|
| Francis Kuk, PhD,(left) is director of Audiology, at the Widex Office of Research in Clinical Amplification (ORCA), Lisle, Ill, and Lars Baekgaard, MS,(right) is a research engineer at Widex A/S, Vaerloese, Denmark. |
The popularity of behind-the-ear (BTE) hearing aids has soared in the last few years. The latest industry statistics showed that more than 50% of hearing aids sold in the United States during 2007 were BTEs.1 A key reason for the renewed interest in BTEs is that this style of hearing aid has undergone a substantial metamorphosis.
Along with the smaller size, today’s BTEs are more stylish, more cosmetically appealing, and more functionally versatile. At the same time, the manner to which current BTEs are coupled has led to a plethora of names and terms that may confuse even the most experienced clinicians. This article will try to provide a structured approach to distinguish the various forms of BTE couplings in order to help demystify some prevailing beliefs.
Basics: Six Basic BTE Couplings
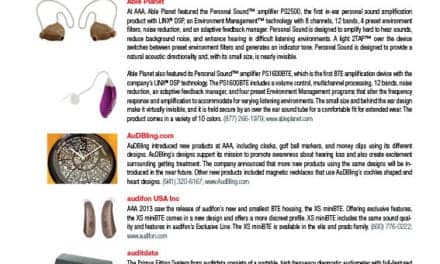
Today’s BTE couplings can be broadly grouped by two distinct dimensions: one involving the “diameter of the tubing” and one involving the “openness” of the fittings. Using these two dimensions and adding thin-wire fittings, one can classify today’s BTE couplings into six categories (Figure 1):

|
| FIGURE 1. The six possibilities of BTE couplings used in today’s fittings |
Standard (traditional) occluded fittings. A “standard fitting” typically refers to the use of a BTE hearing aid (of any size) coupled to an earmold that uses a #13 tubing (inner diameter of 1.9 mm). Although the ear canal is typically occluded, the use of vents of various dimensions allows degrees of sound leakage into and out of the ear canal.
Standard (traditional) open fittings. Traditionally, an “open fitting” refers to the use of a BTE coupled to a #13 tubing or a Libby Horn (3 or 4 mm bore opening) where the ear canal is left unoccluded.
These two categories existed for decades, until the more recent widespread implementation of thin-tubing and receiver-in-canal (RIC, also called receiver-in-the-ear or RITE) models created four more general fitting categories for BTEs:
Thin-tube occluded fittings. This refers to the use of a miniature BTE hearing aid that is coupled to an ear insert or earmold (vented or unvented) via a tubing of approximately 0.8 mm inner diameter.
Thin-tube open-fittings. The current open-fittings (or open-ear fittings) refer to the use of a miniature BTE hearing aid that is coupled to an open ear-tip via a 0.8 mm (inner diameter) tube. Ideally, this leaves the ear canal open for its natural resonance. The distinction between thin-tube open-fittings and traditional open-fittings is the diameter of the tubing used (0.8 mm vs 1.9 mm).
Thin-wire occluded fittings. This refers to the use of a BTE hearing aid where the receiver (loudspeaker) is placed outside of the hearing aid case and inside the wearer’s ear canal. A thin-wire that is insulated in a thin-tube connects the receiver to the BTE case. The receiver is typically housed inside an occluding ear insert (vented or unvented). This is also commonly known as a RIC or RITE hearing aid.
Thin-wire open fittings. To maintain the openness of the ear canal, the receiver of a thin-wire (RIC/RITE) hearing aid must be smaller than the diameter of the ear canal to leave it unoccluded for a majority of its wearers. The ear-insert, in which the receiver is encased, must remain small as well.
Selection: Where to Start?
The rationale for choosing a specific coupling method is relatively straightforward if one understands the differences between:
- An open versus an occluded fit;
- A standard (#13) tube versus a thin-tube; and
- A thin-tube versus a thin-wire (RIC) fitting.
In the subsequent comparisons, we will use the frequency output of a standard occluded-ear fitting (ie, a BTE hearing aid coupled to a standard #13 unvented occluding earmold) as the reference for our discussions.
Open-ear vs Occluded-ear Fittings
In general, the main reason for choosing an open-ear fitting, among many possible reasons, is the minimization or total elimination of the occlusion effect (OE).2 The reduction of OE is possible because the unoccluded ear canal in an open-ear fitting allows the low-frequency SPL that is generated during vocalization to escape the ear canal.
