
By Christopher Schweitzer, PhD
Toward a better understanding of when and why open fittings are “successful”
Open-fit hearing aids, when applied to appropriate candidates, produce an unambiguous reduction in listener complaints about sound quality. However, the “uncertainty” of the value proposition remains—especially when hearing in noise is one of the primary goals of the patient.
|


Open-fit hearing aid styles have been an especially fast growth phenomenon in the United States, where they make up about 24% of all the BTEs dispensed,1 and are also growing in popularity in Europe and elsewhere. The apparent delivery of reduced consumer complaints has progressed well enough to encourage nearly every major hearing aid manufacturer to introduce a variation on the open-fit theme. This impressive sales growth notwithstanding, it should not go without some thoughtful review by dispensing professionals of the premises and properties of this type of hearing device.
The primary audiological candidates for open products are individuals with relatively normal low-frequency hearing loss and mild-to-moderately sloping high frequency loss. That, by most analyses, describes the great untapped hearing loss, non-user category in the comprehensive Knowles MarkeTrak surveys published by Kochkin.2,3
Younger consumers generally have relatively mild hearing loss, situational communication stress, and considerable complaints about traditional hearing aids. In fact, if one were to configure complaints regarding hearing aids (we’ll call it ear-i-tation) scaled against hearing loss, it might be reasonable to draw a diagram that would resemble Figure 1. This is, of course, not based on empirical evidence, but reasonably informed supposition.
However, it seems axiomatic that, as hearing loss gets more severe, the ratio of complaint to benefit generally tilts in favor of benefit. In contrast to the full-time needs of consumers who have more severe hearing impairments, consumers who have milder losses are more typically only “audiologically stressed” in specific situations. They can be expected to be more aware of—and complain about—the physical and sound processing properties of hearing aids.
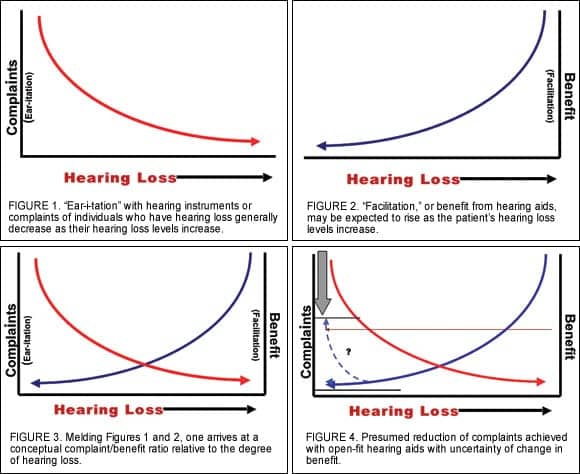
If a simplistic scale of “benefit” (we’ll call it facilitation) were added to this portrayal, the function related to hearing loss might reasonably look like Figure 2. Plotted together, a scenario resembling Figure 3 emerges. It should be noted that the clinical validity and details of these assumptions are untested, and they are assumed to vary among individuals who have similar hearing loss but different communication demands and cognitive abilities. However, this type of conjecture encourages a discussion of how the complaint/benefit vector might be calculated.
As Figure 4 suggests, it seems clear that open-ear hearing aids are designed to deliver a reduction in the complaint factor when they are applied to candidates with the appropriate audiological profile. What remains unclear, however, is the “location” of the benefit component in this type of fitting. It is precisely this “Value Uncertainty” with open-ear products that rarely receives attention in the sales and promotional materials (Figures 5-6) which tend to concentrate on product benefits like “naturalness of sounds” or reduction in occlusion.
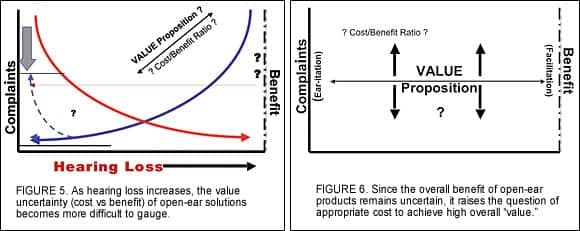
For any product, the value is defined as its benefit divided by its cost. Given the milder degree of hearing loss for which open-fit products are intended, the “benefit” (and/or lack of ear-i-tation) of the products would need to be greater than more conventional fittings given the same price and value levels. Questions that this line of thought raises for dispensing professionals include “Should these products be priced the same as other advanced technology hearing aid products?” and “Is the cost/benefit ratio as favorable as for other advanced products fit to more severely impaired recipients?”
