
Patient Care | November 2018 Hearing Review
A new holistic tool for performance hearing needs assessments
Hearing loss is a shared disability. Studies have shown both client and family preference for—and better outcomes when—involving family members in the hearing rehabilitation process.1,2 Research has also demonstrated a positive link between hearing instrument satisfaction and the number of listening situations in which these deliver benefit.3
The FOCAS tool is designed to:
1) Actively seek input from both the client and family during the hearing needs and goal setting process;
2) Assess whether these are near- or far-field situations, and
3) Help to determine the optimal solutions for each.
This paper describes the survey results, rationale for, and how to use the FOCAS tool.
We surveyed 76 hearing healthcare professionals (HCPs) from around the world, and only 25% reported a family member being present either often or almost always in an appointment. And in terms of delivering hearing satisfaction, only approximately 42% of HCPs regularly (ie, either mostly or always) explore whether their client’s needs may include hearing sounds originating in the far-field. Use of a formal communication assessment tool was also variable.
Accordingly, we developed the Family Oriented Communication Assessment and Solutions (FOCAS) tool, which:
- Actively seeks input from both the client and family during the hearing needs and goals setting process;
- Assesses whether these needs/goals are near- or far-field situations, and
- Helps to determine the optimal solutions for each.
This article describes the survey results, rationale for, and the development of, the FOCAS tool.
Family Centered Care
Adult audiologic care is generally provided along a continuum, from a site-of-lesion approach to a patient-centered care perspective.4 While the former considers the anatomical, physiological, and functional aspects of hearing loss, it has been recognized for some time that this approach inadequately addresses the cognitive, emotional, motivational, and social aspects of hearing loss. And this realization is not unique to audiologic care. Over the last decade or so, there has been a significant shift from a medical to more “patient-centric” and “value-based” models in patient care.5 The patient-doctor relationship is very firmly shifting to a place where the patient is acknowledged to be an active participant in the clinical process and choice of treatment.
Family-Centred Care (FCC) is an extension of person-centered care, and places greater emphasis on the role of the family. According to the Institute of Medicine:
“FCC provides care to patients and family members that is respectful of and responsive to individual patient and family preferences, needs, and values, and ensures that patient and family values guide all clinical decisions.”6
In this context, a family member includes anyone who is related by way of a continuing biological, legal, or emotional relationship. Research indicates both patients and their families report a clear preference for greater involvement during the audiologic process.1,2
Moreover, there is a broad consensus in the literature from wider medical research that FCC results in better health outcomes, well-being, adherence to treatment plans, and satisfaction with services (see Rathert et al7 for a review). In addition, family members report increased awareness of the impact of hearing loss on the patient,8 reduced third party disability,9 and improved relationship quality and quality of life (QoL) with a FCC approach.10 As such, FCC is seen as the most appropriate approach for audiologic care, as communication issues also impact family members.
In terms of benefits for the clinician, research suggests the shared decision-making process encouraged by a family-centered approach improves patient provider relationships and increases trust.11 When trust is high, 90% of clients proceeded with the clinician’s recommendation compared to only 50% when trust was considered to be low between the client and the provider.12
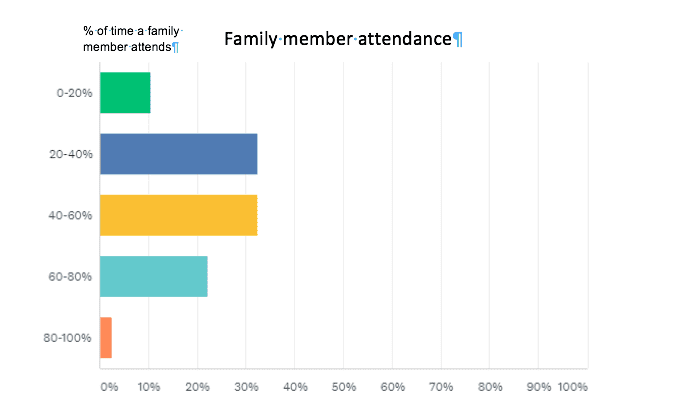
[Click on images to enlarge.] Figure 1. Percentage of appointments attended by a family member.
So, Why Is Family Involvement So Low?
