Volume controls (VC) have been a feature of hearing instruments from their inception. Until the mid-1970s, most hearing instrument manufacturers made their own VCs. When component manufacturers began offering VCs, however, these components were quickly outsourced. Today, component manufacturers produce the vast majority of VCs.
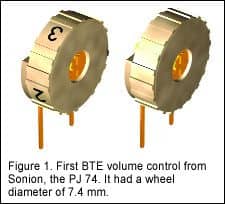
The first VCs supplied by component manufacturers were for behind-the-ear (BTE) hearing instruments. They were large, featuring a wheel diameter of 7 mm or wider (Figure 1). Smaller VCs were developed as hearing aid manufacturers began to develop more discreet devices to cope with stigma issues.
|

|
In the mid-70s, when ITE hearing aids finally became small enough to be situated in-the-ear (prior to this time, they were more aptly described as “out-of-the-ear” hearing aids), their popularity grew quickly. Volume controls for these new ITEs were significantly smaller (Figure 2). As with BTEs, manufacturers’ drive for tinier, more discreet ITE devices called for smaller VCs, and the housing sizes of most VCs were reduced to below 4 mm.
Market Development
The idea of automatic gain control (AGC) goes back at least to the late 1930s and vacuum-tube hearing aids.1 AGC has reduced the need for the VC to be frequently adjusted by the user. However, it was only with the implementation of more advanced forms of AGC—like wideband dynamic range compression (WDRC)—that manufacturers could confidently claim that the “automatic” hearing aid was good enough to reduce user reliance on VCs.
In view of the history of AGC development, one might think that the market for VCs has declined rapidly. However, the percentage of hearing aids with VCs decreased much more slowly than would be predicted. Prior to 1994, almost all (98%) ITE hearing aids had VCs; in 2001, three-quarters (75%) of ITE hearing aids still had VCs.2 The recent HR Dispenser Survey (June 2006 HR) indicates that 57% of all US hearing aids contain a VC, while MarkeTrak VII shows 69% have them. The main reasons for this include:
• It gives the user a sense of control;
• It can compensate for sound environments that are not predicted by the signal processing algorithms implemented, even in today’s DSP-based devices;
• It allows the user to decide how much or how little he/she actually wants to hear in a given situation;
• It allows rapid (albeit manual) changes in the gain setting.
• It is a habit from wearing previous aids.
In MarkeTrak VI,2 Kochkin concludes that about one-third of all hearing aid users need a VC or similar device (eg, remote control) to manipulate gain. The study by Surr et al.3 shows that 77% of experienced users desire a VC, even if the majority of them used it only occasionally.
In July, The Hearing Review published an article by Meredith4 who concluded that, when given a choice, 60% of new hearing instrument users and 89% of experienced users prefer to have a volume control. This suggests that preference for a volume control has not changed appreciably in the 5 years between the two studies.3,4 Furthermore, Meredith4 used subjects with mild to moderate hearing losses. Thus, this data contradicts the common belief that the need for a VC increases with severity of hearing loss—and the reduced dynamic range of the user and/or high demands on the processing power of the hearing aid.
Basic Function of a VC
The role of the VC has always been to adjust the gain setting of the hearing aid. For analog aids this was done as an integrated part of the feedback loop of the amplifier. For digital instruments, the VC is coupled as a voltage divider, with the output voltage determining the digital signal processor (DSP) amplification. The range of attenuation was previously up to 40-50 dB. With today’s better DSP algorithms, this is often configurable in the fitting software (eg, a range of 10-30 dB), allowing for more precise adjustments due to the smaller gain span.
Two Types of VCs
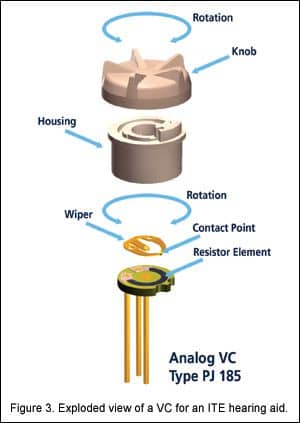
Analog VCs have a resistor element on which a “wiper” travels as the VC is rotated (Figure 3). The wiper makes contact with the resistor element at a point that is determined by the knob position. The contact point divides the resistance element in two parts.
|
|
The length ratio of these two parts is used by the digital aid’s analog-to-digital (A/D) converter to determine the gain. An A/D converter is not necessary with digital VCs, as they will accept the digital output directly.
