Upon biting down, the condyle of the jaw moves closer to the ear canal, compresses the cartilage, and reduces the canal diameter. Upon opening the mouth, the cartilage is pulled forward and the canal expands. The amplitude to which the canal widens depends on the subject. These anatomically driven changes in canal dimensions are the cause for poorly fitting earmolds.
Open, Closed, or Both?
While the changes in the ear canal size and shape are real and obvious, the manner in which ear impressions should be taken is debated. Commonly one of three techniques is used: closed/relaxed mouth impression, chewing impression, or open mouth impression. Impressions can also be made with the multilayer method.
Closed/relaxed-mouth impression. In this technique, the patient behaves naturally during impression syringing and curing. They may talk or just relax for the time the material cures in the ear.
Chewing impression. In this method the patient is encouraged to smile, talk, and chew vigorously as soon as the impression material is syringed into the ear. All these actions are meant to produce a more natural impression that notes these changes.

|
is senior supervisor for shell manufacturing with Oticon Canada, Kitchener, Ontario, and also serves as an adjunct instructor at the Pennsylvania College of Optometry, School of Audiology, located in Philadelphia. For Part 1 of this article, see the April issue of HR or visit www.hearingreview.com. |
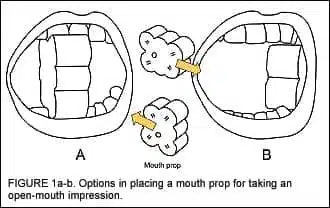
Open-mouth impression. This technique captures the magnitude of the canal widening with mouth opening.1 In order to take an open-mouth impression, a patient opens their mouth wide before the impression material is injected, holds their mouth open during the injection, and does not let their mouth close until the material is fully cured. Because holding the mouth wide open can be uncomfortable, the use of a mouth prop is recommended.
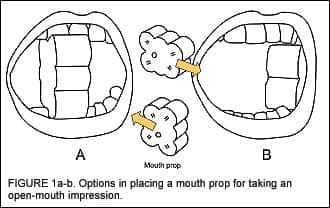
A mouth prop can be used in two ways. First, it can be inserted upright between the front teeth (Figure 1a). This will allow for making two impressions simultaneously and this method is satisfactory in most cases. Still, some feedback may occur when the patient chews food predominantly on one side.
The other method is to insert the prop lengthwise in the corner of the mouth at the side the impression is taken (Figure 1b). This will permit taking only one impression. If an impression from the other ear is needed, another mouth prop must be used in the same manner. This second method produces impressions that are anatomically more accurate and ensures that the resulting hearing instruments are less susceptible to acoustic feedback, particularly when the client is eating/chewing.
The use of a mouth prop in any manner is better than not using one at all. The mouth prop should remain in the mouth as long as the impression cures.
Multilayer impression. In this technique, the impression is taken in several stages using two or three impression materials possessing different viscosity. Then the effectiveness of the impression seal is tested in the patient’s ear.2 The impression is considered finished only if it provides an airtight seal. This method is time consuming and should be considered only in situations where other techniques did not produce a tight impression.
Impression-Taking: The Basics
Inserting the otoblock. All ear impressions can and should be taken with an otoblock inserted past the second bend of the ear canal. The use of the otoblock not only prevents impression material from reaching the eardrum, but also helps to replicate the shape of the ear canal and, most importantly, the flexibility of the canal cartilage.
When impression material is injected, the material flows up against the otoblock, spreads, and stretches the cartilaginous canal tissue out toward the ear aperture. The canal opens up and its increased diameter is captured on the impression. This process is critical in order to build a comfortable and feedback free earmold. In contrast, with a shallow otoblock position, the impression material will not stretch the cartilage within the seal area, and the resulting earmold may fit loosely, have retention problems, and be susceptible to acoustic feedback. (Author’s Note: In the following text, earmolds and ear shells will be collectively referred to as “earmolds” to avoid repetition. When a distinction between the two terms is needed, each will be used separately.)
To insert an otoblock, place the block in the opening of the ear canal with your fingers or a pair of tweezers. Gently pull up the back of the ear, as you would for otoscopic examination. Then, using the earlight, slide the block into the ear canal and up past the second bend. Your little finger should be braced against the side of the head to prevent ear injury should the patient make a sudden movement. Using the earlight will allow you to see the penetration, the blockage of the canal, and the block’s position. Do not push the otoblock straight in, but rather gently ease it in by pushing top and bottom on sides of the block so that you are walking the otoblock slowly into place. Make sure you have inserted the block past the canal second bend, and verify its proper position using the otoscope. When inserting vented otoblocks, use an earlight with a slotted tip.