One reason may be due to the challenges faced when trying to implement a new approach in everyday clinical practice. Phonak has published a number of papers through its Family-Centred Expert Circle to address some of the issues that can be seen as barriers to implementation (eg, see the Counseling Tools website13), however some clinicians may actually be uncomfortable delving into what can be emotional family dynamics associated with hearing loss. Others may have concerns around the time efficiency of including others. And some may stumble on the very first barrier—getting a family member to attend in the first place.
Turnbull14 discusses that at the heart of any attempt to a change in practice, is the need for a clear change management strategy that includes key stakeholders, training, identification of possible barriers, engagement of positive drivers, and ongoing support. One of the barriers to implementing a new approach is the communication assessment and the tools commonly used to record goals, which are critical components of best practice in audiological rehabilitation.
Communication Assessment and Goal Setting
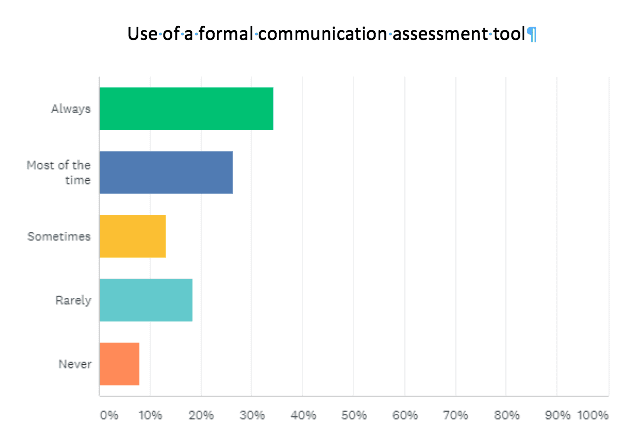
Figure 2. Reported use of a formal communication assessment tool.
A plethora of structured, formal tools have been developed to support communication needs assessments (eg, the Hearing Handicap Inventory for Adults/Elderly (HHI-A/E),15 Abbreviated Profile for Hearing Aid Benefit (APHAB),16 etc), and these have contributed greatly to establishing the needs and goals of the client and in measuring outcomes and benefit. A review of all of these tools is beyond the scope of this paper. However, the results of our survey (Figures 2 and 3) found that for those who used a formal tool most of the time or always (60%), the most commonly used (79%) was the Client Oriented Scale of Improvement (COSI).17

Figure 3. The formal communication assessment tools used by those who use them (see Figure 2).
The popularity of COSI may be due to its ease of administration (very concise and quick), high validity for measuring benefit and satisfaction with hearing aids, and involvement of the client in self-rating.17 Indeed, respondents to our survey really liked the ease of use and utility for identifying goals and tracking benefit.
However, the COSI does not actively seek input from family during the communication assessment and goal setting, which, as discussed, has been shown to lead to better client outcomes. Interestingly, this was pointed out by a couple of survey respondents as an area for improvement to currently available tools, with one commenting the tool they use “could be updated to include family centred care.” Others indicated current tools aren’t “holistic enough” and could provide “differentiation in technology levels.” Availability in different languages was also requested. These insights from our survey were all factored into the development of the FOCAS tool.
When using COSI, areas of need/goals are only ranked in order of significance, rather than exploring the emotional payoff for each and the overall impact they have on QoL. Exploring the emotive/QoL impacts of hearing loss are likely to improve motivation, leading to improved uptake and regular use of hearing technology.18
Finally, the self-reported degree of change and final hearing ability with COSI is rated with hearing aid(s) alone, rather than considering both near- and far-field hearing needs and presenting a holistic hearing solution right up front. Exploring both near- and far-field needs is critical given adoption of hearing solutions is greatly influenced by the number of situations in which the recommended solution delivers better hearing.3
Establishing Hearing Needs in Both the Near- and Far-field

Figure 4. Schematic illustrating the concept of near- and far-field hearing, and which technologies deliver optimal performance as a function of this and background noise.

Figure 5. Signal to noise ratio (SNR) diminishes over distance from sound source.