Human Acoustics: Do Our Ears Selectively Hear from the Front?
One element that seems to have been given insufficient treatment in the public discussion is the spatial acoustic properties of natural and open-ear sound delivery. Carefully obtained physical acoustical measurements by Shaw4 and Kuhn5—as well as measures on KEMAR (the standardized representation of the average head and torso) reported 30 years ago6—show quite unambiguously that sound pressure levels at the tympanic membrane are not strongest for sounds arising from directly in front of the listener. Clearly, sound selectivity varies with frequency, but for many frequencies (generally greater than 500 Hz), there is a bias in favor of the region to the side and partly around the back of the ear’s ipsilateral side. Recent measures in our lab, both on artificial and real ears, further confirm that sounds from the “look-to-listen” region (forward) are less intense at the eardrum than sounds of equivalent energy and distance from the side and some regions of the back.
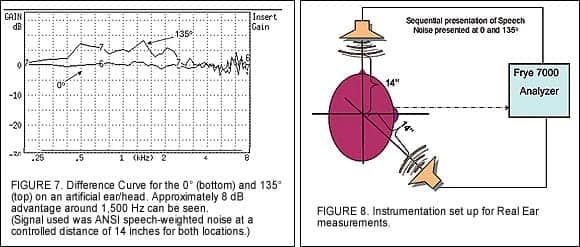
Figure 7 shows the difference in an open-ear fitting for sounds coming from 0° (in front) versus 135° (behind and off the shoulder on the same side as the test ear) at the same controlled level at the top of the head. The artificial ear mounted in the head structure, manufactured by Earmold Design Inc (EDI), generally shows representative acoustical properties of the average human ear. The difference curve indicates a greater sound pressure level (SPL) for the 135° sound source. Figure 8 shows the instrumentation set up for these measures and those that follow on open-ear type hearing aids.
The assumption of directional microphone configurations is that forward-arriving sound sources will be rendered to an advantageous SPL over those of non-frontal sound sources. In most instances, that improvement can be shown to be the case in standard hearing aid couplings and are the basis for most methods of characterizing the Directivity Index.7
However, if the ear canal is deliberately left unblocked, the open canal conditions are presumed to persist, and that includes greater sound pressures (from equally intense sources) arriving at the tympanic membrane from non-frontal regions. Does this create problems and/or reduce the benefit factor for these types of hearing aids? This was a question of interest in the electroacoustical measures reported below.
Directivity and the Open Ear
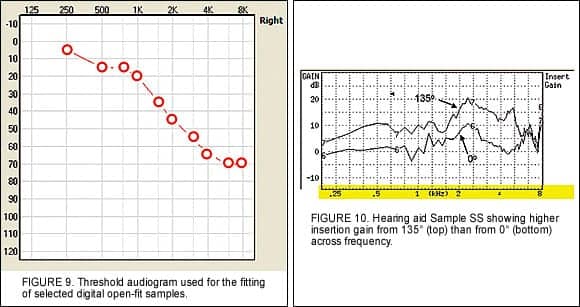
Measurement Method. Open-ear type hearing aids from 6 major manufacturers were attached to an artificial ear and head. A standard audiometric configuration (Figure 9) was used to generate the manufacturer’s fitting proposal for each sample. For these measures, if a noise reduction algorithm was available, it was deactivated to avoid influencing the continuous speech spectrum noise input signal. Feedback cancellation was also deactivated if available as a fitting option.
The speaker was located at a distance of 14 inches to the center of the head and level to the center of the ear (Figure 8). The sound source was fixed at 65 dB SPL at either 0° (front) or 135° (over the back shoulder). The signal level was referenced to a position at the center of the head of the manikin. However, the reference microphone was turned off during the subsequent measurements to exclude unwanted influence from amplified sound leaking back to the reference microphone.
Figure 10 shows an example of the output of one of the open-ear products for the Front (0° Top) minus Back (135° Bottom). The hearing aid in this sample is in the “directional” mode, yet the sound is generally more intensive in the ear canal for the rear sound source than for the front sound source. Clearly, this is not the result that most dispensing professionals would have expected.

An average of eight selected frequencies were taken to generate a modified Front-Back Ratio (FBR) where the 135° output values are subtracted from the 0° values. Table 1 shows the results for the 12 measured samples/configurations. Those with positive numbers show an advantage of the Front-over-Back for these measures. However, it should be noted that most do not (eg, Samples KK, PP, QQ, RR, SS, WW, XX, YY).