Mouth prop. When the otoblock is properly situated in the ear canal, insert a mouth prop into the patient’s mouth as discussed previously.
Mixing the impression material. Mix impression material according to the manufacturers guidelines. If you wear gloves, use a mixing pad and a spatula (a method that Westone refers to as “spleading”). Mixing must be thorough but fast. Also keep in mind that products containing sulfur—which is often found in latex gloves and hand lotions—can react with impression material, preventing proper setting.
While taking ear impressions for large ears, prepare more than one dose of silicone for each ear. Measuring syringes can be more convenient for this than measuring spoons or pre-measured packets. To maintain proper proportions of mixing, opt for a one-to-one silicone and measure out 7 ml or 8 ml of each putty.
Impression materials provided in cartridges are mixed automatically when the silicone is dispensed into the ear. After attaching a cartridge with a mixing canula to the injector, repeatedly squeeze the trigger until the silicone appears at the end of the mixing canula. Bleed a small amount of the mixed silicone and check that both components mix thoroughly. If a syringe is used, depress the plunger until the material starts to flow out of the tip.
Inserting the impression material. Pull the pinna up and back and insert the tip of the canula or syringe far into the external ear canal. Do not seal the ear canal with the tip when you start filling the ear.
If you use a syringe, you need to see the moment the impression material comes out from the canal and covers the tip to a depth of about 3 mm. Continue filling the ear and simultaneously withdraw the syringe keeping the tip imbedded in the silicone. If you use a pistol injector, start withdrawing the mixing tip from the canal just before the material touches the canula. This is called the leading technique. If the silicone covers the canula, the finished impression may have voids and air-pockets.
After the ear canal is filled, syringe the material into the concha. First, fill the undercut at the antitragus, then move up and fill in the helix area. You need to see the material coming back from the undercuts before you proceed to the next area. Finish the impression by filling the rest of the concha. If the impression material is syringed into the center of the concha, air will be trapped in the undercuts and the impression will have voids. The whole operation of filling the ear should be one complete motion.
Let the material cure in the ear undisturbed. Do not touch it or press it into the ear. Kieper3 found that making a “tighter” impression by pressing the material further into the ear creates a worse—not better—seal for the resulting earmold.

Inspecting, marking, and mailing. Before an impression is mailed to the lab, carefully check that it is suitable for the hearing instrument to-be-made: If a long canal is requested, the canal portion on the impression should be adequately long. If a full helix or helix lock is needed, the helix portion on the impression must be fully imprinted. If a large vent is necessary, the diameter of the canal area on the impression is to be at least 1 mm larger than the diameter of the vent prescribed.
For a monaural fitting, sending one satisfactory impression to the earmold lab is enough. However, if two impressions taken from the same patient’s ear are sent, explain the reason on the order form and mark the impressions clearly for easy identification. If the two impressions are open-mouth and closed-mouth impressions, code the open-mouth impression with the letter “O” and the closed-mouth impression with the letter “C”. If the earmold is to be made with a long canal, request that the canal tip in the impression be tapered.
Ear Canal Dynamics
For years, earmold labs have been unable to agree on which technique and material result in the best impression: some labs recommend soft low-viscosity silicones, some prefer medium viscosity, while others advise the use of a firmer higher-viscosity silicone. Recommendations relative to mandibular movements also vary. Certain labs insist on having the patient chew, others prefer impressions taken while the patient’s mouth is relaxed or open. A considerable number of labs claim that the technique and material are irrelevant as long as the impression is complete. With all this contradictory advice, clinicians wonder, “Does it really matter how the impression is taken? If it does, who is right? What will result in the best fit for my patient?”

Axial Magnetic Resonance images5 provided in Figure 2a-b demonstrate the longitudinal axis and size of the condyle, and show the effect of jaw position relative to the ear canal. The condyle of the mandible has been outlined to facilitate its identification, and the border between the cartilaginous and osseous regions has been outlined by a solid white line. Note the substantial width of the condyle and its close proximity to the anterior aspect of the ear canal with at least two-thirds of it being in front of the cartilaginous region of the canal. This clearly visualizes the opportunity for its significant influence on canal activity. With the opening of the mouth (Figure 2b), the condyle moves forward, pulls the cartilage in front of the ear canal, and expands the canal.