Hearing well requires us to detect sounds both close and far away from us. This is known as near- and far-field hearing, respectively. The near field is typically around 1.5 m from the listener and hearing aids work very well within this range, even when there is background noise by using directional microphone and signal processing technology (Figure 4).19-23 However, as shown in Figure 5, the effectiveness of hearing instruments alone starts to diminish as the sound source of interest moves into the far field. This is because sound decreases 6 dB per doubling of distance from its source, and becomes compromised by external environmental factors such as reverberant and competing sound before it reaches the hearing aid microphones. By placing the microphone closer to the source, wireless communication solutions help extend hearing aid benefit in these situations, and when noise is also present, assistive listening systems like Roger deliver unparalleled performance.24,25
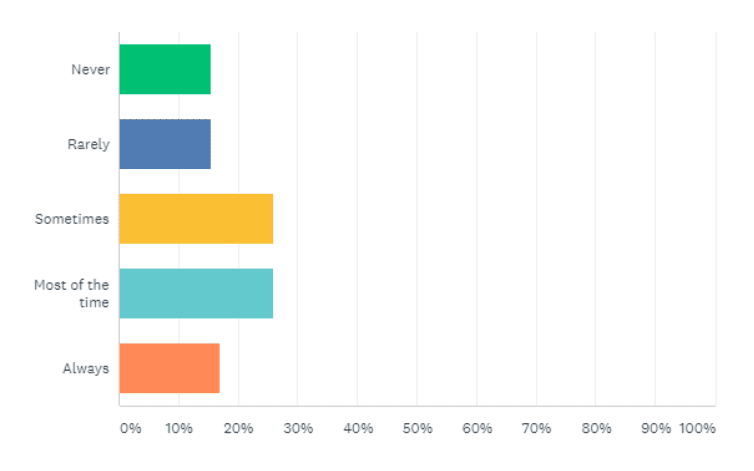
Figure 6. Survey result showing the regularity that HCPs explicitly explore needs in the near- and far-field.
While it is standard practice for far-field hearing needs (eg, a classroom) to be considered for pediatric clients, we suspected this may be less common in an adult rehabilitative setting. Our survey results confirmed this, showing that only about 42% of HCPs regularly (ie, either mostly or always) explore whether their client’s needs are for sounds originating in the far-field (Figure 6). Tellingly, about 25% of HCPs who undertook the survey didn’t even answer this question! For those HCPs who do explore the dimension of distance, our survey results show that about 40% said over half their clients have far-field hearing needs. This surprised us, and suggests that when far-field needs are not explicitly explored, a substantial number of clients may not have all their needs fully met by their hearing solution!
When we asked HCPs who don’t distinguish between near- and far-field hearing needs, 37% either had not considered it or were unaware of the value of exploring this, with one HCP saying they mostly fitted premium hearing aids, therefore negating the need for technology that overcomes distance. Another respondent tended to “…ask at follow-ups,” and another mentioned the lack of a “formal measure in place.”
Given these responses, it is evident that understanding of the acoustic limitations of hearing aids and accessories that overcome distance are not well understood by some HCPs. It is reasonable to assume that some clients (and HCPs) may therefore overestimate the efficacy of hearing aids in certain situations, and may therefore have poorer outcomes or attitude towards hearing aids and their performance over distance, in reverberant, or in very noisy situations.
Given the need for more education on the limits of hearing aid performance, the benefits of involving family and the emotive impacts of hearing loss, as well as considering all hearing needs (both near- and far-field), this led us to develop a resource that folds all these important dimensions into one tool: FOCAS (Figure 7).
Development of the FOCAS
Our goal was to develop a single, clinical tool that:
- Integrates family centered care (FCC) so that clients and their families develop shared goals, are fully informed of the various rehabilitation options available and are central in deciding which is best for them;
- Explores the emotive impact of hearing loss, and
- Considers holistic hearing needs, including both near- and fair-field situations. Because language was noted by several survey respondents as an area for improvement, an additional goal was to translate FOCAS into several languages to promote hearing needs assessments within the hearing profession globally.
