By Donald J. Schum, PhD
The new class of IIC hearing aids provides an entirely new set of options for first-time users—provided they are candidates for the devices. Likewise, mini-BTEs and RITEs also open up new possibilities. Here are some important considerations when selecting IICs, mini-BTEs, and RITEs for new users.
Getting a potential hearing aid user to embrace the concept of wearing amplification can be tricky. Adults with acquired hearing loss may show reluctance for a variety of reasons (Schum, Behrens, and Weile, Oticon white paper, 2011). Clearly, one of the most dominant reasons why potential users delay or avoid getting amplification is concerns about how they will look wearing hearing aids. Although the impairment may well be creating true communication difficulties, concerns about “what others may think” keep many from taking action.
Over the last couple of decades, there have been a variety of attempts by the hearing aid industry to produce hearing aids that are more appealing and more discreet than previous styles. Completely-in-the-canal (CIC) hearing aids were specifically designed to create a potentially invisible solution. The reality is that, for most ears, the faceplate of a CIC can still be seen. CICs have the potential side effects for many patients of occlusion, feedback, handling problems, and annoyance or discomfort.1
For more than the last 5 years, there has been a broad selection of small behind-the-ear (BTE) products made in nontraditional shapes and colors. These products usually also offer either thin-tube or receiver-in-the-ear (RITE) coupling. The combination of a smaller, more discreet size, along with nontraditional shapes and colors, have improved acceptance by many first-time users. Because of the discreet appearance and lower risk of side effects, many professionals have gravitated away from CICs and toward these new mini-BTEs and RITEs.
Over the past couple of years, due to further miniaturization of hearing aid components, a new generation of “invisible” devices—the invisible-in-the-canal (IIC)—have entered the marketplace. These have taken the form of extended wear disposables, instant-fit IICs, and custom-fit IICs. We consider a true IIC to be a product that sits deeper than the second bend of the ear canal. As can be seen in Figure 1, for those ears that can accommodate the device, a true invisible fit can be achieved.
Because of the emergence of potentially truly invisible products, many professionals now face the decision about balancing the portfolio of products they fit with devices that once again sit deep in the ear canal. Concerns about having to face the long-standing side effects that came with CICs may create hesitancy on the part of the dispensing professional to use IICs.
At Oticon over the past year, we have introduced two products in the Intiga family that are specifically targeted toward first-time users: the Intiga RITE and the Intigai IIC. We believe that both products offer excellent technology for the first-time user. However, because of the style differences, neither the technologies used in these products, nor the risk of side effects, are identical.
This article discusses the audiological and non-audiological aspects that differentiate these two products. Such information is essential for the professional when discussing style options with new users.
Agenda of the First-time User
The discussion starts with identifying what we know about the mind-set of the typical first-time user. In our recent white paper (Schum, Behrens, and Weile, 2011), we detail a classic time order to the concerns of the first-time user:
- Appearance,
- Acceptance, and then
- Performance.
Of course, this is a generalization, but for the patient who is hesitant to use amplification due to stigma-related concerns, how the device looks will often dominate their thoughts when selecting a product.
Once the patient comes to terms with the physical appearance of their selection, then it is essential that their initial exposure to amplified sound is positive. There is always a risk that the newly fit devices will be rejected during the first days of use. Therefore, making sure that sound is clear and pleasant, with a minimal amount of side effects, is a strategy that the professional needs to employ in order to keep the fitting moving forward in a positive direction.
Finally, once the patient is comfortable with the appearance and has experienced amplified sound in a positive way, then communication performance comes into sharper focus.

Any trepidation may be reinforced if the initial sound experiences are not positive. It is not that benefits are not important to the first-time user; it is that they may not be the only thing on the patient’s agenda.
With this sequence of issues—appearance, acceptance, performance—in mind, we will look at how a RITE and an IIC differ. Recognizing the differences will help frame the discussion with the patient as to which style is most appropriate.
Appearance
The basic issue with appearance is whether the patient insists on an invisible device or if a discreet RITE will be satisfactory. There is more and more patient marketing these days that indicate the potential for an invisible fitting. This approach has driven more potential users to offices than ever before.
IIC candidacy issues. The complication is that not every patient who seeks an invisible device can be fit with IICs. First, the ear canals have to be large enough and with the right geometry to fit devices that sit beyond the second bend of the ear canal. Second, the patient has to be able to tolerate having something sit that deep in the ear. Finally, they must have the manual dexterity to get the devices in and out of the ears. We believe that the Intigai IIC can fit in approximately 1/3 of the ears in the general population, which we believe is consistent with the market in general.
