegrated implant, or “Baha implant” for short. Originally called a “bone-anchored hearing aid,” the terminology was subsequently revised to more accurately describe the device, which is implanted in the temporal bone behind the ear and actually osseointegrates with the bone to provide transmission of sound via direct bone conduction.
The Baha implant has been used successfully for more than 30 years in more than 30,000 patients worldwide. The implant is placed in a simple outpatient procedure and does not present a risk of further loss of hearing or damage to the ear. Cleared for use in children over the age of 5 years, originally the Baha implant was used only for conductive and mixed hearing losses as a means to overcome (bypass) the conductive block produced by damage to the outer and/or middle ear. (Authors’ note: Children under 5 years old can use the Baha sound processor with an external Softband [headband] option until they are old enough for implantation.) Then, in 2002, the FDA also cleared the Baha implant as a treatment for SSD.

|
| FIGURE 2. The Baha® implant shown in place on a patient’s head without the sound processor snapped onto the abutment. |
As shown in Figure 1, the Baha system consists of a small titanium implant and abutment, which are placed in the temporal bone behind the ear. The small removable sound processor is simply snapped onto the abutment. Figure 2 shows the implant and abutment in place on a patient.
The surgery for Baha is a simple in-office procedure and, after a 3- to 6-month period during which osseointegration occurs, the sound processor is fitted on the patient and adjusted for appropriate amplification parameters. There is a family of sound processors available for the Baha implant, selected according to the needs of the user and the features desired. Further assistance if needed in very adverse, noisy listening environments can also be obtained by using available options, such as a directional microphone, FM unit, or telecoil.
The Baha Implant for SSD
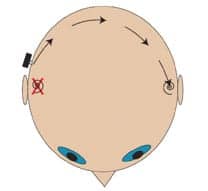
For persons with SSD, the Baha implant is placed on the deaf-ear side to send sound transcranially to the normal-hearing cochlea (Figure 3). However, unlike other T-CROS approaches, it does so in an efficient manner because the energy is delivered directly from a mechanical oscillator that has integrated with the temporal bone. Compared to an external air-conduction hearing aid or a conventional bone-conduction hearing aid used for SSD, the Baha implant produces higher fidelity sound without placing any components on or in either ear. It is cosmetically attractive, often hidden under the recipient’s hair, and comfortable to wear (some patients report they forget they have it on).
|
| FIGURE 3. A schematic illustration of how, in a person with SSD, sound travels intracranially from the Baha implant to the normal hearing cochlea of the other ear. |
All treatment approaches for SSD are intended to overcome the head-shadow effect for sounds from the deaf-ear side (or to help mitigate the effects of noise on the good-ear side), but it is important to note that none provide true binaural processing by the auditory system since there is still only one cochlea receiving sound.
This does not, however, negate the fact that the head-shadow effect has a substantial impact on everyday use so that SSD patients can expect to see significantly improved performance with input from both sides compared to how they perform as a unilateral listener. In recent years, a number of research studies have been done evaluating speech recognition in quiet and in noise for subjects with SSD using a Baha implant, compared to preoperative performance unaided or with use of a CROS hearing aid. Taken as a whole, these studies clearly support the use of the Baha implant for improved performance.11-17 The most effective listening condition for using Baha with SSD has been shown, not surprisingly, to be when speech is on the impaired-ear side and/or noise is on the normal-hearing side.
Localization studies have shown that both the Baha implant and CROS hearing aids produce, on average, essentially chance performance on localization tasks for subjects with SSD.12-15,18 This is not an unexpected finding, because there is still only unilateral input to the central auditory nervous system with these treatment approaches. Interestingly, however, there have been a number of anecdotal reports of possible rudimentary localization abilities for some Baha implant users, and a few individual subjects in some studies have performed at slightly better than chance levels.11,14,16,17 This is presumably due to perception of qualitative differences in the sound coming from the two sides of the head (processed sound coming from the Baha versus unprocessed sound coming directly to the normal-hearing ear).
Finally, there has consistently been improved satisfaction and greater perceived benefit reported by a majority of Baha implant users. Using standardized benefit questionnaires, several studies have compared unaided listening condition to preoperative performance with a CROS hearing aid and postoperative performance with a Baha implant.12-17 Although some individual variability was reported, the overall results of these studies have indicated significantly more favorable scores for the Baha than for the unaided and CROS conditions.
