Phonak ABCs of eAudiology #3: 10 Steps to Clinical Applications & Providing Feedback for eAudiology
The Phonak ABCs of eAudiology is a handbook of step-by-step guides for incorporating eAudiology and Phonak eSolutions into daily hearing care practice. Each guide has been written by a renowned international expert in this field. A comprehensive range of considerations have been broken down into easy-to-follow steps towards practice implementation. Following the 10 steps in this series of implementation guides could see hearing care professionals up and running with eAudiology services in your practice very soon, benefiting from improved workflows and cost savings, providing your clients quality care in a way which is most convenient to them.
When conducted via eAudiology, effective communication between hearing care practitioners and patients and their significant others is dependent on both technical and interpersonal factors. It is important to recognize that technology may potentially depersonalize relationships, produce conversational impediments (eg, stemming from a lack of stability of an Internet connection), and result in sensory and non-verbal limitations and challenges. Interpersonally, eAudiology communication may be affected by underdeveloped norms regarding “typical” conversational discourse and social distancing. Despite these challenges, most research on eAudiology suggests patients experience good clinical outcomes and high levels of satisfaction.
Where to start?
Step 1
Evaluate need in your clinic. Factors to consider include the location of patients and potential patients (eg, rural vs. urban), ease of transportation (eg, road conditions, access to public transportation options), and personal factors such as health-related mobility and lifestyle. Similarly, evaluate technological feasibility. Are the hardware, software, and IT connectivity sufficient to support eAudiology applications?
Step 2
Are the stakeholders in place? Evaluate interest from the clinic staff regarding willingness to design, install, learn new protocols, and deliver hearing healthcare via eAudiology. eAudiology success is critically dependent on stakeholder buy-in. Similarly, survey current patients to gauge their interest in having an eAudiology option. Locations may vary in the extent to which a meaningful proportion of a clinic’s clientele are comfortable with eAudiology to warrant initial investment.
Step 3
Decide on a suitable platform for the clinical tasks you wish to conduct via eAudiology (eg, remote otoscopy, counseling, hearing instrument fitting and adjustment, etc…), and conduct dry runs to ensure systems are operating as expected.
Step 4
Therapeutic alliance and rapport are as important in eAudiology conferencing as they are in face-to-face care, and thus, it is important to establish interpersonal conditions necessary for effective patient care. Good rapport leads to an alliance between all stakeholders that enables cooperative communication and the willing disclosure of sensitive information. Importantly, spend the time necessary to build rapport when communicating via videoconferencing.
Step 5
Be mindful that there is significant evidence that patients are able to quickly adapt and establish rapport with a telemedicine provider1. Feel confident that there is good reason to suspect that patients and their significant others are able to provide information and to be as forthcoming during eAudiology appointments as they would be with face-to-face appointments.
Step 6
Recognize that patients and significant others may alter their appearance and communication styles when communicating via an information communication technology. Examples include being more courteous or meticulous about their appearance.2
Step 7
In addition to patients and significant others altering communication patterns, recognize that practitioners need to adjust communication patterns in order to accommodate to the medium. This will require flexibility and creativity when conferring empathic gestures (eg, overcoming the inability to provide a reassuring touch to a patient).
Step 8
Challenge assumptions. Although perhaps counterintuitive, there is the viewpoint that telemedicine may actually be better suited than face-to-face appointments when delivering bad news3. In face-to-face communication, patients are not only attempting to absorb bad news, they are also faced with the task of engaging in challenging interpersonal conversation. From this viewpoint, telemedicine operates as a buffer by providing patients with more space to process bad news, free one’s gaze from the practitioner, and to hear news in a more comfortable (ie, home) environment.
Step 9
Solicit feedback from staff and patients. Provide surveys throughout different stages of the patient’s care in order to evaluate patient satisfaction, if adjustments to operating procedures are necessary, and whether additional training is required.
Step 10
Assuming successful implementation, communicate the availability of eAudiology services at your clinic more broadly. Doing so represents a means by which to increase accessibility to audiology services and to distinguish your practice.
