By Suman Penwal1* and Chandrahas Chandanshive2
Department of Audiology, All India Institute of Speech and Hearing, Mysuru, India;1 Department of Audiology and Speech-Language Pathology, Topiwala National Medical College and B. Y. L. Nair Charitable Hospital, Mumbai, India.2
* Grade-1 Audiologist, All India Institute of Speech and Hearing, Manasagangothri, Mysuru-06.
Email: [email protected].
Abstract
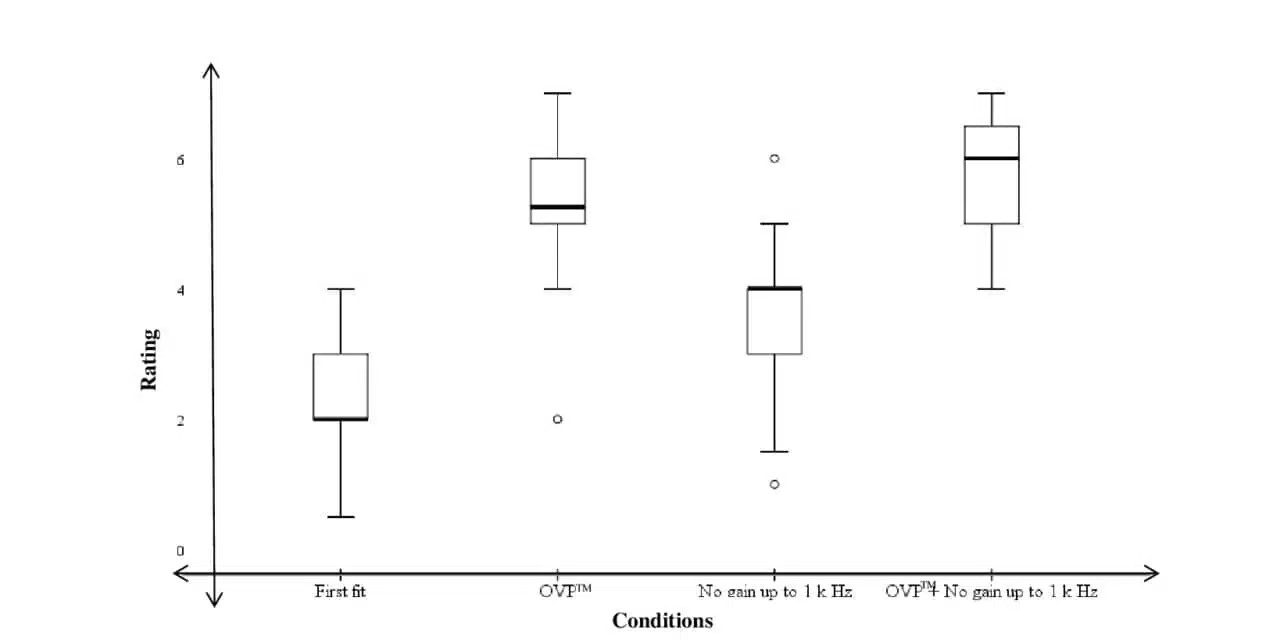
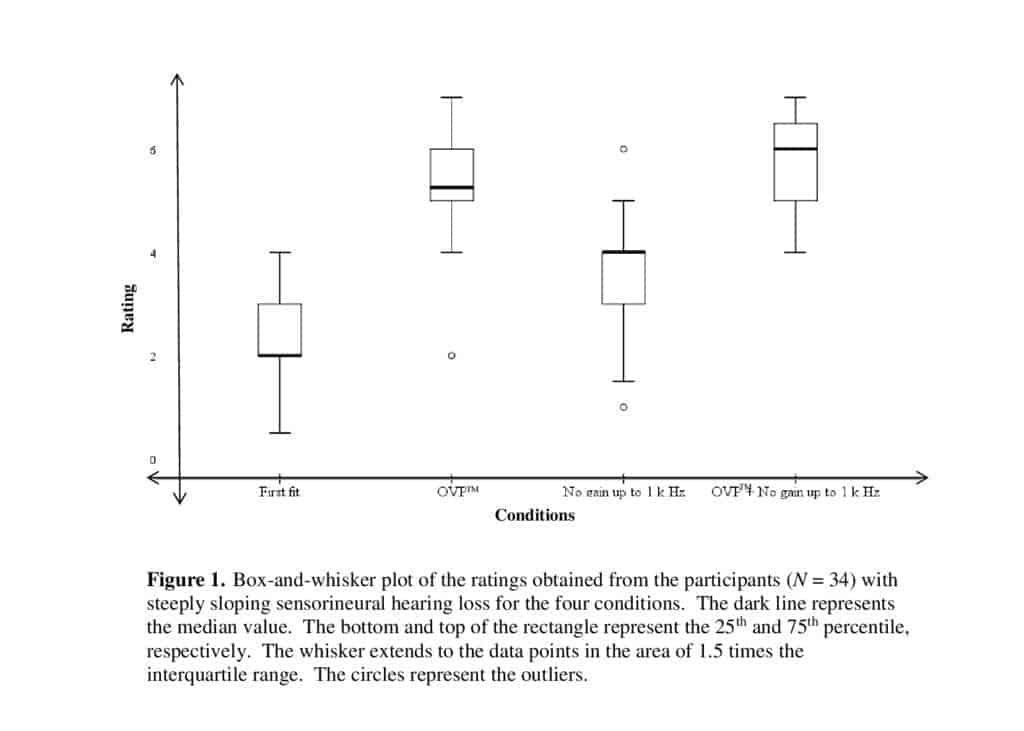
Thirty-four participants recruited in the study were requested to rate the quality of perception of their voice, wearing binaural hearing aids for the four conditions (First fit, OVPT, No gain up to 1 k Hz, and combination of OVPT and No gain up to 1 k Hz). A statistically significant difference was noted between all possible pairs of conditions (p< .001). The results suggest that perception of own voice of an individual with steeply sloping hearing loss was best rated with the combination of OVP and No gain up to 1 k Hz for the non-native language speakers.
Introduction
The normal audition was reported to play a keen role in effective communication by the construction of motor plans.1 This was observed to be an outcome of auditory feedback of one’s own speech.2 Hence, this creates the need for the near-normal perception of own voice to attain effective communication. However, it was noted that 59% of the naive hearing aid users reported their own voice perception as troublesome.3 This was also found to be the prime reason behind the denial of amplification.4 The restricted usage of auditory resources is a major cause of cognitive decline as hearing loss limits the ability to make optimum use of auditory resources.5 Therefore, one needs to accept the amplified signal, both environmental sounds, and their voice, to avoid later cognitive complications and communication breakdown.