It is also important to realize that several of these samples did not have a directional mode, or a configurable directional mode. All were fit using the audiogram shown in Figure 9 without adjustment other than those related earlier to improve the integrity of the measurements. In every case, multiple measures were obtained to increase the confidence of the data.
Clinical Implications
The measurement methodology used here is by no means either standardized or assumed to be representative with regards to the complexities of advanced hearing aid operations. For example, some are designed to alter the null pattern (maximum reduction) of sounds from spatial locations according to various level and frequency determinations. The use of a single speaker for the sound source and a broadband noise clearly limits the operations of such adaptive directional systems which actively attempt to sort various simultaneously occurring sounds and deal with them intelligently.
However, from the standpoint of raw simplicity, it seems clinically pertinent to know that, if a single sound arrives at the head from the side, that signal may have a more intensive SPL at the eardrum than a subsequent one that arrives from directly in front. Clearly, closer study of this problem with more sophisticated instrumentation is desirable.
Considerable efforts in research labs and on standards committees have been directed towards new methods to characterize directionality, especially with advanced adaptive modes of configuration.8,9 However, for clinical environments, these are difficult to implement and their usefulness for open-fit hearing aids is unproven. Most clinicians may want to know, for example, that in an unoccluded ear, sounds arriving from directly in front are unlikely to be more intense than from other directions on the same side of the head.
User Survey. Returning to the basic question, “Can benefit with open-fit hearing aids be shown to be as impressive as a reduction of the user’s complaint,” the answer must obviously include consumer opinion, as electroacoustic determination is anything but straightforward.
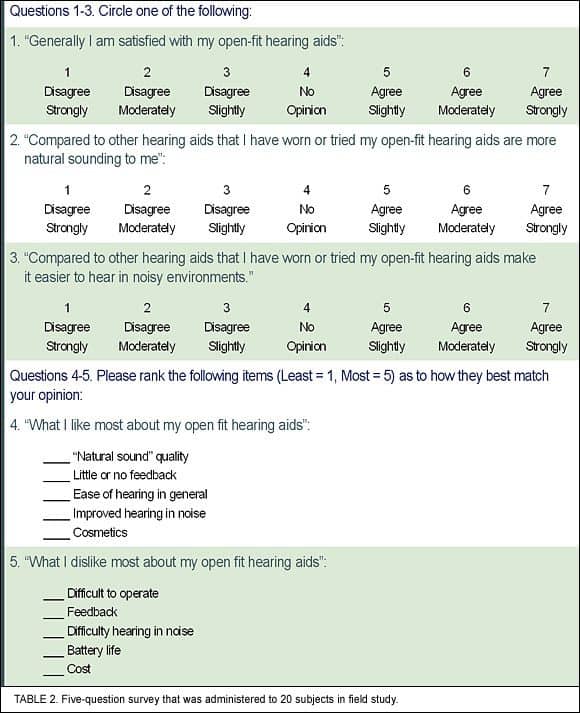
A simple survey questionnaire (Table 2) was prepared and circulated to current users of open-fit products to obtain a limited look into subjective valuation of the delivered benefit. Three questions were asked to scale the magnitude of “overall satisfaction,” “general ease of hearing,” and “ease of hearing in noise.” The remaining two questions asked for a rank-order of attributes “Liked” or “Disliked” about open-fit hearing aids.
The 20 survey respondents represented users of five different hearing aid brands. Again, this was not a comprehensive data collection attempt, but rather a quick attempt to explore the findings of the electroacoustic measures recorded in Table 1, which suggests that benefit in noise might have limitations due to the anatomical acoustics.
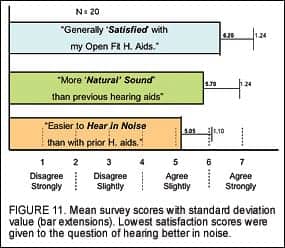
Analysis of Variance indicates a significant difference among the three questions. Clearly the “ear-i-tation” factor, or the complaint comment, was subjectively improved, as indicated by both the high ratings of Overall Satisfaction and the Natural Sound indications. Hearing in Noise appears slightly improved over users’ previous hearing aids, but with a less robust agreement indication. It should be noted that 14 of the 19 survey respondents were fit with the same model of open-ear hearing aids, which ranked the highest in the modified Front-to-Back electroacoustic measures discussed earlier (Sonic Innovations Ion, which also corresponds to Sample OO in Table 1). It is difficult to speculate whether or not this improved the rating on the Hearing in Noise question, but it deserves mention.