To download a PDF of the article, please click here: 10 Steps to Clinical Applications & Providing Feedback for eAudiology
Are you up to the challenge?
Test your ability to establish rapport with a patient via eAudiology. For a patient who is scheduled for a face-to-face appointment, ask to meet with them beforehand via videoconferencing and assess what works (and what may not work) when developing your therapeutic relationship.
Other Articles in the Phonak ABCs of eAudiology series below:
| 1. | Licensure and Stakeholder Support | William Campbell |
| 2. | Optimizing Your eAudiology Environment | Danielle Glista, PhD |
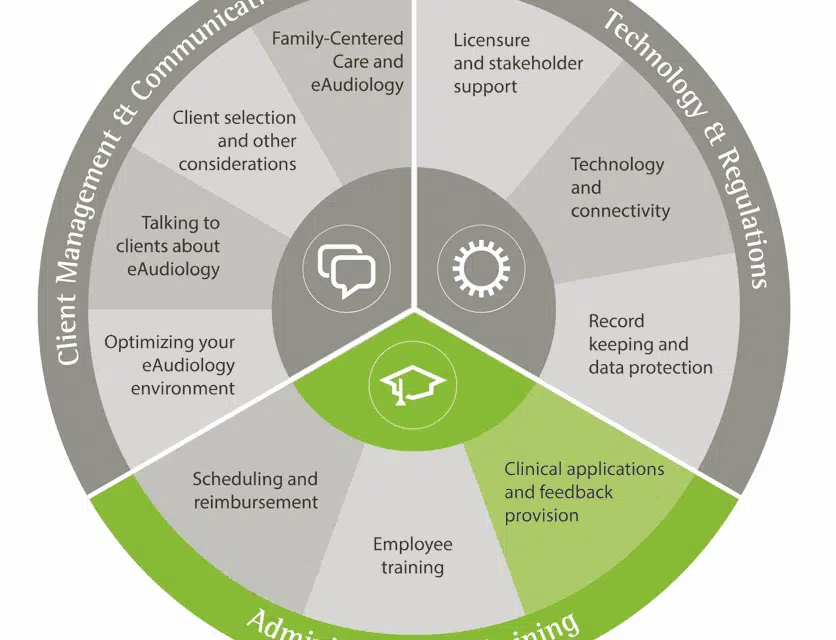
| 3. | Clinical Applications and Feedback Provision | Gurjit Singh, PhD |
| 4. | Employee Training | Karen Muñoz, EdD |
| 5. | Scheduling and Reimbursement | Rachel Higginbotham, AuD |
| 6. | Technology and Connectivity | Jean Anne Schnittker, AuD |
| 7. | Talking to Clients about eAudiology | Gina Angley, AuD |
| 8. | Client Selection and Other Considerations | Evelyn Davies-Venn, PhD |
| 9. | Family-centered Care and eAudiology | Joseph Montano, EdD |
| 10. | Record Keeping and Data Protection | William Campbell |
References
1. Ghosh GJ, McLaren PM, Watson JP. Evaluating the alliance in videolink teletherapy. J Telemed Telecare. 1997;3(1):Supplement 33-5.
2. Modai I, Mahmoud J, Kurs R, Barak P, Hanan I, Kitain L. Cost effectiveness, safety, and satisfaction with video telepsychiatry versus face-to-face care in ambulatory settings. Telemedicine and e-Health. 2006;12(5)..
3. Krishnan N, Fagerlin A, Skolarus TA. Rethinking patient-physician communication of biopsy results—The waiting game. JAMA Oncol. 2015;1(8):1025-1026.

About the Author: Dr Gurjit Singh is a Senior Research Audiologist at Sonova Holding AG, an Adjunct Lecturer at the University of Toronto, and an Adjunct Professor at Ryerson University. In addition to being a clinical audiologist, Gurjit completed his PhD in cognitive psychology at the University of Toronto and a masters in social psychology at the University of Waterloo. Gurjit’s research interests include eAudiology, factors that contribute to speech understanding in noise, emotion, and clinical decision-making.