
This study looks at several factors related to first-time use of hearing aids with the new Oticon Intiga device, which employs a system of gradual gain increases during the first month of use until it reaches full prescriptive gain. Some benefits derived from the use of help systems—such as directional microphones—are realized almost immediately and grow as the hearing aid increases the amplification. Other help systems provide some significant immediate benefit, and then appear to grow in terms of improved aided performance over time, as the auditory system experiences increased audibility of, and learns to use, speech and spatial cues that facilitate speech understanding in complex sound environments.
When first-time users (FTUs) initially visit a hearing care practice, most have already journeyed through a long process that ultimately led to the decision that they probably need amplification. This process is likely to include:
- Attracting unwanted attention to oneself due to misunderstandings and miscommunications;
- Becoming suspicious that this is due to a hearing loss;
- Acknowledging that there is a problem;
- Contemplating and realizing the consequences (and perhaps even self-examination); before
- Admitting/understanding that there is a hearing problem, and hearing aids may be the solution.1




Thomas Behrens, MScEE, is manager of clinical evidence and communications at Oticon A/S, Smoerum, Denmark; Brian Kreisman, PhD, is director of the Center for Amplification, Rehabilitation, and Listening (CARL) and an associate professor at Towson University, Towson, Md; Michael Schulte, PhD, is a research audiologist at Hörzentrum Oldenburg, Oldenburg, Germany; and Julie Neel Weile, MA, is a clinical audiologist at Oticon A/S.
This recognition process is troublesome for a large proportion of FTUs, but it also provides a good background to explain to them the potential benefits of hearing rehabilitation. If, for example, they are aware of their loss of social interaction due to untreated hearing loss, then they are also more likely to seek out hearing aids that may benefit them in social situations.
Hence, when they finally decide to do something about their hearing loss, we should be able to provide a solution that benefits them in key listening situations, allows them to adjust to amplified sound, and is so discreet that it does not attract attention.
This article presents findings of a study about the potential benefits of a new hearing solution for FTUs, Oticon Intiga. The study investigates the immediate benefits and acceptance of the devices, both in the field and in the laboratory. These are compared to benefits obtained over the first month of use, when an Automatic Adaptation Manager ensures the transition from an initial first-fit gain prescription to a fully prescribed gain setting. For a full report on the findings of this study, please refer to the companion paper by Nagle et al (manuscript in preparation).
Benefits of Hearing Aids to First–Time Users
Interestingly, when looking through the literature, very little evidence exists to describe the immediate benefits and acceptance of hearing aids during the first week of use. The traditional paradigm is that it takes time to acclimatize to hearing aids and experience many of the benefits (eg, “You’ll get used to it”). However, this paradigm has led to protocols that have generally ignored benefit and acclimitization during the first week of hearing aid use.
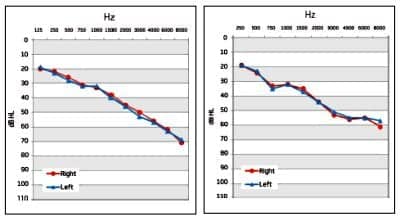
Figure 1. Average audiometric data from Oldenburg in the left panel and from Towson in the right panel.
Studies on speech understanding benefits of hearing aids are typically conducted using an input level of about 65 dBSPL with hearing aids in an omnidirectional mode. While this may be a valid observation for a very specific acoustic condition, modern hearing aids typically include automatic functions that enable and disable help systems, such as directionality and noise reduction, depending on the particular acoustic environment. These automatic changes are based on specific acoustic criteria programmed into the acoustic scene analysis systems that drive the “decision-making” processes of a hearing aid. Therefore, it seems reasonable to evaluate potential benefits of hearing aids at different levels in different masking conditions.
Valente and Mispagel2 reported no benefit of an open-fit hearing aid in an omnidirectional mode, and 1.9 dB benefit of the same device in a directional mode. These results were obtained by first-time users after 4 weeks of hearing aid use, with the speech presented in a demanding competition from a surrounding restaurant noise presented at 65 dBSPL. A similar benefit of about 1.8 dB was found by Kuk and Keenan3 using the HINT in competing noise presented at 75 dBSPL.
In a study by Hällgren et al,4 a relatively small hearing aid benefit, in this case about 0.4 dB, was found in steady-state speech-shaped noise presented at 75 dBSPL. However, when they used a speech masker, benefit increased to about 2.5 dB. Thus, when there are temporal fluctuations in the masker, the benefits of aided listening in noise seem better materialized because level fluctuations allow for listening of speech cues in the weaker masker intervals.