Kuk et al6 noted that noise-reduction algorithms improve the perception of one’s own voice for the hearing aid user. They recruited participants in two groups, the former with less than 40 dB HL of hearing loss and the latter with more than 40 dB HL at low frequencies. The authors have found that the reduction in the gain at low frequencies resulted in unequivocal benefits between the groups with more benefit to the latter group. It can be inferred that the low-frequency cutoff is ineffective in improving the own voice perception in subjects with near-normal low frequencies.
Subsequently, the open-fit earmold was suggested to improve the perception of own voice.7 However, Kuk et al8 observed that increasing the diameter of the vent resulted in poorer directivity index in a directional hearing aid. Hence, venting was not considered effective in improving the own voice perception of the hearing aid user. It was alluded by Painton9 that the K-amp circuit in combination with the noise-reduction algorithm further reduces the gain of low frequencies. Stemming from the work done by Zwislocki,11 a deeply fitted, completely-in-the-canal hearing aid was recommended to resolve the problem caused by the occlusion effect.10,12 However, it was reported to cause physical discomfort to the hearing aid user and clinically arduous to obtain the seal between the bony canal and the hearing aid.13
The recently introduced Own Voice Processing (OVP) strategy in Signia hearing aids improved the perception of one’s own voice in hearing aids users by Høydal.3 However, the smaller sample size in the study was one of the major limitations. Therefore, the current study was designed to evaluate the acceptance of one’s own voice in non-native speakers of the English language using the recent algorithm and frequency-specific gain alteration. It was a secondary aim to examine efficacy of the algorithms for the population with steeply sloping sensorineural hearing loss. As in these cases, the benefits of noise-reduction algorithms are sparse.4
The study aimed to compare the own voice perception of the hearing aid user in four conditions with a) First Fit based on the Nx fitting formula; b) OVP; c) No gain up to 1 k Hz and, d) OVP with No gain up to 1 k Hz.