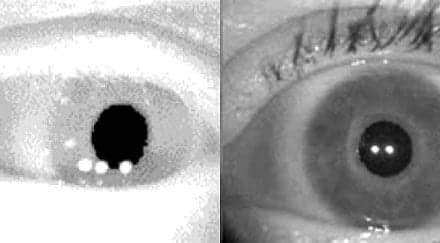
Comparing digital images of open-mouth impressions and closed-mouth impressions made on 172 subjects, Oliveira5 found that open-mouth impressions commonly resulted in wider canals. In 25% of the ears, the canal was stretched 8 mm3 or more, which is an equivalent of a 3 mm vent (Figure 3).
Data in another study6 showed that 36 of 67 subjects (54%) had asymmetrical changes in the ear canal volume: With the opening of their mouth, one ear canal would exhibit an increase in the canal volume greater than 5% compared to the other ear. A 5% increase in the canal volume creates a 2 mm vent for an average ear canal. Sound leakage that occurs through this occasional, uncontrolled and undesirable “venting” can be—and often is—a nightmare in hearing instrument fittings.
|

|
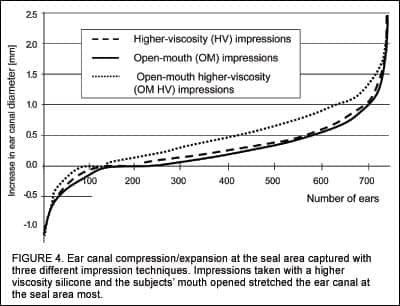
Pirzanski and Berge7,8 compared ear impressions taken with various techniques and materials from both ears of 744 subjects to further investigate the nature and extent of ear canal dynamics. The impressions were taken by the audiologists enrolled in the distance education AuD degree program at the PCO School of Audiology.9 The research method compared the diameter of the ear canal in the anterior-posterior direction on four ear impressions taken from the right ear and four impressions from the left ear of each subject. The first two sets of impressions from each ear were made with a low viscosity silicone and a higher viscosity silicone, with the subjects’ mouth closed. The two other impressions were taken with the subject’s mouth closed and mouth open, using a higher viscosity silicone.
To find if there were any parallels between this and previous research, the data obtained on ear canal expansion/compression due to jaw actions was compared with the data from Oliveira.6 The dotted line in Figure 3 is the linear increase in the ear canal diameter in the anterior-posterior direction with mouth opening. While there were some differences in the compression area, in the expansion area the similarity of both studies was striking.
Figure 4 illustrates ear canal expansion/compression measured for all 1488 ears (744×2) with three different impression techniques. The data for each curve were sorted from the smallest to the largest value. The data for each curve were sorted from the smallest to the largest value. It was a surprise to find that the population of these subjects had their ear canals expanded with mouth opening almost as much as with a more viscous silicone. The curve for the open-mouth higher-viscosity (OM-HV) condition showed a much greater canal widening than the other two conditions.
Further analysis of the OM-HV impressions showed that (again, with the data sorted from the smallest to the largest value) the right ears of the subjects were as dynamic as the left ears (Figure 5). In fact, the two curves look almost identical. This does not mean that the two ears of each subject had similar dynamics. In fact, they did not. The rugged third curve illustrates the actual expansion in the right ear canal with the corresponding left ear of the same subject. Obviously, there was asymmetry in dynamics in the majority of the subjects: 66% of pairs of ears exhibited a difference in the canal expansion greater than 0.2 mm. This finding was consistent with previous research.7
Most patients have asymmetrical ears in terms of the canal cartilage softness and the extent to which the canal is affected by mandibular movements. That is why, in binaural fittings, the hearing aid made for the more dynamic ear canal is at a higher risk of a fitting problem than the less dynamic ear.