Study Method to Assess Immediate Benefit and Acceptance
To assess immediate benefit and acceptance, a protocol was designed that examined a number of laboratory and field measures over the first month of use. On days 0, 1, 3, 14/16, and 28/30 relative to the fitting day, the following measures were administered at the Hörzentrum in Oldenburg, Germany, and at Towson University in Towson, Md.
To investigate potential benefits and acceptance reflecting daily life use with the devices, two different acoustic conditions were created. One condition was created with the purpose of providing information about the amplification and compression system of the present hearing aid. A second condition was designed to investigate the benefits of one of the help systems, Split Directionality, that is enabled in situations with background noise at moderately high levels (described in more detail below).
Subjects. Inclusion criteria were symmetrical hearing loss (maximum 10 dB difference between ears) and no or negligible conductive components. As the study also sought to test the first month of use with a shorter adaptation period, an inherent minimum wear-time was needed for the user to become experienced with amplified sound and for the adaptation manager to reach the level of prescribed gain.
A total of 43 test persons with no prior hearing aid experience participated at the two test sites, with 22 at Towson and 21 at Oldenburg (total of 20 females, 23 males). One subject from Towson was unable to comply with the minimum wear-time demands of at least 6 hours per day; he was excluded from the study. Therefore, data from 42 participants were included in the data analysis, 21 from each site.
The mean age of the study population was 67.6 years (65 in Towson and 70 in Oldenburg), ranging from 20 to 85 years. The mean 4-frequency PTAs (average of threshold at 0.5, 1, 2, and 4 kHz) were 39 dBHL and 40 dBHL in the right and left ear, respectively. The average air conduction hearing thresholds (HTL) of subjects at the two study sites are shown in Figure 1.
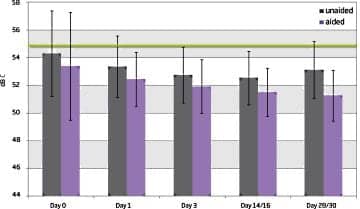
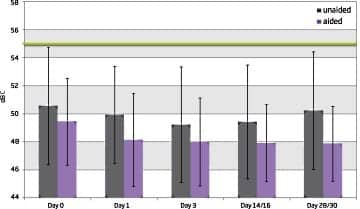
Figure 2. Average German OLSA (left) and US Matrix (right) test results from unaided and aided testing for the 5 test days. Also shown in green is the fixed level of the ISTS masker. Note that lower thresholds indicate better performance.
Hearing instrument. Oticon Intiga is a small open-fit, receiver-in-the-ear (RITE) style hearing instrument. It is equipped with the Speech Guard amplification and compression system, Spatial Sound 2.0, the proprietary Voice Aligned Compression rationale, and a number of help systems (eg, traditional noise reduction, split and full directionality).
Additionally, it has been optimized for first-time users and thus comes with a new first-fit gain prescription and new, faster automatic adaptation manager. In addition, the designs of both hearing instrument and speaker unit have been optimized to ensure greater headroom and better retention.
Materials and procedures. The test protocol encompassed lab tests, as well as daily life tests, that were repeated through the first month of hearing instrument use; at the day of fitting (Day 0), the first day of use (Day 1), the third (Day 3), at approximately 2 weeks (Day 14-16), and after 1 month (Day 28-30). Different specified days 14/16 and 28/30 were allowed for the two last visits at the two sites, as this significantly facilitated the practical execution of testing at each site and was considered insignificant to the results.
The laboratory tests used were the Hearing in Noise Test (HINT)5,6 in the United States, and in Germany the Göttinger Sentence Test (GOESA),7 the Matrix test (available in both German8 and US English), and a measure of listening effort based on the use of the Matrix sentences. A preliminary validation study of the US Matrix is currently being conducted at Towson University, with a larger, multi-site study being planned.8,9
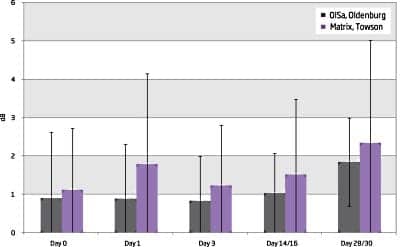
Figure 3. Hearing aid benefit (aided – unaided threshold), as a function of test day and test site of the OLSA and Matrix tests.