Patient goals. This fit rate means that many patients who are looking for a true invisible solution will not be able to be accommodated. The options then become either a custom product (CIC) that may not be truly invisible or a small RITE product that can accurately be referred to as “discreet.” For some patients, the lack of invisibility may be a deal breaker. However, for many, the discreetness that the newer generation of RITE products such as Intiga RITE offers may be satisfactory. Clearly, a key part of the discussion with the patient is whether invisibility is a must-have feature. If the patient is willing to consider a discreet RITE solution, then virtually all ears can be fit.
Acceptance As indicated above, we believe that the initial exposure to amplified sound must be positive for the first-time user. There are a variety of signal processing approaches that are employed in an advanced product to make the first experiences listening through hearing aids acceptable.
Adaptation management. One of the most important trends over the past decade in the marketplace has been the introduction and now widespread use of adaptation management.3 This approach has allowed the first-time user, who likely has developed hearing loss over a number of years, to be provided with a gradual introduction to amplified sound. In addition, broader bandwidth and lower noise circuitry, especially nonlinear processing with a specific focus on reducing the sound quality problems of compressed signals,4 allow for advanced-technology hearing aids to sound more natural than ever before. These advancements, available in both RITE and IIC products, help to reduce the difficulty faced by first-time users when moving into the world of amplified sound.
Occlusion. However, probably the biggest concern is that a deeply seated product may cause occlusion issues for the first-time user. Although occlusion can occur with RITE products when fit to a closed coupling option, the risk is greater with small custom products where there is little or no ability to increase the vent size. In fact, occlusion is probably one of the biggest reason why many hearing care professionals moved away from CICs and other smaller custom products once RITEs and other mini-BTEs became available. However, the likelihood of occlusion is significantly reduced with IICs than with most CICs and other smaller custom products with restricted venting.
It is important to start with a review of what causes occlusion. Patients will experience an unacceptable perceived loudness level in the lower frequencies of their own voice when a column of air is trapped between the tip of the device and the tympanic membrane and the custom device oscillates out of phase with the structures of the head during vocalizations.1 In essence, the low frequencies of the voice become trapped in the ear canal.
One approach to reduced perceived occlusion is to increase the effectiveness of the vent in bleeding off low frequency energy. Effective venting can be increased in two ways: increasing the surface area of the vent opening or decreasing the length. IICs have a much shorter total body length than CICs and other smaller custom products. Although it is difficult to increase vent diameter in many ears and still have the device sit inside the second bend, the short body (typically 15 mm or less) of IICs improves the ability of the vent to reduce trapped low frequency energy.
Deep/tight-seal option. An alternative approach to reducing occlusion is to deeply seat the hearing aid in the ear canal so that there is a tight seal with the bony portion of the ear canal. This can reduce perceived occlusion because the hearing aid now resonates in phase with the bones of the head.
Over the years, it has become clear that creating a bony seal creates discomfort issues on the part of the patient. However, if the device terminates within the bony portion—even though there is not a tight seal—occlusion can be significantly reduced.1 This is because the bony walls will not resonate in the reduced volume of air in the same way as the softer tissue further out in the canal.
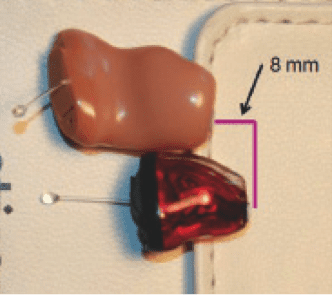
Figure 2 provides a photo of an IIC and a CIC, both made for the author’s right ear. They are placed in the photograph to replicate the relative depth when worn on the ear. Notice that the IIC sits approximately 8 mm closer to the tympanic membrane than the CIC, terminating within the bony portion.