The impact of asymmetry in ear canal dynamics is also evident in the structure of hearing aid remakes. A study by Pirzanski and Berge10 investigated a total of 337 cases of patients fitted binaurally where one or both instruments required a remake. In all cases the patients had similar hearing loss in both ears, and the aids were built with consecutive serial numbers (eg, it was assumed that one technician made both shells and assembled both instruments). The results showed that binaural remakes were the least common type, accounting for only 32% of all remakes. Hearing aid remakes for the left ears were at 35%, and for the right ears at 33%. This 68% (35%+33%) of remakes occurring only for one hearing aid in a binaural fitting corresponds surprisingly well with the fact that over 50% of human ears exhibit asymmetry in ear canal dynamics significant enough to lead to a fitting problem.6
Figure 6 shows ear canal dynamics from yet another perspective. Employing digital imaging technology, an image of a closed-mouth low-viscosity (CM-LV) impression and an OM-HV impression were combined. When the canal area was crosscut at various levels, an interesting pattern in the canal expansion appeared. First, the OM-HV impression was larger in most areas. Second, the canal did not expand evenly in all anatomical directions like a balloon would; it expanded only in certain areas to a varying degree, all the way between canal second bend to the canal aperture, reaching a maximum of 0.8 mm. Interestingly, the area of maximum stretching is shifting from the anterior area in section 1 to inferior area in section 3, and then partially returning to the anterior area in section 5. It is clear that expansion of an ear canal is unique, and often different between both ears of the same person.
After reading the above, one can appreciate the fact that, with this kind of prevalence of soft and dynamic ear canals, fitting problems should be much more frequent—and very few hearing aids should be fitted successfully. This would happen if earmold labs did not coat ear impressions with wax prior to casting the earmold or earshell. In fact, all earmold labs coat ear impressions, and this makes fitting hearing instruments possible and successful.

Ear canal dynamics not only adversely affect the acoustic seal of the hearing aid and cause retention problems, but may also make the instrument uncomfortable to wear. Ear soreness and irritation are often reported with earmolds that are loose and subsequently require frequent pushing back into the ear. The friction between the earmold and canal will often irritate the ear.
Patients with dynamic ear canals may complain that the sound cuts off. The misperception is that mandibular movements rotate the earmold or shell in the ear canal to the extent that the sound bore is partially or totally blocked by an ear wall. However, this isn’t the explanation. The apparent reduction in the instrument loudness in conjunction with mandibular movement actually results from the ear canal widening when the patient opens their mouth. The resulting stretching can be major—in some ears reaching 2 mm (Figure 7). With the increased volume of the canal, the receiver has to move a larger volume of air than previously required. Since the hearing aid’s amplification level has not changed, the sound pressure in the expanded canal is considerably lower and the instrument’s loudness reduced to the point that the hearing aid may be perceived as dead.
This effect of the sound going on and off primarily affects low-to-moderate power hearing aids where the sound leaking from the canal is not strong enough to trigger feedback. In higher powered hearing aids, the expansion of the ear canal will allow for enough sound to radiate back to the microphone and cause feedback.
At this point, it may be apparent to the reader that taking open-mouth impressions with more viscous impression materials is beneficial and desirable for patients possessing soft and active ear canals. This is correct. The question is whether or not canal dynamics can be predicted ahead of time and correctly quantified during patient examination. If yes, the volume of hearing aid remakes could be reduced through either requesting a thicker wax coating on the impression taken from soft/dynamic ear canals or employing the OM-HV technique.
To find the answer, Pirzanski and Berge8 asked audiologists to evaluate each ear of the 744 subjects in their study and classify the ears as having canal cartilage that is “soft,” “medium soft,” or “firm.” Mandibular activity in the ear canal was classified as “none,” “moderate,” or “severe.” These perceptions were then compared with impression measurements. Stretching in the ear canal below 0.5 mm was considered minor, widening from 0.5 mm to 1 mm was moderate, expansion over 1 mm was classified as significant. The results were surprising: For canals classified as soft, medium soft, and firm, the number of predictions consistent with the measurements were 8%, 16% and 83%, respectively. Inaccurate predictions regarding ear canal softness were made for 66% of the ears. The predictive value of observations relative to the magnitude of TMJ movements was 81% accurate for inactive ear canals, and 17% and 10% accurate for ear canals with moderate and severe TMJ movement, respectively. The total of inaccurate observations concerning TMJ movements was 52%. These findings were consistent with Oliveira’s research.6

If the ear canal is firm and not affected by mandibular movements, the OM-HV impression will not differ from an impression taken with any other technique. However, if the ear canal is soft and/or active, the OM-HV impression will most precisely capture the canal dynamics.