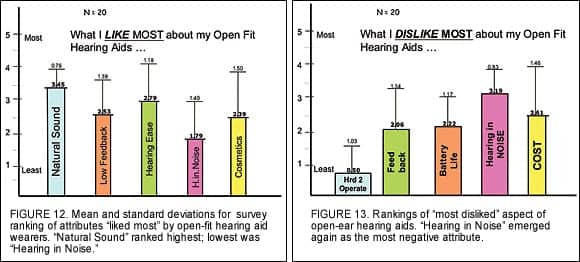
Figures 12 and 13 show the results of the two questions in which respondents were asked to rank what they “Most Liked” and “Most Disliked” about their open-fit hearing aids. The sampling method only queried those listed response choices (eg, alternative answers were not allowed). Highest among the Most Liked (Figure 12) choices was “Natural Sound,” followed by “General Ease of Hearing,” “Low Feedback Problems,” “Cosmetics,” with “Hearing Better in Noise” coming in last.
The low response ranking of hearing better in noise showed internal consistency by emerging as the “Most Disliked” attribute (Figure 13). Interestingly, it exceeded Cost, as well as Battery Life, Feedback, and Difficulty in Handling (Hard to Operate). Other research that implemented a more conventional survey10 on a sample of 10 subjects showed a somewhat different trend using a single manufacturer’s product.
Discussion
There are clear limitations to the instructional power of the present findings in terms of sample size, polling method, etc. However, they tend to support the suppositions of the first part of this article to a guarded extent: Namely, open-fit hearing aids, when applied to appropriate candidates, produce an unambiguous reduction in listener complaints about sound quality. However, the “uncertainty” of the value proposition remains—especially when hearing in noise is of high importance to the user.
The overall value proposition of open-fit hearing aids is a topic that warrants more systematic study. A distinct separation of types of open products should contribute further to understanding the issue, in addition to developing and implementing a larger user survey base.
Finally, the properties of anatomical acoustics should be given a more thorough look, especially as clinicians move towards more extensive routine application of open-fit hearing aids.
References
1. Strom K. The HR 2006 Dispenser Survey. The Hearing Review. 2006; 13(6):16-39.
2. Kochkin S. MarkeTrak VII: Customer satisfaction with hearing instruments in the digital age. Hear Jour. 2005;58(9): 30-43.
3. Kochkin S. MarkeTrak V: “Why my hearing aids are in the drawer:” The consumer’s perspective. Hear Jour. 2000;53(2):32-42.
4. Shaw E. Transformation of sound pressure level from the free field to the eardrum in the horizontal plane. J Acoust Soc Am. 1974; 56: 1848-1861.
5 Kuhn G. Physical acoustics pertaining to directional hearing. In: Yost W, Gourevitch G, eds. Directional Hearing. New York: Springer-Verlag;1987:3-25.
6. Manikin Measurements. Proceedings of Manikin Measurement Methods Conference, Washington, DC;1976:8.
7. Ricketts T. Directional hearing aids: New designs and predictions applied to old concepts. Hear Jour. 2006;59(6):10-18.
8. Dittberner A, Bondy J. A method is proposed to evaluate directional-microphone strategies. Hear Jour. 2006;59(7):28-35.
9. American National Standards Institute. Method of Measurement of Performance Characteristics of Hearing Aids Under Simulated Real-Ear Working Conditions (ANSI S3.35);2004.
10. Yanz JL. Open-ear fittings: An entry in hearing care for mild losses. The Hearing Review. 2006;13(2):48-52.
Correspondence can be addressed to HR or Christopher Schweitzer, Hear 4-U International, 2770 Arapahoe Rd, Ste 126, LaFayette, CO 80026; e-mail: [email protected].
Open Fitting on HR Online
Open-fit hearing aids are one of the hottest topics in hearing care today. In the August 2006 HR (available at the www.hearingreview.com/Archives), retired Mayo Clinic audiology director Darrell Rose, PhD, discusses earmold modifications and the potential to serve larger populations with open and mini-BTE devices. In May 2006, another former director of audiology at Mayo Clinic, Dave Fabry, PhD, presents “Facts vs Myths: The ‘Skinny’ on Slim-Tube Open Fittings” in which several misconceptions—such as “Open-fit hearing aids with omni-directional mics provide improved speech recognition in noise by providing improved audibility”—are debunked. In January 2006, Mark Flynn, PhD, and colleagues address “Thin-Tube Open Fittings: Preferred Patient Populations and Study Results,” noting that it is also possible to use a standard earmold if more amplification is required.