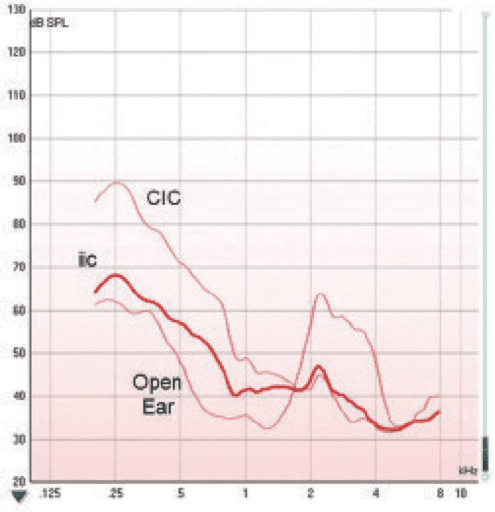
Figure 3 provides the results of an objective occlusion test performed by the author. The lower thin line provides the spectrum of the vocalized vowel “ee” (produced at a steady 65 dB SPL 18 inches from the lips). The upper thin line is the results for an “ee” vocalization with the CIC in place but turned off. The thick line provides the results with the IIC. As can be seen, for the CIC, the primary spectral peak in the low frequencies (approximately 250 Hz) is enhanced by nearly 30 dB by the presence of the CIC. However, the enhancement with the IIC is only about 6 dB.
Performance
Assuming that the patient has become comfortable with the appearance of the new devices and has successfully managed the first days of the introduction to amplified sound, eventually the discussion will return to performance. Again, the patient most likely took action due to perceived listening difficulties, and finding relief from those struggles will become the focus of the fitting before long.
The difference in style between the Intiga RITE and IIC leads to some significant differences in technology. These differences may well have audiological implications.
The two major technologies not available in the IIC (nor with any other IICs in the marketplace) are directionality and wireless connectivity. Although this loss of functionality has some audiological implications, there are also some advantages to the size and placement of the IICs.
However, the deeply seated faceplate does offer two specific advantages. First, the user has access to certain pinna-related localization cues that are lost in RITEs and BTEs with microphone placement over the ear. In the natural, open ear, there are slight spectral differences between sound arriving directly and sound that is reflected off of the convoluted structures of the pinna. These are high frequency cues that can be used for some precise localization tasks.5 Second, the pinna, due to the fact that it protrudes from the side of the head behind the entrance to the ear canal, gives the listener a naturally improved sensitivity to sounds coming from the front versus the back.
Although this effect is built back into many over-the-ear hearing aids by some manufacturers (we call our implementation Front Focus6), it is always better to allow for natural perception compared to artificial reproduction if at all possible. In the author’s opinion, the benefits of the deeply seated microphone in an IIC probably do not make up for the lost benefits of directionality. However, if the patient chooses an IIC style for other reasons, it is somewhat comforting to know that there are some audiological compensations.
Wireless-related considerations. The small size of IICs prohibits the inclusion of wireless receivers and transmitters at this point in time. As wireless technologies continue to become smaller, it is conceivable that on-board wireless may be a reality in true IIC products at some point in the future.
In the Intiga family, the loss of wireless includes both the loss of binaural processing and the loss of connectivity to other electronic devices. This means that the RITE offers added features, such as the Spatial Sound compression approach, Binaural Synchronization of automatic features, and binaural user conveniences along with full connectivity to externally generated transmitted sound sources.
For a patient who is gravitating toward an IIC for purely cosmetic reasons, this restriction in function may cause some reconsideration.
Final Thoughts
The hearing aid style decision for a first-time user ultimately belongs to the user. The professional may have strong opinions one way or the other concerning IICs and RITEs, but the patient deserves an objective description of the similarities and differences between the styles.
In many cases, the patient may have an “invisible or nothing” attitude, at least entering the hearing aid consulting process. If the professional believes that, for practical and/or audiological reasons, the RITE style is a better option than the IIC, then that case should be made to the patient. Other professionals have already embraced IICs and other invisible options as they are helping to break down a major barrier of reluctance. Either way, the material in this paper should help lay out the issues in a way that can assist in the patient counseling process.
Donald J. Schum, PhD, is vice president of audiology and professional relations at Oticon Inc, Somerset, NJ. CORRESPONDENCE can be addressed to Dr Schum at: [email protected].
References
1. Dillon H. Hearing Aids. Turramurra, Australia: Boomerang Press; 2012.
2. Behrens T, Kreisman B, Schulte M, Weile J. Meeting the first-time user challenge. Hearing Review. 2011;18(13):18-29. Available at: /practice-management/17185-meeting-the-first-time-user-challenge
3. Schum D. Adaptation management for amplification. Seminars in Hearing. 2001;22(2):173-182.
4. Schum D, Sockalingham R. A new approach to nonlinear signal processing. Hearing Review. 2010;17(7):24-32.
5. Bear M, Connors B, Paradiso M. Neuroscience: Exploring the Brain. Baltimore, Md: Lippincott, Williams & Wilkins; 2001.
6. Schum D. Redefining the hearing aid as the user’s Interface with the world. Hear Jour. 2007;60(5):28-33.