Lowering Remake Rates
The above directions for taking OM-HV impressions may be received by certain clinicians with reservation. Their clinical experience may be that they encounter too few remakes to foresee any tangible benefit from altering their impression taking technique. However, there is a flaw in this reasoning: The majority of hearing aids returned to manufacturers due to fitting problems come from clinicians who consider the number of their remakes to be very low.
Consider that more than a half of all hearing aid remakes occur within the first 12 weeks of hearing instrument use.8 This is difficult to justify if we keep in mind that custom hearing aids are manufactured from impressions taken individually from patients’ ears. Therefore, patients’ satisfaction with new hearing instruments should be the best—not the worst—at the beginning of the fitting.
Taking OM-HV impressions will not eliminate all remakes, but it will reduce their incidence. A comparison of the number of remakes experienced by two clinicians working in the same office and using the same impression material found that the clinician who used the closed-mouth technique had 57% more remakes compared with the other who routinely took open-mouth impressions. A review of 1900 earmold fittings completed in a hospital setting found that a switch from a lower viscosity to a higher viscosity silicone reduced the percentage of remakes from 10-14% to 5%, a remarkable difference!10 In both studies, prior to the change, the clinicians involved considered their remake rates already low. Based on research data, there is potential to lower the number of remakes in new hearing aids and earmolds by 50%, provided OM-HV impressions are regularly taken.
Some earmold labs have reservations towards the use of OM-HV impressions. They are aware that an open-mouth impression may resolve, for example, a problem with acoustic feedback, but may create another with discomfort. This may happen if the canal tip in the impression is not tapered. Impression tapering should be the routine procedure in earmold manufacturing. The OM-HV impression is a tighter impression that expands the ear canal both across and lengthwise, as shown in Figure 7. The across-stretching is desirable and beneficial for the instrument fitting; the lengthwise expansion is not. If not corrected, it leads to manufacturing an earmold that will have the canal area longer than the canal in the patient’s resting ear. As a result, the earmold may be uncomfortable.
The necessary impression correction for this problem is called canal tip tapering. Canal tip tapering is a procedure carried out by the earmold lab technician in which the medial end on the canal in the impression is trimmed to ensure earmold comfort and easy insertion without compromising the instrument’s ability to stay securely in the ear and seal effectively.
In my opinion, canal tip tapering should be carried out in all fittings where the earmold or earshell is made with a long canal extending past the second bend. The two exceptions to this are musician’s earplugs and transcranial fittings. The former must seal the ear canal at the bony area to provide effective noise attenuation without the occlusion effect; the latter must seal deeply to provide gain high enough for stimuli to produce crossover to the opposite cochlea and improve sound localization.
Coming in Part 3: Impressions and earmolds/earshells for pediatric patients.
References
1. Pirzanski C. An alternative impression-taking technique: the open-jaw impression. Hear Jour. 1996;49(11): 30-35.
2. Pirzanski C. Secrets of the multilayer impression-taking technique. The Hearing Review. 2000;7(10):22,24,26-27. Available at: www.hearingreview.com/articles.ASP?articleid=H0010F01
3. Kieper R, Berger E, Lindgren F. An objective assessment of the effect of ear impression technique on real-ear attenuation of earmolds. Indianapolis: Cabot Safety Corp; 1991.
4. Garcia H, Staab W. Solving challenges in deepcanal fittings. The Hearing Review. 1995;2(1): 34-40.
5. Oliveira R, Hoeker R. Ear canal anatomy andactivity. Sem Hear. 2003;24(4):265-275.
6. Oliveira R, Babcock M, Venem M. The dynamic ear canal and its implications. The Hearing Review. 2005;12(2):18-19,82. Available at: www.hearingreview.com/Articles.ASP?articleid=H0502F01
7. Pirzanski C, Berge B. If you blame buffing for bad fittings, you’ve probably given the wrong impression. Hear Jour. 2004;57(2):40-45.
8. Pirzanski C, Berge B. Ear canal dynamics: Facts vs perception. Hear Jour. 2005;58(10):50-58.
9. Pirzanski C, Berge B. Earmold acoustics and technology. Doctoral level course, PCO School of Audiology. Available at: www.audonline.org
10. Pirzanski C, Berge, B. Is the end near for acoustic feedback? The Hearing Review. 2004;11(4):18-23. Available at: www.hearingreview.com.
Correspondence can be addressed to HR or Chester Pirzanski, Oticon Canada, 500 Trillium Dr, Unit 15, Kitchener, ON N2R 1A7; e-mail: [email protected]