Expert Roundtable | September 2015 Hearing Review
Note: This is the fifth article in a seven-part special Expert Roundtable series published in the September 2015 edition of The Hearing Review, guest-edited by Douglas Beck, AuD. For all the articles in this Expert Roundtable, click here.
Chapter 5: Lower cognitive function may be a risk factor for lower satisfaction with hearing aids
It appears likely that patients with lower cognitive function would benefit from a longer period of counseling, education, and training on topics such as expectations for hearing rehabilitation, hearing aid care, and use of hearing aids, including manual adjustments and battery changes.
With the escalation of audiology-related research in cognition, audiologists have begun to wonder if understanding a patient’s cognitive ability would offer a meaningful contribution to the development of an individualized treatment plan. This is a reasonable curiosity and one toward which we have gained some insight.
Between our research centers in Minneapolis and Berkeley, Calif, we maintain an active database of almost 1,200 volunteer research participants with hearing loss. At the time of qualification for research participation, all volunteers complete a battery of assessments, the results of which are logged in the database. One component of the qualification is the Montreal Cognitive Assessment (MoCA).1 The MoCA is a 13-item screening tool which can be administered in 10 minutes; it is available as a one-page document and is designed to measure cognitive abilities including attention, memory, language, and visuo-spatial functions. The MoCA has a maximum score of 30. Scores above 26 are considered to be within the normal range; scores below 26 indicate the possibility of cognitive impairment, and scores below 22 indicate the possibility of more significant cognitive impairment. (See www.MoCAtest.org for details.)

Jason Galster, PhD
We completed a retrospective analysis of relationships among a variety of participant and hearing aid factors and global scores on the MoCA. Some examples of the assessed factors are age, gender, high-frequency pure-tone average (PTA), aided Hearing-in-Noise Test (HINT) performance, and overall satisfaction with hearing aids. Some of these relationships will be discussed here.
The participant sample included 61 adults with hearing loss, who had recently completed a multi-week hearing aid field trial. For this reason, subjective and objective hearing aid outcomes reflect participants’ experience with a single hearing aid type, whereas the physical hearing aid style and ear-coupling configuration varied across participants. Ages ranged from 55 to 84 years. For the purpose of analysis, participants were grouped into proportionally distributed age quartiles.
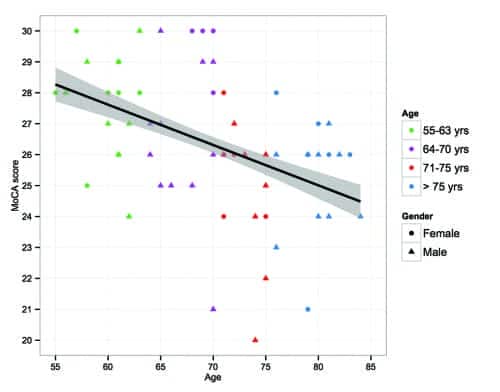
Figure 1. MoCA scores are shown as a function of participant age, with each of the four age groups represented by different colors and gender represented by different symbols. Box plots show quartile distributions around the mean. A linear regression of MoCA score and age is also plotted.
Figure 1 shows a scatterplot of participants’ MoCA scores plotted as a function of age. Individual colors represent each of four age quartiles; gender is shown as symbol type. The fitted line shows a linear regression between the two variables. The linear regression model indicates that age accounts for approximately 25% of variance in the MoCA scores. This is an important observation as it reinforces the expectation that age is a dominant factor in participants’ cognitive abilities.
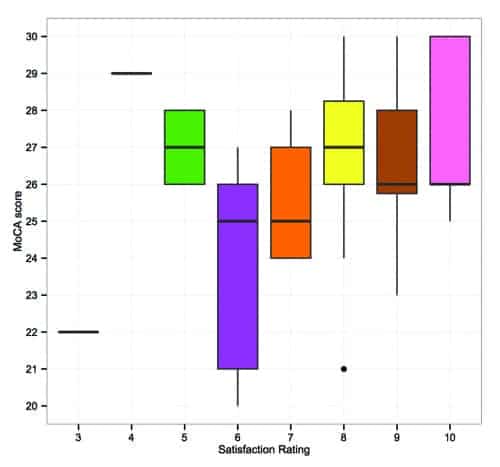
Figure 2. MoCA scores are shown as a function of overall hearing aid satisfaction. Boxplots show quartile distributions around the mean.
Figure 2 shows participants’ satisfaction with their hearing aids plotted as a function of MoCA score. Satisfaction ratings were recorded on a scale of 1 to 10, in response to the item “Please rate your overall satisfaction with the hearing aids.” Satisfaction rating correlated positively with MoCA score (p<0.05), indicating that participants with higher cognitive ability reported greater satisfaction with their hearing aids.
The relationship between hearing aid satisfaction and cognitive ability is perhaps one of the most intriguing results of this study. This relationship suggests that patients with lower levels of cognitive functioning may be at greater risk for poor satisfaction with and possible rejection of their hearing aids. We do not yet have validated recommendations for modifying a clinical routine to meet the needs of a patient with lower cognitive ability, as these results warrant further investigation. However, it is likely these patients would benefit from a longer period of counseling, education, and training on topics such as expectations for hearing rehabilitation, hearing aid care, and use of hearing aids, including manual adjustments and battery changes.
The results of this study, including analyses not reported here, indicate that the MoCA is sensitive to a variety of demographic and audiologic factors. However, this does not suggest that the MoCA should be used as part of an audiologic assessment. Reliance on this screening tool is impacted by the auditory interaction between administrator and patient, and has been shown to introduce bias and yield inaccurate outcomes.2 Based on these observations, the inclusion of cognitive assessment in future audiologic outcome measures may provide insight that could be leveraged to better develop individualized treatment plans.
Acknowledgements
Thanks to Elizabeth Galster, Amanda Wolfe, Alyson Gruhlke, and Ryan Irey. These findings were originally presented at the 2015 American Auditory Society meeting in Scottsdale, Ariz.
References
-
Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J Am Geriatrics Soc. 2005;53:695- 699.
-
Dupuis K, Pichora-Fuller K, Chasteen AL, Marchuk V, Singh G, Smith SL. Effects of hearing and vision impairments on the Montreal Cognitive Assessment. Aging Neuropsychol Cognition. 2014;17:1-25.
Jason Galster, PhD, is senior manager of audiology research at Starkey Hearing Technologies, Eden Prairie, Minn.
Correspondence can be addressed to HR or Dr Galster at [email protected]
Original citation for this article: Galster J. Expert Roundtable, Chapter 5: Lower cognitive function may be a risk factor for lower satisfaction with hearing aids. Hearing Review. 2015;22(9):20.
This article is one of seven chapters in a series of articles that review the key points addressed during the 2015 AudiologyNOW! session titled “Issues, Advances, and Considerations in Cognition and Amplification.” Follow the links to related chapters by Douglas L. Beck, PhD, Brent Edwards, PhD, Christian Füllgrabe, PhD, Gabrielle Saunders, PhD, Andrea Pittman, PhD, and Gurjit Singh, PhD.