Materials and Methods
A purposive sampling technique was used to enroll 34 adults (30 males and 4 females) in the study. All the participants were in the age range of 48 to 85 years (mean age = 67 years, SD = 10.38 years) and had symmetrical mild sloping to profound sensorineural hearing loss (PTA 1 = 38 dB HL). All of them were naive users of amplification with no complaint of active middle ear effusion. Additionally, all the participants were native speakers of Hindi and Marathi languages.
Informed consent was obtained from the participants. It was ensured that the ”Ethical Guidelines for Bio-behavioral Research Involving Human Subjects“14 were followed. All the procedures involved in the study were non-invasive.
Materials and Procedure
The participants were fitted binaurally with the Signia Pure 7 Nx hearing aids, programmed using the company’s NX fitting algorithm. The medium power receivers of appropriate length coupled with vented sleeves were attached to the devices. The OVP procedure was carried out as per the fitting protocol given by the company. During the procedure, there was no reflective surface placed in the area of one meter (3.28 feet) around the client. The participant was asked to start counting over ‘21’ after a tone. As the software detects the voice, the default level of OVP was activated for the second and fourth conditions. In the third condition, the gain dials were kept at zero for 250 Hz to 1 k Hz frequency, from the fine-tuning section.
The blinded participants were instructed to read the Rainbow passage15 at the conversational level. The four conditions were counterbalanced. With this, the participants were instructed to rate the perception of their voice on a 13-point scale from 1 to 7, with the half-point interval adapted from Froehlich et al.16 The ratings were such that “7” denoted most natural perception and “1” indicated the worst or most unnatural perception of their voice.
Statistical analysis
The Shapiro-Wilk test of normality indicated that the data was not normally distributed. Hence, non-parametric analyses were carried out using SPSS software (Version 21, IBM Corporation, NY).
Results
The findings are reported in terms of comparison between the four conditions. The mean, median, standard deviation, and range of the obtained data are summarized in Table 1.
Table 1. Mean, median, standard deviation (SD), and range of the four conditions
| Conditions | Mean | Median | SD | Maximum score | Minimum score |
| First Fit | 2.26 | 2 | 0.94 | 4 | .5 |
| OVP | 5.38 | 5.25 | 1.08 | 7 | 2 |
| No gain up to 1 k Hz | 3.58 | 4 | 1.11 | 1 | 6 |
| OVP + No gain up to 1 k Hz | 5.83 | 6 | 0.76 | 4 | 7 |
Maximum rating = 7, minimum rating = 0
The non-parametric statistical test was conducted as the data was found to be non-normally distributed, using the Shapiro-Wilk test of normality. To establish whether a statistically significant difference existed between the conditions, a Friedman test was carried out. The results revealed statistically significant differences existed between the conditions [χ2 (3) = 85.53, p< .001].
Further, the Wilcoxon signed rank test incorporating Bonferroni’s correction was done to check for the significance of the difference in scores between pairs of conditions. It revealed that there was a significant difference between conditions 1 and 2 (Z = -5.04, p< .001), conditions 2 and 3 (Z = -4.34, p< .001), conditions 3 and 4 (Z = -4.97, p< .005), conditions 1 and 3 (Z = -4.28, p< .001), conditions 1 and 4 (Z = -5.10, p< .001), and conditions 2 and 4 (Z = -2.85, p< .005).
Discussion
The findings of the current study suggest that all four conditions are significantly different from each other. The data has shown maximum benefit in the perception of own voice with the fourth condition ie, OVP + No gain up to 1 k Hz. This observation is evident in the ratings (Figure 1) for the four conditions. The OVP strategy was reported to perform separate dynamic analyses of the environmental sounds and the voice of the hearing aid user with low-frequency optimization.