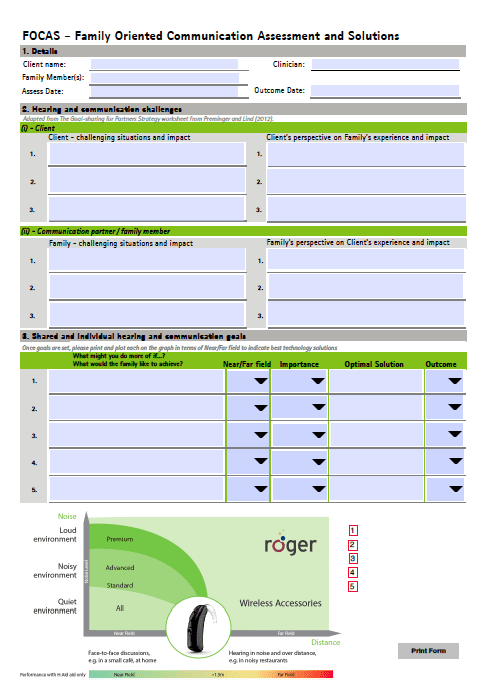
Figure 7. The FOCAS tool showing the 3 main sections that fold in aspects of FCC, shared communication goal setting and measurement as well as explicit consideration of both the near- and far-field.
Click here to see the full-page version of the Interactive FOCAS form
Family centered approach and exploring the emotional impact of hearing loss. The FOCAS tool was developed to address efficiency and efficacy of family involvement while also retaining the goal-oriented and benefit measurement aspects of other tools. There is a move away from very specific goals which, while they can be measured very effectively, can be limiting in what is addressed as “difficult hearing situations.” Rather, more general goals may be discussed in terms of what the client would like to achieve—which are more real for the client. This question is also asked of the family as a unit to establish shared goals that encourage a team approach to addressing communication needs.
The structured flow, which includes elements adapted from a worksheet developed by Preminger and Lind,26 allows time for the client, with a response from family members; and alternatively, where family members are asked to share their perspective to allow the client to gain insight into the impact of their hearing loss on others.
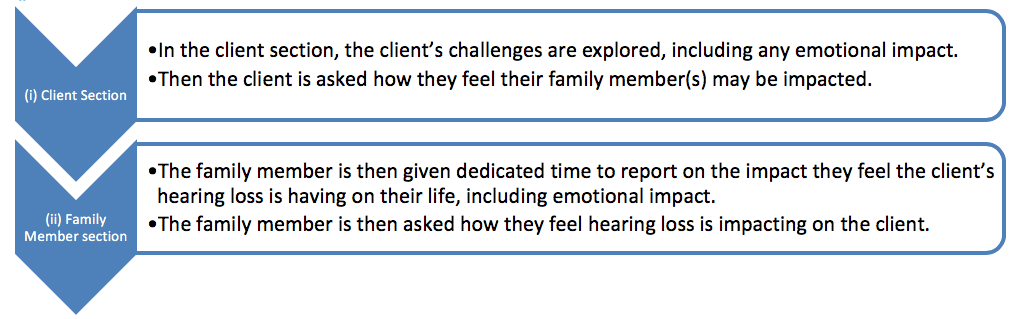
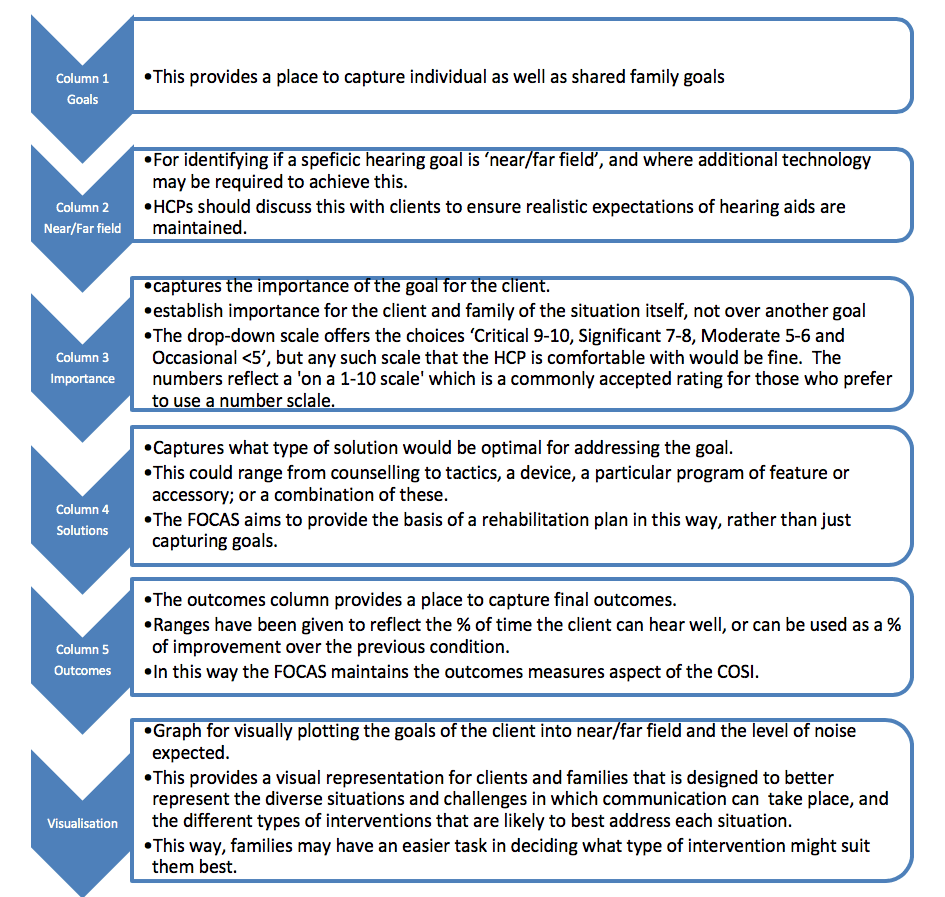
Table 1. Process flow for how you complete the two key sections within the FOCAS tool.
