
|
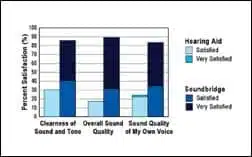
| FIGURE 1. Vibrant Soundbridge middle-ear implant recipients reported improved sound clarity and overall sound quality compared to their hearing aid, based on three subscales of the Hearing Device Satisfaction Scale. |
Approximately 31.5 million Americans—about one in 10—suffer from some kind of hearing loss.1 The most common form of hearing loss is sensorineural (SNHL), which affects an estimated 60% of this population. Research has shown that only one in five people who could benefit from a hearing aid actually wear one,2 which leads to 24 million people in America with hearing impairment who do not use hearing instruments. People with moderate SNHL are not considered good candidates for cochlear implants, due to relatively good residual hearing. Considering the usage and satisfaction statistics, however, there is clearly an unmet need for people with hearing impairment who fall through the cracks between cochlear implants and hearing aids (Figure 1).
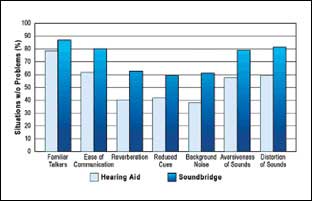
Dissatisfaction rates may be due, in part, to the specific audiometric configuration of the individual’s hearing loss. Patients with normal hearing—or at worst a mild loss for low frequencies in combination with a severe or even profound degree of loss for the mid- to high frequencies—present a challenge in rehabilitation in view of the highly variable amplification needs across the frequency range. People with relatively normal or mild loss at low frequencies can manage one-on-one or small-group conversations in ideal listening situations (eg, low-level background noise, minimal reverberation, familiar topics or speakers), especially when speech reading cues are provided. However, when presented with a variety of sound environments, with various levels and types of background noise and often no visual cues, these patients are placed at an additional disadvantage by their hearing impairment (Figure 2).3
|
| FIGURE 2. Middle-ear implant recipients as a group reported significant improvement with the VSB compared to the subject’s own hearing aid on all seven subscales of the Profile of Hearing Aid Performance (PHAP), which measured perceived benefit in a variety of listening situations. |
The presence of good low-frequency hearing thresholds when using conventional amplification, especially if combined with an occluding earmold, can lead to an increased awareness of the known limitations of conventional amplification. Patients with a high frequency loss may be potentially less tolerant of, and more irritated by, issues such as occlusion, poor sound quality, the physical sensation of the earmold, and the visibility of the hearing aid, in comparison with patients presenting with a flat, moderate to severe loss.4 Additionally, the increased high frequency gain requirements of a hearing aid that is configured to treat such a hearing loss place the patient at greater risk of experiencing feedback. As a consequence of their dissatisfaction with conventional amplification, such patients with predominantly high frequency hearing loss may choose to ignore their specific amplification needs altogether and elect to struggle on in adverse situations without any assistance from amplification, despite the added stress in communication and negative impact on their satisfaction and lifestyle.2

|
| FIGURE 3. The Audio Processor (AP) is the only external component to the system. This contains the microphone and processing electronics, as well as a size 675 hearing aid battery. |
Addressing High Frequency SNHL
The Vibrant Soundbridge® recently received an expanded indication for use in adults who have moderate to severe sensorineural hearing loss (SNHL) and desire an alternative to acoustic hearing aids. The middle ear device is now further intended to treat moderate to severe SNHL for adults who cannot achieve success or adequate benefit from hearing aids, or cannot medically tolerate hearing aids due to conditions such as chronic perichondritis of the ear, chronic otitis externa, atresia of the ear canal, congenital malformations, or skin reaction from the hearing aid. Prior to receiving the device, it is recommended that an individual have experience with appropriately fitted hearing aids; in clinical trials, the subjects were required to be users of acoustic hearing aids for at least 3 months before evaluation for inclusion in the study.