The research work done by Kuk et al6 has proven low-frequency cutoff to add improvement in the perception of one’s own voice. Secondly, the reduced occlusion in the ear canal attained with the reduction of low frequencies6,16 would be a possible reason behind the improved own voice perception. Further, the reduction in low frequencies was also reported to reduce the increased low-frequency energy inside the ear canal due to vocalization.10,18 However, it can be construed that low-frequency gain reduction and OVP in unison provide even better acceptance of the own voice by hearing aid users.
The findings are also in agreement with the work done by Høydal3 as the perception of one’s own voice was rated better than first fit alone. From the above two observations, it was inferred that the two conditions together complement each and produce better acceptance of the perception of speakers’ own voice. This can also be attributed to the requirement of higher SNRs for the perception of non-native language speakers.19 However, the reduction in the gain for the low-frequency signals can adversely affect the quality of the perception of environmental speech sounds. The current study has not considered the perception of external speech sounds.
Conclusion
From the findings, use of OVP is recommended, in combination with no gain up to 1 kHz for individuals with steeply sloping sensorineural hearing loss in a non-native context.
Acknowledgments
We would like to acknowledge our participants for being patient and considerate.
Declaration
The authors report no potential conflicts of interest. No funding was received.
References
- Borden GJ. Use of feedback in established and developing speech. Speech and Language.1980;(3):223-242.
- Perkell J, Matthies M, Lane H, et al. Speech motor control: Acoustic goals, saturation effects, auditory feedback and internal models. Speech Commun. 1997;22(2-3):227-250.
- Høydal EH. A new own voice processing system for optimizing communication. Hearing Review. 2017;24(11):20-22.
- Kochkin S. MarkeTrak V:“Why my hearing aids are in the drawer:” The consumers’ perspective. Hear J. 2000;53(2):34-41.
- Zekveld AA, Kramer SE, Festen JM. Cognitive load during speech perception in noise: The influence of age, hearing loss, and cognition on the pupil response. Ear Hear. 2011;32(4):498-510.
- Kuk FK, Plager A, Pape NML. Hollowness perception with noise-reduction hearing aids. J Am Acad Audiol. 1992:39-45.
- Kuk FK. Perceptual consequence of vents in hearing aids. Br J Audiol. 1991;25(3):163-169.
- Kuk F, Keenan D, Sonne M, Ludvigsen C. Efficacy of an open-fitting hearing aid. Hearing Review. 2005;12(2);26-32.
- Painton SW. Objective measure of low-frequency amplification reduction in canal hearing aids with adaptive circuitry. J Am Acad Audiol. 1993;4:152-156.
- Kuk F, Ludvigsen C. Ampclusion management 101: Understanding variables. Hearing Review. 2002;9(8):22-32.
- Zwislocki J. Acoustic attenuation between the ears. J Acoust Soc Am. 2005;25(4):752.
- LaFerle KR. Case studies using the Beltone Invisa CIC Hearing Aid. Seminars in Hearing; 1996;17(1):91-101.
- Garcia H, Staab W. Solving challenges in deep canal fittings. Hearing Review. 1995;2(1):34-40.
- All India Institute of Speech and Hearing. Ethical guidelines for Bio-behavioral Research Involving Human Subjects. http://www.aiishmysore.in/en/pdf/ethical_guidelines.pdf. Published July 2009.
- Fairbanks G. Voice and Articulation Drillbook. 2nd ed. New York: Harper and Row; 1960.
- Powers T, Froehlich M, Branda E, Weber J. Clinical study shows significant benefit of own voice processing. Hearing Review. 2018;25(2):30-34.
- Tonndorf J. Bone conduction. In: Tobias JV, ed. Foundations of Modern Auditory Theory: Volume 2. Academic Press; 1972:195-273.
- Van Engen KJ, Bradlow AR. Sentence recognition in native-and foreign-language multi-talker background noise. J Acoust Soc Am. 2007;121(1).
- Hervais-Adelman A, Pefkou M, Golestani N. Bilingual speech-in-noise: Neural bases of semantic context use in the native language. Brain Lang. 2014;132:1-6.