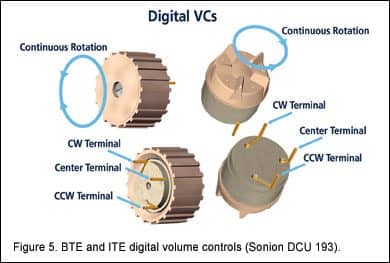
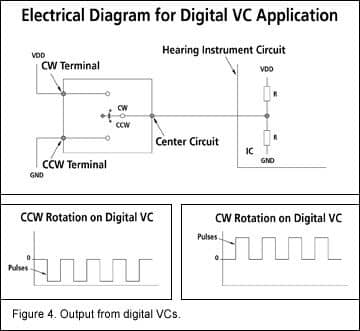
Digital VCs generate output pulses as the VC is rotated (Figures 4-5). Depending on the rotational direction—clockwise or counter-clockwise—the pulses will be present from the center terminal to one of two outer terminals. No pulses are generated when the VC is stationary. When the hearing aid is turned on, the VC does not indicate what gain setting should be used. Instead, the gain is defined during the fitting session as the “wake-up setting.” In some hearing aids that employ datalogging, this gain setting can change over time and can be controlled by the actual behavior of the user.
Thus, the main advantage of a digital VC is that there is less fiddling with the hearing aid by the user. For hearing aid manufacturers, digital VCs have another advantage: It is not necessary to have both left and right versions for ITEs. Instead, the fitting software tells the aid which of the clockwise or counter-clockwise output pulses should be used for “Up” and “Down” adjustments. This reduces the stock-keeping units (SKU) by 50%.
Continuous Rotation and On/Off Switches
One of the most important differences between analog and digital VCs is that there is no end stop on digital VCs. The easiest way to explain why is to imagine the opposite situation: If the digital VC had an end stop, and the VC was turned fully up when the hearing aid was shut off, it would not be possible to increase the gain further (ie, from the pre-defined wake-up setting) the next time the aid was turned on. To do so, it would be necessary to place the VC in mid-position, shut off the instrument, and then turn it on again.
Since there is no end stop, there can be no on/off switch on the digital VC. This is considered to be a disadvantage by some ITE users. For BTE volume controls, the situation is different. The requirements and guidelines for hearing aids issued by the “Nordic Cooperation on Disability” state that: “On behind-the-ear models and body-worn models the gain control should not be combined with the main switch.” Since many hearing aid manufacturers need to compete in the Nordic market, they choose to comply with the requirements—meaning that the on/off switch is located separately.
Conclusion
What is the future for VCs? To paraphrase Mark Twain: Rumors of the death of VCs are greatly exaggerated. For the reasons mentioned above, hearing aids will still offer a VC option. As signal processing algorithms continue to improve, it is clear that the future for VCs greatly depends on the component manufacturers. Their ability to come up with innovative solutions to the challenges of small size requirements and ease of operation will determine the success of VCs. The newer thin-tube, open-fitting and receiver-in-the-ear BTEs call for smaller VCs. For ITEs, combining functions in an easy-to-operate manner can be a way to provide better user satisfaction.
References
1. Lybarger SF. A historical overview. In: Sandlin RE, ed. Handbook of Hearing Aid Amplification, Vol 1. San Diego: Singular Publishing Group Inc; 1995.
2. Kochkin S. MarkeTrak VI: Isolating the impact of the volume control on customer satisfaction. The Hearing Review. 2003;10(1):26-35.
3. Surr RK, Cord MT, Walden BE. Response of hearing aid wearers to the absence of a user-operated volume control. Hear Jour. 2001;54(4):32-36.
4. Meredith R. Volume control preferences with WDRC digital hearing aids. The Hearing Review. 2006;13(7):24-28.
This article was submitted to HR by Morten Wagner, BSEE, product manager for Electromechanical Components at Sonion A/S, Roskilde, Denmark. Correspondence can be addressed to HR or Morten Wagner, Sonion Roskilde A/S, Byleddet 12-14, DK-4000, Roskilde, Denmark.