It is commonly accepted that the accumulation of low-frequency SPL during vocalization is the main source of the “hollow voice” complaint. Kuk et al3 has estimated that the average objective occlusion effect with a typical occluding earmold is about 20 dB. In addition, each 1 mm vent diameter leads to a reduction of the OE by about 4 dB.4
This means that, for the average ear to be completely clear of the OE, the equivalent vent diameter of the earmold should be larger than 5 mm. This vent size is almost impossible for a standard custom ITE hearing aid, or a typical earmold, to achieve. True open-ear fitting is the only possible option to achieve a complete elimination of the objective OE.
On the other hand, an open-ear fitting has its challenges and caveats. Kuk and Keenan5 provided a discussion on the effect of vent diameter on hearing aid performance. This can be summarized as:

|
| FIGURE 2. Effect of vent diameter and open fitting on hearing aid output. As much as 20 dB of output reduction is experienced at 250 Hz with a 3 mm vent. With an open-ear fitting, output reduction is seen up to 2000 Hz, with almost 10 dB reduction at 1000 Hz. |
Caveat #1: Loss of low-frequency output. The output of a hearing aid below 1000 Hz is significantly reduced with an increase in vent diameter.5 Figure 2 shows the effect of vent diameter on the output of a hearing aid. For example, as much as 20 dB of output reduction is experienced at 250 Hz with a 3 mm vent diameter. With an open-ear fitting, output reduction is seen up to 2000 Hz with almost 10 dB output reduction at 1000 Hz. This suggests that individuals with substantial gain requirements in the low- to mid-frequencies (up to 1500 Hz) may be under-fit with an open-fit hearing aid. An occluded earmold, even with substantial venting (3 mm), may be more desirable.
Caveat #2: Reduction of maximum available gain. Kuk and Keenan5 showed that the maximum gain before feedback at 3000 Hz decreased from around 40 dB in a completely occluding earmold, to about 30 dB in a 3 mm vent, and 25 dB in an open-ear tube fitting. This is the result of increased feedback potential with the increased acoustic leakage.
This decrease in available gain has at least two implications. First, it affects the ability of the hearing aid output to match a prescribed gain/output target. This, in turn, could potentially affect sound quality and recognition of soft sounds, including speech.
Second, in order to ensure adequate available gain, it is imperative that open-ear fittings use advanced active feedback cancellation algorithms to offset the risk of feedback. Presently, some active feedback cancellation algorithms may improve the available gain by 15 dB to 20 dB6 and bring the available gain at 3000 Hz to >40 dB in an open-ear fitting. This is similar to an effective vent diameter of less than 1 mm.
Caveat #3: Increased contribution from direct sounds. As the vent diameter increases, more sounds from the environment enter the ear canal directly through the vent. Indeed, a characteristic of an open-ear fitting is that the real-ear occluded response (REOR) with the hearing aid and earset in situ is the same as the real-ear unaided response (REUR). This means all sounds will enter the ear canal unaffected and any resonance effect (such as ear canal resonance at 2700 Hz) will be preserved. Thus, sounds at the eardrum may be dominated by different sources (processed or direct) depending on their relative levels:
- If the level of the processed sounds is at least 20 dB higher than that of the direct natural sounds (leaked through the vent), one can assume that the SPL at the eardrum is dominated by the processed sounds. The results of any processing achieved by the hearing aid will most likely be preserved. This is the case where the input level is low, such as with soft speech or in quiet environments or when the gain is high.