The Matrix test was used to test the benefit of amplification in a situation with soft speech in a background of ISTS maskers. The uncorrelated ISTS signals10 were presented from speakers at ±45° and ±135° at 55 dBC with the adaptive speech coming from the front (0° azimuth) with a start level also at 55 dBC. The hearing instruments were set in fixed omnidirectional microphone mode.
The HINT was used to test speech-in-noise benefit of the hearing aid in split directional mode. Standard uncorrelated continuous noise from ±90° and ±135° at 70 dBC was used, with speech presented adaptively from the front at 0° azimuth. The hearing aid was fixed in split directional microphone mode (high frequency directional).
For both speech tests, loudspeakers were placed at a distance of 0.8 m and 1.5 m from the center of the head of the subjects in Towson and Oldenburg, respectively.
To minimize training effects in the data, each test was administered beginning with a short training session, followed by either the aided or unaided condition. The conditions and order of tests were balanced and randomized between the participants.
For the listening effort test, the same speaker setup and hearing aid settings as in the Matrix test were used. The ISTS masker was set at 55 dBC from ±45° and ±135° azimuth, with speech coming from the front (0°) at levels of 49, 52, 55, 58, 61, and 64 dBC (from -6 to +9 dBSNR) in randomized order. A training session was followed by an aided and unaided condition; the latter two were randomized. During the test, the subject rated perceived listening effort on a 13-point scale, ranging from no effort to extreme effort as described by Luts et al.9
At each visit, the internally developed New User Questionnaire was administered to observe how the participants perceived the use of the hearing instrument. The questionnaire was filled out in person by the participants at every visit, making it possible to follow their perceptions over the course of the first month. It includes items relating to the physical comfort of the devices, listening comfort of loud sounds, speech in quiet and in noise, perception of own voice, and overall performance. In addition, it contains items relating to the process the first-time user is going through. These are questions on whether the users are happy with the decision to acquire hearing aids, how well they adjust to the aids, and whether they see themselves as long-term users. A 5-point scale with “1” indicating poor performance or dissatisfaction and “5” indicating good performance or great satisfaction is used in the questionnaire.
Study Results
Study participants were generally in compliance with the minimum use-time criteria. However, as mentioned, one subject was excluded due to low usage time. The average daily use-time logged by the hearing instruments was about 10.5 hours.
Data in absolute scores from speech intelligibility lab tests were analyzed using a repeated measures analysis of variance (RMANOVA) with study site coded as a between-subject factor. The factors investigated by the overall analysis were potential changes in speech reception thresholds over the first month of use and differences between unaided and aided conditions. Furthermore, a second analysis was conducted on the benefit (differences between unaided and aided scores) data from the two specific tests, Matrix/OLSA and HINT/GOESA, to examine the effects of site and the change in benefit over the first month. Data from the listening effort test were processed similarly, investigating the effects of site, changes in scores over time, and differences between aided and unaided conditions. The significant main effects and interactions from these analyses are reported.
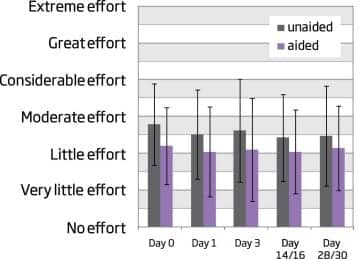
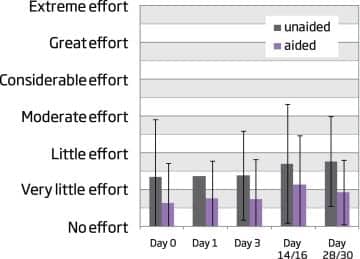
Figure 4. Mean ratings of listening effort with +3 dBSNR, when listening for Matrix sentences in an ISTS masker (speech at 58 dBC and masker at 55 dBC). Ratings are given for each site individually, Oldenburg to the left and Towson to the right, and related to the scale used.
Speech reception. Figure 2 shows the unaided and aided speech reception thresholds from the Matrix test, presenting the data as they were obtained in the laboratory setup, with thresholds given in absolute numbers and related to the fixed noise level used. The outcome of the RMANOVA showed significant effects of test site, significant differences in thresholds over time, and significant differences between unaided and aided thresholds (all significant at p<0.001). The site effect relates to thresholds obtained at Towson being systematically lower (better SRTs) than those obtained in Oldenburg; however, there were no interactions with site, which indicates that developments over the first month of use (as well as differences between aided and unaided) did not differ significantly between sites.