SSD: Evaluation, Fitting, and Verification of Baha Fittings
Each SSD patient should be evaluated individually in terms of Baha candidacy. An elderly person who rarely leaves home may not have any need for treatment, while a CEO of a large company would likely be avidly seeking solutions to the difficulties caused by not hearing with one ear. A real-world trial with a Baha sound processor placed externally on a headband (or Softband for a child) may assist some candidates in deciding whether to proceed with Baha implantation, but it is important to warn that an externally placed device will not produce as high fidelity or quality of sound as the actual Baha implant, due to the loss of high-frequency transmission and output gain that occurs when signals must pass through the skin.
Once the decision has been made to receive an implant, it is important to have a good protocol for evaluating, fitting, and verifying the Baha treatment on the individual to ensure maximal efficacy. One factor to consider in SSD fittings is if the individual patient has higher-than-average interaural attenuation (IA) between the implanted deaf ear and the normal-hearing cochlea, which can occur due to differences in bone quality. This can easily be determined by examination of unmasked bone-conduction thresholds measured with the vibrator placed on the mastoid of the implant ear. If values are higher than 0 dB, some additional gain may be needed in the Baha fitting to provide good audibility in the normal-hearing ear for soft sounds coming from the deaf-ear side. Another factor to consider is that a slightly more high-frequency emphasis response might be useful to help overcome the head-shadow effect, which results primarily in a reduction of high-frequency energy.19
Recently, a very good fitting and evaluation approach for Baha with SSD was published by Snapp and Telischi20 in which they promote the use of speech-in-noise testing in the form of the QuickSIN test.21 This simple time-effective test allows for evaluation and demonstration of the potential positive effects of the treatment. The use of tracks on the QuickSIN test that are spatially separated allows the target speech material (sentences) to be oriented toward the deaf ear and the speech babble “jamming” signal to be oriented toward the good ear. In addition to providing an objective outcome measure in the form of the difference in dB signal-to-noise ratio (SNR) needed for good performance aided versus unaided, it gives the patient a more “real-world” demonstration of how the Baha may provide benefit for the unique communication problems caused by SSD.
Conclusions
Both objective and subjective data reported in the research literature, and case study reports such as the one presented in the sidebar, support the contention that the Baha is a satisfactory and beneficial solution for those with SSD who are seeking assistance. These people might otherwise remain untreated since alternative treatments have often not been well accepted. It is important to remember, however, that a good protocol needs to be utilized for assessment of candidacy, and for fitting and verification of the Baha implant to ensure maximal efficacy for individuals with SSD.

|

|
| FIGURE 4. Unaided audiogram of a young girl with SSD, who received a Baha implant on her left side at the age of 13 years old. | TABLE 1. Preoperative and postoperative speech-in-noise scores (percent correct) and self-assessment questionnaire results (higher values indicate better perceived performance) for the SSD patient whose audiogram is shown in Figure 4. |
Case Study Using Baha
Figure 4 and Table 1 illustrate a case study of Baha implant use in a typical SSD patient (courtesy of Lisa Christensen, AuD, of Arkansas Children’s Hospital, Little Rock, Ark). Shown in Figure 4 are the unaided puretone audiometric threshold data of this young female patient who received a Baha implant and abutment on her deaf ear at the age of 13 years and 10 months old. After a sufficient period of healing and osseointegration, she was fitted with a Baha Divino® sound processor.
Shown in Table 1 are this patient’s preoperative (unaided) and postoperative (Baha-aided) test results using sentence materials from the Hearing-In-Noise Test (HINT),22 an objective measure of speech recognition. Results are presented for testing at three different fixed signal-to-noise ratios (SNR), with sentences directed toward the deaf ear and noise directed toward the good ear (ie, loudspeakers placed at 90° and 270° azimuths). Scores are also shown in Table 1 for the Speech, Spatial and Qualities self-assessment questionnaire (SSQ),23 which documents patient-assessed perception of their performance in each of three areas: speech, spatial hearing, and quality of hearing.
As can be seen, substantial objectively measured and patient-perceived improvements in performance are observed with the Baha implant compared to preoperative unaided performance. Additionally, this patient reports consistent and regular use of the Baha.