- If the level of the processed sounds is similar in magnitude to the natural sounds, the resulting SPL measured at the eardrum will be a combination of the natural sounds and processed sounds. Cancellation and reinforcement of sounds may occur depending on the phase relationship between the direct and processed sounds. This may result in unexpected dips and peaks in the measured real-ear aided response (REAR) during real-ear measurements. Sound quality may be affected. Strategies and algorithms designed to preserve the naturalness of the processed sounds (eg, Sound-Harmony, which adjusts for the lost low frequencies and potential phase cancellations) may be desirable in these cases.7
- If the level of the direct input sounds is substantially higher than the level of the processed sounds, the effect of any processing by the hearing aid may be “masked” by the level of the direct natural sounds. This could be the case in noisy situations where the level of the inputs is higher than the level of the processed sounds treated by the directional microphone and/or noise reduction algorithms. In these cases, the effectiveness of the directional microphone and noise reduction algorithm may be diminished. Indeed, Dillon8 has shown that the directivity index (DI) of a directional microphone decreases by almost 4-6 dB in the lower frequencies with a 3 mm vent diameter. On the other hand, the DI above 1000 Hz remains minimally affected. This may explain why studies evaluating the SNR advantage of a directional microphone in an open-ear fitting still show SNR improvements, albeit of a smaller magnitude (2-3 dB on average).7
The implication from the contribution of direct natural sounds is that sophisticated signal processing algorithms are even more necessary in an open-ear fitting than in an occluded-ear fitting for optimal hearing aid performance. Algorithms to minimize the cancellation effects from the direct sounds, as well as algorithms to preserve the SNR advantages of directional microphones and noise reduction, are needed to ensure satisfactory performance.
Who are the candidates for an open-ear fitting? Despite the freedom from the occlusion effect, open-ear fittings could limit the amount of available gain and compromise the effectiveness of the signal processing algorithms on the hearing aids. Thus, these devices may not be appropriate for all hearing-impaired wearers, especially those with more than a moderate degree of hearing loss.
|
Degree of hearing loss at 500 Hz (in dBHL) |
Recommended vent diameter (solid mold) |
|
< 20 dB |
open |
Table 1 provides an initial estimate of the optimal vent diameter for the average hearing-impaired person. In this estimation, the degree of hearing loss at 500 Hz is used as a guideline. It is assumed that a traditional solid earmold or ear-insert of the typical length (22 mm) is used. Use of a shorter earmold or of a hollow earmold will change the recommendations substantially. It should also be mentioned that, because the vent effect reduces the output of a hearing aid up to 2000 Hz, open-ear fittings may not be appropriate for those with more than 60 dBHL at 1000 Hz.
Other factors (ie, experience with amplification, size of ear canal, etc) should also be considered. In addition, hearing aids that do not have sophisticated processing algorithms may be less effective in an open-ear mode in preserving audibility and SNR than an occluded-ear fitting.
Standard-tube (#13) vs Thin-tube Fittings
The main advantage of using a thin tube (inner diameter of 0.8 mm) instead of the traditional #13 tube (inner diameter of 1.9 mm) is the cosmetic appeal of a thin tube. A thin-tube BTE is less visible and has increased patient acceptance.9

|
| FIGURE 3. Coupler output of an Inteo IN-9 hearing aid connected to a #13 tube compared to the same device connected to a thin-tube (0.8 mm inner diameter). Note the lower resonant frequency and the lower high frequency output with the thinner tubing (in red). |
The drawback of a thin tube is its reduced high-frequency output when compared to the standard #13 tube. This is illustrated in Figure 3, which shows the effect of replacing the #13 tubing (and earhook) with a thin-tube commonly used in open-ear fittings. Two observations are apparent. First, the tubing resonance that occurs at around 1000 Hz is shifted downwards to around 800 Hz. Second, a reduction in the hearing aid output by 5-10 dB is seen above 1000 Hz.
The changes in the output of the hearing aid (below the maximum power output or MPO) when using a thin-tube fitting may be offset by compensations made within today’s digital hearing aids such that a desirable output appropriate for the wearer may still be possible. Unfortunately, this compensation still leads to less available gain for the wearer. For those with a mild-to-moderate degree of hearing loss, the effect is transparent because sufficient gain is still attainable (despite the compensation). For someone with a more severe degree of hearing loss, the use of a thin tube could potentially limit the available high-frequency output.
Who are the candidates for a thin-tube fitting? One common misconception is that a thin-tube fitting is synonymous with an open-ear fitting. This may have been true initially when thin-tube open-ear fitting was first introduced. However, with the recognition of the cosmetic advantage of a thin-tube, many hearing aid and earmold manufacturers have made available occluding earmolds that use a thin-tube instead of the standard #13 tube. Thus, thin-tube fittings are available in both open-ear and occluded-ear fittings. Therefore, candidates for thin-tube fittings should be considered separately for open-ear and occluded-ear fittings.