This structure encourages a discussion if different perspectives result in highlighting incongruencies between family members and seeks to then establish shared goals.27 Rather than establishing goals in order of importance, goals are rated on the importance they play in the client’s and their family’s life, as two quite different goals may have similar importance. This also helps clients to express and gain self-awareness in their own terms about the impact certain situations have on their quality of life.
By exploring potential motivational differences and finding common ground to address them, isolation caused by a lack of understanding or unwillingness to accept hearing loss can be addressed more readily, and the increased benefit when family members share responsibility for health outcomes can be realized more readily.
Near- and far-field needs. When establishing the communication and hearing challenges as well as subsequent goal setting, the FOCAS tool encourages all needs to be considered in terms of the noise present and proximity. From this, the various technologies and strategies required to optimally meet each goal can be discussed and a potential rehabilitation plan developed. If a client is unable to pursue all recommendations, then this can also be the basis of establishing realistic expectations for some goals where the optimal solution has not been possible.
How to Use FOCAS
The process for using the FOCAS tool is detailed in Table 1. As one can see, the flow indicates how you complete the two separate key sections within the FOCAS tool.
Summary
With the concept of FCC becoming more relevant for HCPs, several barriers have been identified that can make implementation more difficult. One barrier identified is the absence of a communication needs assessment tool which takes into account family input and the setting of shared goals. A survey of 76 hearing care professionals from several countries also identified that in many cases near- and far-field requirements for effective communication were not considered regularly, and identified that some HCPs are not be aware of the limitations of hearing aids over distance. The survey further identified that no tool at all was being used in some countries due to lack of access to tools in the local language.
The FOCAS tool was developed to address these issues and is currently being trialed in Australia and New Zealand for ease of use and efficacy in its aims. At the time of writing, the FOCAS has been translated into 21 languages. The outcomes of the trial will be used to further refine the tool, and a validation study is underway which will be reported on in future publications.
Correction
An earlier version of this article, as well as the print edition, incorrectly referenced work by English & Kasewurm. The paragraph that contains references #11 (Preminger et al, 2015) and #12 (Thom et al, 2002) have replaced this error.
References
-
Poost-Faroosh L, Jennings MB, Cheesman MF. Comparisons of client and clinician views of the importance of factors in client-clinician interaction in hearing aid purchase decisions. J Am Acad Audiol. 2015;26(3):247-259.
-
Meyer C, Scarinci N, Ryan B, Hickson L. “There is a partnership between all of us:” Audiologists’ perceptions of family member involvement in hearing rehabilitation. Am J Audiol. 2015;24:536-548.
-
Kochkin S. Increasing hearing aid adoption through multiple environmental listening utility. The Hearing Journal. 2007;60(11):28-31.
-
Singh G, Hickson L, English K, et al. Family-centered adult audiologic care: A Phonak position statement. Hearing Review. 2016;23(4):16.
-
Special Report: Hearing care and “value-based reimbursement” in medicine. Hearing Review. 2018;25(3)[Suppl]:2-7.
