|
| Starkey’s Destiny 1600. |
Pediatric hearing amplification is a rapidly growing industry, fueled mainly by a sharp increase in early diagnosis and the ingenuity of technologists. A look at two of the leading manufacturers and a dialogue with an educational audiologist provide a glimpse of where this sector is headed in the new year.
For the people at Starkey, Eden Prairie, Minn, 2008 is definitely the year of Real-Ear Measurement (REM), a system of verifying the accuracy of a hearing aid fitting by measuring the acoustic signal generated within the patient’s ear canal.
Despite being a proven technology identified by the American Academy of Audiology as the standard of practice for verifying fittings, REM, for a number of reasons, has had difficulty gaining a solid foothold among hearing professionals. High cost and complexity of equipment, as well as space and time demands, have limited its regular usage to only about 23% of audiologists and hearing instrument professionals.
ON THE INSIDE
But with Starkey’s Destiny 1600 line, these problems are avoided, as the REM is completely integrated into the hearing aid itself, thus taking up no space in fitting rooms and eliminating the expense of external equipment, which has included a computerized control and display module, microphones attached to the patient’s head, and a speaker and boom.
Now it’s all inside the hearing aid, as every model in the Destiny 1600 line uses digital processing to perform calibrated real-ear measurements without external equipment. All models are equipped to work with Starkey’s Inspire OS programming software to measure real-ear responses. According to Jerry Yanz, senior staff audiologist at Starkey, it’s a “revolutionary development that allows practitioners to take advantage of REM accuracy without the expenditure of time, space, and money required in the past.”

|
| The Destiny 1600 with probe. |
The technology involves placing a small silicon probe tube under the hearing aid to measure actual acoustical production. The resulting measurement of the real-ear coupler difference (RECD) is what gives the accurate reading of the acoustic signal produced in the patient’s ear canal. The hearing aid itself is manufactured to digitally store the data of its own specific coupler response, rather than mere averages as have been typically used by hearing aid producers. At fitting time, the hearing aid goes into a special calibration mode; the receiver temporarily becomes a calibrated signal source, and the microphone becomes a probe microphone, picking up the acoustic signal from inside the ear canal rather than noise from the outside environment, thus enabling the hearing aid to make the RECD measurement. A significant advantage is that the system can be recalibrated according to the growth of the patient’s ear. And, of course, when working with children and infants, the need for a “behavioral” approach, ie, verbal questions and responses that work better with adults in determining the effectiveness of the hearing instrument, is eliminated.
Yanz says that the Destiny 1600 with integrated real-ear measurement, first introduced in April 2006, is the fastest-growing product line in the industry. It has other advanced features as well, including Active Feedback Intercept (AFI), which uses a digital algorithm to provide resistance to feedback. “For pediatrics,” Yanz says, “anytime you can eliminate oscillation, you increase the ability to hear higher frequencies, which is very important.”
The Destiny 1600 also has “directional speed detection” for switching between omnidirectional and directional reception, and “acoustic signature,” a set of environmental detection algorithms that, Yanz says, “improve comfort level in a noisy world.”
At Phonak, there is excitement about the Naida hearing instruments. With “Sound Recover,” a Phonak proprietary algorithm first seen in Naida, users can hear speech, birdsongs, telephones, and other high-frequency sounds “like never before,” according to Christine Jones, Manager, Wireless Technology, who adds, “Clinical results have shown dramatic improvements in speech understanding and production in just a few weeks of Sound Recover use.” Additionally, field studies show high user acceptance and rapid acclimatization. The CORE technology at the heart of Naida provides users with high-fidelity, stereo, and wireless connectivity. Communication Optimized Real-audio Engine (CORE) is also the basis for enhanced directionality, automatic functions, and wireless programming. MP3, Bluetooth, FM, and many other devices are easily accessed. This instrument comes in an “unexpectedly small” water-resistant casing.
STREAMLINED WORKFLOW
Also recently available, Jones says, is Phonak’s new dedicated mode for pediatric hearing instrument fittings. “The Junior Mode,” she reports, “provides fitters with a streamlined workflow for setting instruments for infants and young children, including DSL 5.0 and specialized pediatric defaults based on the age of the child.” Since the needs of children change most dramatically from birth to school age, “the software,” Jones says, “generates the most appropriate defaults for children aged 0-4 and different settings when a child age 5-8 is entered.” Initial defaults are based on evidence-based research in pediatric amplification and the guidance set forth by Phonak’s International Pediatric Advisory Board.
In FM systems, Phonak has launched Dynamic FM, a new wireless platform that boasts “the largest improvement in signal to noise ratio in the industry,” along with new features and benefits such as a multitalker network that can accommodate up to 10 different speakers, a dynamic speech extractor that maintains the high sound quality and optimal FM benefit over a wide range of conditions, and FM Monitoring, which, by checking battery status, microphone function, and audioshoe integrity, provides teachers with the assurances needed to focus their attention on teaching rather than trouble-shooting. The new Inspiro transmitter will offer these features when coupled with the new universal MLxi receiver, the Naida-integrated ML10i (which also offers the water resistance of Naida), and the MLxi Baha.