Assuming that the BTE hearing aid has an MPO of around 120 dBSPL (typical of most BTE with a moderate output), a thin-tube open-ear fitting would be appropriate for those with less than 20-30 dBHL at 500 Hz and less than 60 dBHL at 1000 Hz. Candidates for a thin-tube occluded-ear fitting may be more restrictive than those with a standard #13 tube fitting because of the reduction in high-frequency output. In general, the upper limit of the hearing loss should not exceed 60-70 dBHL across frequencies for a thin-tube, occluded-ear fitting. In contrast, the upper limit would be 70-80 dBHL for a standard #13 tube occluded-ear fitting.
Hearing aids with only a mild output level (< 110 dBSPL) may pose difficulty for those with more than a moderate degree of hearing loss. The fitting range should be 10-20 dB less than that available with a moderate MPO (ie, 50-60 dBHL across frequencies).
Thin-wire vs Thin-tube
In this article, we have intentionally described RIC or RITE BTEs as “thin-wire hearing aids” in order to highlight the similarities/differences to a thin-tube hearing aid. Because the external diameter of the thin-tube is just slightly larger than that of the thin-wire, a thin-wire fitting and a thin-tube fitting are cosmetically similar. The differences between the two arise from the receiver in the wearer’s ear canal. The following examines the validity of some of the claims thought to be potential advantages of placing the receiver in the ear canal.
A smaller hearing aid? With the receiver outside the BTE case and inside the wearer’s ear canal, one would expect that the size of a RIC hearing aid to be smaller than a traditional BTE hearing aid. Indeed, this is the case for the majority of RIC hearing aids today. On the other hand, the size of today’s BTE hearing aids has been reduced substantially from those available in earlier days. An example is the newer micro-size thin-tube BTE hearing aids. Additionally, the elimination of components such as the telecoil, direct audio input capability, optional user controls (eg, VC or program switches), and the use of a smaller battery (size 312 or 10 vs size 13 or 675) often facilitated size reductions.10
Therefore, the assumption that a RIC hearing aid is smaller than a traditional BTE may not always be valid. This is especially the situation when RIC devices are compared to a micro-size thin-tube hearing aid.
To be even smaller than a micro-size hearing aid would require further miniaturization of the receiver, size reduction of the IC chip, and hearing aid case redesign (including component layout). For example, in our company’s case, these additional considerations enabled the recently introduced Passion PA-115 RIC to be about 30% smaller than the micro-size m-model BTEs.
A broader bandwidth? One of the much-discussed comments about RIC hearing aids is that they have a broader bandwidth. The validity of that statement is dependent on the reference to which the RIC hearing aid is compared. It may be true if the comparison is made to other hearing aid styles made by the same manufacturer. This is a direct result of improvement in receiver technology; in general, receivers that are more recently introduced have a broader bandwidth.
On the other hand, the statement may be less valid if one compares bandwidths among manufacturers. Table 2 summarizes the bandwidths of various hearing aid models and styles made by several manufacturers. One can see that, within a manufacturer, the bandwidth of the RIC product is typically broader than its other products. However, one can also see that RIC devices made by a particular manufacturer (eg, #3) may not compare well to the products made by another manufacturer (eg, #2-A, #5-C). Therefore, one should not automatically assume that RIC hearing aids have a broader bandwidth.

|
| TABLE 2. Frequency responses of various hearing aid models from selected manufacturers. It is unwise to assume that each BTE type offers the same broadband responses across manufacturers. |
How did these assumptions about a broader bandwidth arise? Previously, it was shown in Figure 3 that a thin-tube fitting reduces the high-frequency output of a hearing aid (compared to a #13 tube). As indicated, the narrower the tubing, the more restrictive the bandwidth. Thus, if one were to take the output of a hearing aid receiver directly (ie, without going through earhooks and earmolds), as in a RIC or a custom product, a bandwidth that is broader than the standard configuration should be achievable. Right?