References
- Giolas T, Wark D. Communication problems associated with unilateral hearing loss. J Speech Hear Disord. 1967;41:336-343.
- Choissoine-Kerdel JA, Baguley DM, Stoddart RL, et al. An investigation of the audiological handicap associated with unilateral sudden sensorineural hearing loss. Am J Otol. 2000;21:645-651.
- Hausler R, Colburn S, Marr E. Sound localization in subjects with impaired hearing. Acta Otolaryngol Suppl. 1983;400:1-62.
- Harford E, Barry J. A rehabilitative approach to the problem of unilateral hearing impairment: the contralateral routing of signals. J Speech Hear Disord. 1965;30:121-138.
- Punch J. CROS Revisited. Asha. 1988;February:35-37.
- Valente M, Potts LG, Valente M, Goebel J. Wireless CROS versus transcranial CROS for unilateral hearing loss. Am J Audiol. 1995;4:52-59.
- Sullivan RF. Transcranial ITE CROS. Hear Instrum. 1988;39(1):11-12, 54.
- McSpaden J, McSpaden C. A method of evaluating the efficacy and effectiveness of transcranial CROS fittings. Audecibel. 1989;Spring:10-14.
- Bauman N, Braemer M. Using a CIC hearing aid in transcranial CROS fittings. Hear Jour. 1996;49(3):27-28, 45-46.
- Hayes D, Chen J. Bone conduction amplification with completely in the canal hearing aids. J Am Acad Audiol. 1998;9:59-66.
- Vaneecloo FM, Ruzza I, Hanson JN, et al. The monaural pseudo-stereophonic hearing aid (BAHA) in unilateral total deafness: a study of 29 patients. Rev Laryngol Otol Rhinol (Bord). 2001;122(5):343-350. (English abstract only; article in French.)
- Bosman AJ, Hol MK, Snik AF, et al. Bone-anchored hearing aids in unilateral inner ear deafness. Acta Otolaryngol. 2003;123(2):258-260.
- Niparko JK, Cox KM, Lustig LR. Comparison of the bone anchored hearing aid implantable hearing device with contralateral routing of offside signal amplification in the rehabilitation of unilateral deafness. Otol Neurotol. 2003;24:73-78.
- Wazen JJ, Spitzer JB, Ghossaini SN, et al. Transcranial contralateral cochlear stimulation in unilateral deafness. Otolaryngol Head Neck Surg. 2003;129(3):248-254.
- Hol MK, Bosman AJ, Snik AF, et al. Bone-anchored hearing aid in unilateral ear deafness: a study of 20 patients. Audiol Neurotol. 2004;9(5):274-281.
- Hol MK, Bosman AJ, Snik AF, et al. Bone-anchored hearing aids in unilateral inner ear deafness: an evaluation of audiometric and patient outcome measurements. Otol Neurotol. 2005;26(5):999-1006.
- Lin LM, Bowditch S, Anderson MJ, et al. Amplification in the rehabilitation of unilateral deafness: speech in noise and directional hearing effects with bone-anchored hearing and contralateral routing of signal amplification. Otol Neurotol. 2006;27(2):172-182.
- Wazen JJ, Ghossaini SN, Spitzer JB, Kuller M. Localization by unilateral BAHA users. Otolaryngol Head Neck Surg. 2005;132(6):928-32.
- Shaw EAG. Transformation of sound pressure level from the free field to the eardrum in the horizontal plane. J Acoust Soc Am. 1974;56:1848-1861.
- Snapp H, Telischi F. A recommended protocol for Baha assessment and verification for individuals with single-sided deafness. Audiol Today. 2008;20(4):21-27.
- Etymotic Research. QuickSIN Speech-in Noise Test Version 1.3. Elk Grove Village, Ill: Etymotic Research; 2001.
- Nilsson M, Soli S, Sullivan J. Development of the Hearing in Noise Test for the measurement of speech reception in quiet and noise. J Acoust Soc Am. 1994;9(2):1085-1099.
- Gatehouse S, Noble W. The Speech, Spatial and Qualities of Hearing Scale (SSQ). Intl J Audiol. 2004;43:85-99.
Citation for this article:
Sammeth C, Cire G. Effectiveness in Treating Single-Sided Deafness with the Baha System. Hearing Review. 2009;16(4):34-41.