-
Committee on Quality of Health Care in America and Institute of Medicine. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press; 2001.
-
Rathert C, Williams ES, McCaughey D, Ishqaidef G. Patient perceptions of patient-centred care: Empirical test of a theoretical model. Health Expect. 2012;18(2):199-209.
-
Hallberg LR-M, Barrenäs M-L. Group rehabilitation of middle-aged males with noise-induced hearing loss and their spouses: Evaluation of short- and long-term effects. Brit J Audiol. 1994;28(2):71-79
-
Habanec OL, Kelly-Campbell RJ. Outcomes of group audiological rehabilitation for unaided adults with hearing impairment and their significant others. Am J Audiol. 2015;24:40-52.
-
The National Council on Aging—Seniors Research Group. The consequences of untreated hearing loss in older persons. https://www.ncoa.org/wp-content/uploads/NCOA-Study-1999.pdf. May 1999.
-
Preminger JE, Oxenbøll M, Barnett MB, Jensen LD, Laplante-Lévesque A. Perceptions of adults with hearing impairment regarding the promotion of trust in hearing healthcare service delivery. Int J Audiol. 2015 Jan;54(1):20-8. doi: 10.3109/14992027.2014.939776
-
Thom DH, Kravitz RL, Bell RA, Krupat E, Azari R. Patient trust in the physician: Relationship to patient requests. Fam Pract. 2002 Oct;19(5):476-83.
-
Phonak. Counseling tools: Professional tools for hearing care professionals in order to make your work a little easier. https://www.phonakpro.com/com/en/resources/counseling-tools/family-centered-care.html.
-
Turnbull B. How do I implement family-centered care in my practice? Hearing Review. 2016;23(12):22.
-
Ventry IM, Weinstein BE. The Hearing Handicap Inventory for the elderly: A new tool. Ear Hear. 1982;3(3):128-134.
-
Cox RM, Alexander GC. The Abbreviated Profile of Hearing Aid Benefit. Ear Hear. 1995;16(2):176-186 .
-
Dillon H, James A, Ginis J. Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. J Am Acad Audiol. 1997;8(1):27-43.
-
Singh G, Barr C, Montano J, English K, Russo F, Launer S. Family-centered audiology care: Emotion and reason in hearing healthcare. Hearing Review. 2017;24(5):30-32.
-
Picou EM, Aspell E, Ricketts TA. Potential benefits and limitations of three types of directional processing in hearing aids. Ear Hear. 2014;35(3):339-352.
-
Crukley J, Scollie SD. The effects of digital signal processing features on children’s speech recognition and loudness perception. J Am Acad Audiol. 2014;23:99-115.
-
Blamey PJ, Fiket HJ, Steele BR. Improving speech intelligibility in background noise with an adaptive directional microphone. J Am Acad Audiol. 2006;17(7):519-530.
-
Bentler R, Palmer C, Mueller HG. Evaluation of a second-order directional microphone hearing aid: I. Speech perception outcomes. J Am Acad Audiol. 2006;17(3):179-189.
-
Gravel JS, Fausel N, Liskow C, Chobot J. Children’s speech recognition in noise using omni-directional and dual-microphone hearing aid technology. Ear Hear. 1999;20(1):1-11.
-
Thibodeau L. Comparison of speech recognition with adaptive digital and FM remote microphone hearing assistance technology by listeners who use hearing aids. Am J Audiol. 2014;23:201-210.
-
Comparison of wireless microphones. noise. Phonak Field Study News. http://www.phonaknhs.co.uk/Image/files/fsn_Roger_Microphone_Performance_Comparison.pdf. January 2015.
-
Preminger JE, Lind C. Assisting communication partners in the setting of treatment goals: The development of the goal-sharing for partners strategy. Sem Hear. 2012; 33(1):53-64.
-
Saunders G, Preminger J, Scarinci N. Family-centered care: Working with partners reporting “incongruent” hearing aid outcome. Hearing Review. 2017;24(2):26-30.

David Crowhen, MAud

Bettina Turnbull, MAud
About the authors: David Crowhen, MAud, is Audiologist & Brand Manager at Phonak New Zealand, and Bettina Turnbull, MAud, is Director of Audiology & Education for the Asia-Pacific Sales and Training Team at Sonova headquarters in Stäfa, Switzerland.