|
| FIGURE 4. Differences in output between the ED receiver configured as a BTE and the same receiver configured as an ITE hearing aid. The bandwidth of the receiver, when tested as an ITE (to simulate a RIC), does not become broader than when tested as a BTE, and earhook/tubing resonance typically seen at 1000 Hz, 3000 Hz, and 5000 Hz is replaced by a smaller resonance peak. |
This is only partly true. Figure 4 shows the frequency-output response of a Knowles ED hearing aid receiver tested in a BTE case and in an ITE case (using the same chip and amplifier setting). Differences in the measured output of the two hearing aid styles are the results of the different acoustic modifications resulting from the earhook and tubing used in the BTE (in black) and the ITE hearing aids (in red). Comparing the two outputs, one immediately recognizes that the bandwidth of the ED receiver, when tested as an ITE hearing aid (ie, to simulate a thin-wire RIC hearing aid), is not broader than when it is tested as a BTE, which is the intended use of this receiver type.
This suggests that simply using a BTE receiver in a thin-wire configuration may not extend the bandwidth of the hearing aid. Other factors would also affect the output bandwidth of the hearing aid.
Figure 4 also shows another important characteristic of a RIC hearing aid. When used without an earhook or an earmold tubing (such as in a custom product or in a RIC), earhook/tubing resonance that is typically seen in a BTE at 1000 Hz, 3000 Hz, and 5000 Hz disappears. Rather, the resonance peaks are replaced by a much smaller resonance peak at around 2500 Hz (the specific frequency being determined by the small receiver tubing used in the ITE). One also sees that the frequency response curve of the ITE is smoother. But, most importantly, one should recognize that the output around 1000 Hz (and its odd harmonics) is significantly lowered. For example, the output around 1000 Hz is reduced by 13 dB from 128 dB to around 115 dB! For wearers whose hearing losses are at the upper limit of the fitting range around these frequencies, a RIC fitting (rather than a traditional BTE) fitting may yield insufficient output.
On the other hand, if one were to compare the frequency response of a thin-wire RIC hearing aid to its equivalent thin-tube hearing aid (using the same receiver), it is likely that the frequency response of the thin-wire RIC hearing aid is broader than that of the thin-tube hearing aid. And, with the use of newer receiver designs, it is possible that some newer RIC hearing aids have a broader frequency bandwidth. A broader bandwidth would provide a richer and clearer sound quality than a more restricted bandwidth.
The broader bandwidth does not necessarily mean that every hearing-impaired person may benefit from it. Despite the improvement in receiver technology, many of the receivers that have an extended bandwidth also have a limited MPO (eg, below 110 dBSPL). Thus, the applicability of the extended bandwidth may be restricted to mild-to-moderate hearing losses. People with a more severe loss may not receive sufficient output.
Consequently, there is no guarantee that a RIC hearing aid implies a broader bandwidth. A receiver that is especially made to have a broader bandwidth has to be specifically designed for the RIC device. The bottom line: each thin-wire RIC needs to be judged on its own merits.
More gain before feedback? There is a substantial separation between the microphone and the receiver of the thin-wire hearing aid when the receiver is in the wearer’s ear canal. It is intuitive to assume that this increased separation would reduce the likelihood of feedback. Indeed, this is true if one compares the available gain of a BTE to an ITE or CIC using the same hearing aid components.8
On the other hand, there is no reason to suspect that a RIC hearing aid yields more available gain before feedback than a traditional or a micro-size BTE hearing aid. This is because the distance between the bore opening of the earmold and the microphone in a traditional BTE is similar to the distance between the receiver opening and the microphone of a RIC. Indeed, if the receiver in the RIC has a broader bandwidth than the traditional BTE, its likelihood of feedback may be even higher, leading to less available gain.
Additionally, today’s technology affects the validity of the idea that RIC hearing aids yield higher available gain before feedback. With the advances in DSP technology, it is possible to achieve 15-20 dB more available gain before feedback in today’s hearing aids using active feedback cancellation algorithms.6 A custom product with an active feedback cancellation algorithm may yield more available gain than a RIC hearing aid that may not have such an algorithm or have a feedback algorithm that may be less effective.
A wider fitting range? Because the available gain before feedback in a RIC hearing aid is not necessarily higher than that of a traditional BTE (or thin-tube BTE), for the reasons stated earlier, one should not expect a RIC hearing aid to fit a more severe hearing loss than its electroacoustic specification would indicate.