A DIFFERENT PERSPECTIVE
When it comes to an overview of pediatric hearing amplification, someone with a “view from the top,” you might say, is educational audiologist Dr Robyn Miller, AuD, CCC-A, AAA. Not that Miller is a leading producer of hearing aids or even associated with any manufacturers. On the contrary, she renders her services in the public school system of Montgomery County, Maryland, and maintains her office in an elementary school.
What Miller does know is children with hearing loss, and the most effective ways of addressing their issues. As a premed student at James Madison University, Miller had originally thought of becoming a pediatrician, but when she realized that “too much blood” was involved, she switched to speech pathology and audiology, going on to receive her MA in audiology from George Washington University and her PhD from A.T. Still University of Health Sciences. Her love and concern for children ultimately led her to work in the field of pediatric hearing loss, and she relishes the opportunity to help children make sense of the world around them.
Miller has been fortunate to see substantial progress made in her field. One thing she’s convinced of is that “with the new digital hearing instruments, cochlear implants (CI), and bone anchored hearing aids, children with hearing loss are now able to hear better in school and at home.”
Another important steppingstone, Miller believes, has been the Newborn Hearing Screening Program, a federally regulated program that identifies hearing loss problems in infants within 48 hours of birth, “before they and their mothers leave the hospital.” This has greatly facilitated early intervention, and, as Miller says, “early amplification is the key to the child’s speech and language development.” Before the program was started, children who may have had a mild or moderate hearing loss weren’t being diagnosed until they entered kindergarten. “Now,” Miller says, “these children are getting diagnosed at birth or within 1 year so that by the time they enter school, they’re not as delayed or not delayed at all.”
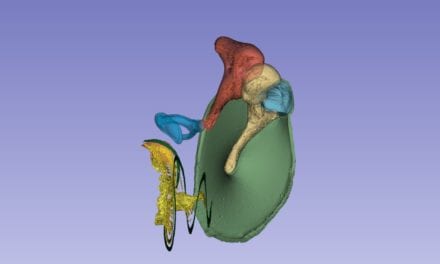
Miller has witnessed the advent of cochlear (inner ear) implants, which have dramatically improved hearing for those with severe and profound hearing loss. Introduced 11 years ago, these implants were at first done for one ear only, the reason being that residual hearing capacity is lost when the implant procedure is performed, so it was thought that given the newness of the procedure, it would be best not to tamper with whatever hearing might remain in one of the ears. In the past year, however, bilateral cochlear implants have come to the fore, as medical practitioners, Miller says, “are more optimistic about the implants and have learned that balance is not as much of a concern as was initially thought.” Miller identifies Advanced Bionics, manufacturer of the Harmony model implant, and Cochlear Corp, maker of the Freedom model implant, as two of the most widely used sources
|
| With Starkey’s Destiny line, REM is fully integrated into the hearing aid. |
Miller emphasizes, however, that neither cochlear implants nor hearing aids restore hearing totally. “It’s not like eyeglasses, where you can regain normal eyesight most of the time. There is still difficulty with clarity and understanding. Much depends on the age at which the child first receives amplification, but whatever the age, the brain needs to learn how to use the sounds it’s receiving—it doesn’t happen naturally. Cochlear implants are most successful when the parents are very involved in a supportive role, and when there is a great educational team including teachers of the deaf and an audiologist.” Cued speech, Miller adds, a system of using hand signals to indicate sounds that lips make (not sign language), can also be very useful in achieving optimum results.
The point, Miller says, is that “CI is not a miracle worker. It requires a lot of family commitment, teamwork with the school, and rehab after activation of the CI.” The procedure is expensive, as well, costing about $10,000 for each ear. Federal medical assistance for children will pay for one ear, and so will most insurance companies, while some companies, Miller reports, are now paying for the bilateral procedure.
Overall, “the benefits of CI are huge,” Miller says. “In my school, I have a pair of twins who were implanted at 1 year, and now, at almost 3, they are above their age level in all of their speech and language.”
Yet another key technical advance is the FM systems used in a classroom setting to overcome background noise. The teacher wears a microphone, and the child has a receiver that is either part of the hearing aid, or attached to the hearing aid or implant. This enables the hearing-impaired child to hear the teacher’s voice above the noise in the classroom.
Miller is also encouraged by the growth in acceptance of children who have a hearing impairment by other children. “Kids are getting more open to children with special needs. The role of the educational audiologist is key to making everyone feel comfortable in this situation.”
It is estimated that 2% of all youngsters under the age of 18 have hearing loss, with most cases congenital in nature. Miller believes that the advances in treatment and growth in usage of hearing aids and implants are a result of early diagnosis, and that such diagnosis is the crucial factor in successful hearing amplification. “We’re already seeing huge improvements,” she concludes, “but in the next 5 years, with digital microchips, the technology should explode.”
Alan Ruskin is staff writer for Hearing Products Report. He can be reached at [email protected].