Threshold changes. Significant changes in thresholds over time can be seen in Figure 2, and appear to indicate a lowering of aided thresholds. Analyses (Post-Hoc, Tukey HSD, p<0.001) verified that aided performance was better than unaided performance on all test days, and that aided performance on Days 1 through 28/30 was significantly better than on Day 0.
Average benefit of hearing aids at both sites for the Matrix and OLSA tests is shown in Figure 3. Averaging across sites, benefit was about:
- 1 dB on Day 0,
- 1.3 dB on Day 1,
- 1.1 dB on Day 3,
- 1.3 dB on Day 14, and
- 2 dB on Day 28.
The RMANOVA analysis revealed a significant effect of day (p<0.01), but no effect of site (p>0.05). Further analyses (Post-Hoc, Tukey HSD) showed significant changes from Days 0 to 28 (p<0.01), Days 3 to 28 (p<0.01), and Days 14 to 28 (p<0.05). Thus, the data demonstrate that there is a hearing aid benefit already on Day 0, and that this benefit increases over the first month of use.
The results of the HINT and GOESA testing also showed aided benefit, again with a difference between sites, which did not interact with benefit. In addition, aided thresholds continued to decrease during the entire period, indicating a significantly improved performance with split high frequency directionality as gain increases in the devices.
Table 1. Mean ratings of the 9 items in the New User Questionnaire for all test days along with the corresponding standard deviations in parentheses. Note that no data are available for items 4, 6, and 8, at Day 0 as the subjects did not have the experience to make such judgment.
Listening effort. Ratings of listening effort in the modulating speech-like ISTS masker were obtained for a great range of signal-to-noise ratios. The manuscript by Nagle et al covers this in more detail; in this article, we limit our focus only to one of these: using a speech level of 58 dBC. In effect, this produces a situation with a positive SNR (recall that the masker level was set to 55 dBC), compared to the negative SNRs where most of the speech intelligibility testing took place. Results at this SNR are shown in Figure 4 for each test day.
Figure 4 suggests that there are lower mean ratings for aided listening than for unaided listening at every day tested, and the overall magnitude of the hearing aid benefit is roughly constant over time, being about a scale point. Ratings from Towson are generally lower than ratings from Oldenburg, and the hearing aid benefit appears to be larger at Towson than at Oldenburg. These results were verified by the analysis, which showed significant effects of aided relative to unaided and of test site (RMANOVA, p<0.001).
Comments on site effects. The site effects seen on the aided and unaided thresholds, as well as on the corresponding effort ratings, are likely due to a number of factors differing between test sites. It is well known that differences in speech reception threshold exist between implementations of the same test in different languages.9,11 Also, the difference in distance between the subject and the loudspeakers at the two sites may have contributed to some differences in the perceived acoustic mixtures.
Questionnaire results. Mean questionnaire ratings of the nine items of the New User Questionnaire for all test days are shown in Table 1, along with the corresponding standard deviations (in parentheses). In general, the data indicate relatively stable self-ratings across the test period. All ratings start above 3 and remain high during the entire study, indicating mean rating levels from acceptable to good. Item 1 relating to physical comfort in the ear does show a tendency to improve during the period, and indeed the mean rating on Day 28 of 4.2 is significantly greater than the mean ratings for Days 0, 1, and 3 (p<0.01 on Days 0 and 3, and p<0.05 on Day 1, Wilcoxon Matched Pairs).
Item 7 regarding the perception of own voice improves significantly from Day 0 to Days 14 and 28 (p<0.05, Wilcoxon Matched Pairs). Laugesen et al12 reported similar results when examining FTU perception of own voice; they found that both first-time users and experienced users perceive changes in the sound of their own voice, but generally users accept this change as being unavoidable and, with time, not worth mentioning.
Relating mean ratings to the labeling used in the questionnaire, the average rating on physical comfort is slightly better than “comfortable.” Similarly, loud sounds are rated as slightly better than “somewhat comfortable.” That loud sounds are given this rating is an expected finding, given that all users ended up in a full prescribed setting— which is not the case in a large clinical population, where the final gain setting would typically be less than full prescribed after 1 month. Still, this finding suggests that a full prescribed setting can be used as the default at the end of the adaptation period.