Fitting range is dependent on many variables. One important variable is the receiver of the hearing aid, because it directly affects the MPO and the bandwidth of the amplified sounds. In general, the larger the receiver (in physical size), the higher the MPO and the greater the fitting range. On the other hand, since the receiver of a RIC hearing aid is placed in the ear canal of the wearer, and the battery used in such an application must be small (eg, size 312 or 10) to fit into a micro-size case, the MPO of the RIC seldom exceeds 120-125 dBSPL (and the typical value is below 110 dB SPL). Consequently, the claim that a thin-wire hearing aid increases the fitting range to include more severe hearing losses may not always be true. Indeed, if the RIC hearing aid uses a small receiver (MPO less than 110 dB SPL) in order to provide an open-ear fitting option, its fitting range will be more limited than a traditional BTE hearing aid that uses a larger receiver.
Another contention is that, since a RIC hearing aid is inserted deeper into the ear canal than a traditional fitting, this reduces the volume of the residual ear canal and effectively increases the SPL measured at the eardrum. While this may be true, there is no reason why a thin-tube micro-size BTE hearing aid or a traditional size BTE cannot have the earmold inserted deeper into the ear canal to achieve the same increase in SPL. Thus, the use of a RIC in and of itself does not necessarily increase the fitting range. But one should recognize the manufacturers’ recommendations of the insertion depth of the RIC hearing aid in order to achieve the desired output.
Additional considerations for a thin-wire RIC hearing aid:
- Because the receiver of a RIC hearing aid is inside the ear canal, exposure of the receiver to moisture and cerumen is significantly increased over that of the traditional BTE (including thin-tube) fittings. Care should be exercised in the cleaning of the receiver-encased earsets/earmolds so the hearing aid receivers are not damaged.
- The stability/reliability of the RIC electrical wire in making good contact between the hearing aid amplifier and the receiver may be a consideration. Frequent removal of the wire from its connection and accumulation of moisture/debris could weaken the contact and create intermittence and distortion. Thus, wearers of a thin-wire RIC hearing aid should exercise caution when handling and caring for their hearing aids.
One advantage of RIC designs that use a modular concept (eg, Passion PA-115) is that the receivers can be easily snapped in/out by the clinicians. Thus, repair of RIC hearing aids can be achieved at the clinician’s site conveniently.
Who are the candidates for thin-wire RIC hearing aids? Similar to thin-tube hearing aids, thin-wire RIC hearing aids can be fit in an open-ear fitting or an occluded-ear fitting. In addition, both classes of hearing aids are equal in their cosmetic appeal. Because a thin-wire RIC may be reduced in size further from a thin-tube hearing aid that has the same components and features, it may offer a slight cosmetic advantage over the thin-tube hearing aids. This, of course, ignores the design of the BTE hearing aid case, which is also an important determinant of the cosmetic appeal of the hearing aid.
From an electroacoustics standpoint, a thin-wire hearing aid has the potential of a smoother frequency response and a broader bandwidth (depending on manufacturer) than a thin-tube hearing aid. Thus, some may offer better sound quality than a thin-tube hearing aid to wearers with a mild-to-moderate degree of hearing loss.
Assuming that the RIC hearing aid has a peak MPO of around 110 dBSPL (typical of most RIC with mild-to-moderate output), a thin-wire RIC open-ear fitting would be appropriate for those with less than 20-30 dBHL at 500 Hz and less than 50-60 dBHL at 1000 Hz. Candidates for a thin-wire RIC occluded-ear fitting may be restricted to those with less than 60-70 dB hearing loss across frequencies. This restriction in fitting range is a direct result of the limited MPO in many RIC hearing aids.
For a more moderate-to-severe degree of hearing loss, the typically higher MPO and the presence of tubing resonance in a thin-tube hearing aid may be more desirable than a RIC fitting. Of course, as repeatedly mentioned in the previous discussions, such a recommendation is based on the assumption of the typical RIC and thin-tube hearing aid. Variations among manufacturers/products could invalidate such a recommendation. It is imperative that clinicians are familiar with the electroacoustic specifications of the specific RIC hearing aid, and not categorically assume that one class of hearing aid is more appropriate than the other.
Conclusions
Despite the significant variations in how today’s BTEs are configured, it is important to recognize that all the different variations can be traced back to two independent dimensions: the amount of ear-canal occlusion (“open vs closed”) and the diameter of the ear-piece tubing. Understanding the differences among the various configurations allows clinicians to select the best cosmetic and functional hearing aid option for the wearers.
Correspondence can be addressed to or Francis Kuk, PhD, at .