|
| FIGURE 4. The internal component of the Vibrant Soundbridge®, the Vibrating Ossicular Prosthesis (VORP), is shown on the left. At the end of the VORP is the tiny Floating Mass Transducer (FMT), which is shown here under magnification, and in a size comparison to a dime. It attaches directly to the incus. |
The Soundbridge (Figures 3-4) consists of two primary components: the Vibrating Ossicular Prosthesis (VORP) and the Audio Processor (AP). The surgically implanted VORP contains a magnet surrounded by a receiving coil, a demodulator package, a conductor link, and the Floating Mass Transducer (FMT). The AP is worn externally on the head, posterosuperior to the pinna, at a 45° angle to the ear canal. It contains a microphone, a signal processor, telemetry electronics, and a magnet, and it is powered by a standard 675 zinc air battery.
The AP is held to the scalp by magnetic attraction between the implanted magnet in the VORP and the magnet in the AP. The AP can be worn under the hair and is therefore not usually visible. The implant utilizes hearing technology that physically drives the ossicular chain, bypassing the ear canal and tympanic membrane. Unlike a hearing aid, which amplifies sound, the Soundbridge is a direct drive prosthetic that mechanically vibrates the bones in the middle ear without surgically altering the structures of the middle ear.
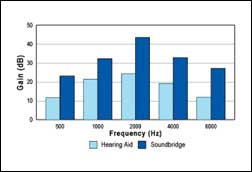
Locating the hearing aid’s sound source in the ear canal typically causes distortion and occlusion—common sources of dissatisfaction among people with high frequency hearing loss. However, the implant leaves the outer ear free of obstruction, overcoming these problems. Additionally, by entirely removing the hearing aid loudspeaker, the listener benefits from significantly increased functional gain, while greatly decreasing the potential for feedback (Figure 5).
|
| FIGURE 5. The middle-ear implant increased functional gain at all frequencies when compared to the recipients’ previous hearing aids. This increase was statistically significant (p<.02) at 1500, 2000, 4000 and 6000 Hz. All recipients’ preoperative hearing aid fittings were evaluated for appropriateness prior to their inclusion in the clinical trial. |
Direct Drive Technology
One of the major theoretical advantages of the direct drive approach over conventional acoustic devices is the potential to provide improved sound quality. Luetke et al5 have observed that direct drive users perceived better sound quality than with conventional acoustic hearing aids, which may be attributed to:
- Increased signal delivery in the higher frequency bands;
- Improved signal coupling (bypassing the tympanic membrane);
- Reduction in acoustic feedback;
- No insertion loss;
- No occlusion effect;
- Reduced distortion from canal resonances, and
- Proximity to the cochlea (signal source located closer to the inner ear).
The FMT is a totally enclosed transducer that uses inertial drive to impart mechanical energy directly to a vibrating structure of an ear. Though tiny, the mechanical vibrations that the FMT imparts can be comparable to very high sound pressure levels (SPL). The FMT has been specifically designed to mimic the vibratory responses of the middle ear. It is capable of delivering mechanical stimulation to the middle ear throughout the entire speech-related audiometric frequency range.
When evaluating the FMT against a hearing aid by using the human temporal bone model and recording the output of a laser Doppler vibrometer, Ball and Katz found that the FMT placed in a temporal bone and driven at a level equivalent to 110 to 115 dBSPL resulted in accurate reproduction of speech and music at the stapes footplate in the temporal bone. High frequency information content was even present at frequencies higher than 7 kHz. The hearing aid receiver produced a signal for both speech and music at the stapes footplate when driven at 110 to 115 dB SPL. However, high frequency information was largely absent (Figure 6). Music was also degraded, and only a limited amount of high frequency information content was present.3
Who Are Likely Candidates?

|
| “Hybrid Hearing Device Being Developed.” January 2007 News. |
In addition to patients with moderate to severe hearing loss across the audiogram, the Vibrant Soundbridge offers a unique solution for patients with more complex “ski slope” audiograms. In some ways, low frequency residual hearing can help these patients “get by” in situations where they have learned to compensate, but it places them at a clear disadvantage in group discussions, work situations (eg, teleconferences where speech reading is not applicable), and environments with high levels of background noise (eg, restaurants). Many of these individuals have tried hearing aids, but are not satisfied with the outcome.
Potential Vibrant Soundbridge candidates would be commonly classified as “unsuccessful” hearing aid users; they choose not to wear their hearing aids all the time, whether due to comfort or sound quality issues, lack of benefit, intractable feedback, or the inability to achieve the appropriate levels of functional gain. Ironically, hearing aids can further frustrate these candidates by blocking the ear canal from low frequency sounds that these individuals normally would hear, and by distorting higher frequencies.
In addition to the need for high frequency hearing in a work setting, the middle-ear implant has clear applications for people with difficulty in hearing the high frequency sounds at home, including music or children’s voices. The Vibrant Soundbridge serves as an alternative for those individuals who simply cannot wear a conventional hearing aid due to medical or anatomical conditions that make hearing aid use problematic or impossible.
This article was submitted to HR by Darla Franz, MA, director of education and corporate communications at Med-El Corp, Durham, NC, and Rebecca Novak Tibbitt, senior consultant, RNT Communications LLC. Correspondence can be directed to Darla Franz, Med-El Corp, 2222 E Hwy 54, Suite B-180, Durham, NC 27713; email: .
References
- Kochkin S. MarkeTrak VII: Hearing loss population tops 31 million people. Hearing Review. 2005;12(7):16-29.
- Scherer MJ, Frisina DR. Characteristics associated with marginal hearing loss and subjective well-being among a sample of older adults. J Rehabil Res Dev. 1998;35:420-6.
- Uziel A, Mondain M, Hagen P, Dejean F, Doucet G. Rehabilitation for high-frequency sensorineural hearing impairment in adults with the Symphonix Vibrant Soundbridge: A comparative study. Otol Neurotol. 2003;24(5):775-783.
- Goode RL, Krusemark J. Advantages of a new miniature hearing aid for mild to moderate hearing loss. Laryngoscope. 1999;109:1919-23.
- Luetje CM, Brackman D, Balkany TJ, et al. Phase III clinical trial results with the Vibrant® Soundbridge implantable middle ear hearing device: A prospective controlled multi-center-study. Otolaryngol-Head Neck Surg. 2002;126: 97-107.