For the item concerning speech understanding in quiet, the mean rating corresponds to “easy” to understand; in noise, it is “somewhat easy.” Perception of own voice is typically rated between “somewhat natural” and “natural,” and overall performance is typically rated “above average.”
The items that relate to the process the user undergoes typically indicate that the user is “happy” with the decision to get hearing aids, that adjustment to the aids has been “easy,” and that they “more than likely” see themselves as long-term users.
Conclusion
Results from this study have shown that there are immediate benefits of the Oticon Intiga hearing aids used, which materialize on the first day of use. Some benefits deriving from the use of help systems, such as directional microphones, are realized in large part immediately and grow as the hearing aid increases the amplification. Others give some significant immediate benefit, and then appear to grow (in terms of improved aided performance) over time, as the auditory system experiences increased audibility of, and learns to use, speech and spatial cues that facilitate speech understanding in complex sound environments.
The small open-fit RITE style hearing aid used in this study also seems to provide immediate acceptance of the physical fit, loudness, and speech understanding, as shown in questionnaire ratings. Also, self-ratings show the users adapted well from the first-time user prescription (adaptation Step 1) to the experienced user prescription (adaptation Step 3). The ratings further suggest that Oticon Intiga provides the overall performance that is necessary for a first-time hearing aid user to become an experienced long-term user.
Acknowledgements
The authors would like to thank our colleagues from Towson University: Stephanie Nagle, Jennifer Smart, Candace Robinson, Caitlin Marczewski, and Cortney Butler; and from Oldenburg: Kirsten Wagener, Kevin Pollak, and Anja Schröck; and from Oticon: Don Schum, Anja Ravn Madsen, Maria Grube Jakobsen, and Sebastian Oakley.
References
- Engelund G. Time for Hearing—Recognising Process for the Individual. A Grounded Theory [PhD thesis]. University of Copenhagen & Oticon Research Centre, Eriksholm, Denmark, Department of Nordic Studies and Linguistic Audiologopedics; 2006.
- Valente M, Mispagel KM. Unaided and aided performance with a directional open-fit hearing aid. Int J Audiol. 2008;47:329-336.
- Kuk F, Keenan D, Ludvigsen C. Efficacy of an open-fitting hearing aid. Hearing Review. 2005;12(2):26-30.
- Hällgren M, Larsby B, Lyxell B, Arlinger S. Speech understanding in quiet and in noise, with and without hearing aids. Int J Audiol. 2005;44:574-583.
- Nilsson M, Soli S, Sullivan J. Development of the hearing in noise test for the measurement of speech reception thresholds in quiet and in noise. J Acoust Soc Am. 1994;95:1085-1099.
- Operating Instructions HINT Audio CD 2.0. Eden Prairie, Minn: Maico Diagnostics; 2004.
- Kollmeier B, Wesselkamp M. Development and evaluation of a German sentence test for objective and subjective speech intelligibility assessment. J Acoust Soc Am. 1997; 102:2412-2421.
- Wagener KC, Brand T. Sentence intelligibility in noise for listeners with normal hearing and hearing impairment: influence of measurement procedure and masking parameters. Int J Audiol. 2005;44:144-156.
- Luts H, Eneman K, Wouters J, et al. Multicenter evaluation of signal enhancement algorithms for hearing aids. J Acoust Soc Am. 2010;127:1491-1505.
- Holube I, Fredelake S, Vlaming M, Kollmeier B. Development and analysis of an International Speech Test Signal (ISTS). Int J Audiol. 2010;49:891-903.
- Soli SD, Wong LL. Assessment of speech intelligibility in noise with the Hearing in Noise Test. Int J Audiol. 2008;47:356-361.
- Laugesen S, Vestergaard H, Nielsen C. Common conceptions about first-time versus experienced hearing aid users: facts or fiction? In: Rasmussen A, Poulsen T, Andersen T, Larsen CB, eds. Hearing Aid Fitting. 21st Danavox Symposium. 2005:261-287.
Citation for this article:
Behrens T, Kreisman B, Schilte M, Weile J. Meeting the First-Time User Challenge. Hearing Review. 2011;18(13):18-29.



 Hearing Exams with Hearing Aid Benefits" data-lazy-src="https://hearingreview.com/wp-content/uploads/2019/10/dreamstime_m_102029139-440x264.jpg"/>
Hearing Exams with Hearing Aid Benefits" data-lazy-src="https://hearingreview.com/wp-content/uploads/2019/10/dreamstime_m_102029139-440x264.jpg"/>