Special Issue: Sudden Sensorineural Hearing Loss | December 2003 Hearing Review
Articles in this Special Edition:
- Sudden Hearing Loss: Unique Challenges and Opportunities. An introduction by Maurice H. Miller, PhD, guest editor
- Etiologies and Treatment Options for Sudden Sensorineural Hearing Loss, by Jose N. Fayad, MD, and Antonio De La Cruz, MD
- The Diagnostic and Treatment Dilemma of Sudden Sensorineural Hearing Loss, by Jack J. Wazen, MD, FACS, and Soha N. Ghossaini, MD
- Sudden Hearing Loss: A Team Approach to Assessment, Treatment, and Rehabilitation, by Michael H. Fritsch, MD, Allan O. Diefendorf, PhD, and Michael K. Wynne, PhD
- Steroid Therapy for Sudden Sensorineural Hearing Loss, by Chris Halpin, PhD, and Steven D. Rauch, MD
- Rehabilitative Aspects of ISSNHL, by Maurice H. Miller, PhD, and Jerome D. Schein, PhD
By Chris Halpin, PhD, and Steven D. Rauch, MD
Sudden Sensorineural Hearing Loss (SSNHL) is one of the few sensorineural losses known to be reversible. In cases where such an outcome is possible, there appears to be a time window of no more than 2-4 weeks from onset of deafness during which treatment must be started to be effective. Further, there is a range of outcomes, including some untreated cases where spontaneous recovery is seen and some treated cases that do not respond at all. Because of the possibility of improved outcome with steroids, and the narrow window of opportunity for initiating treatment, SSNHL should be considered an emergency of the ear.
Related article: Sudden Sensorineural Hearing Loss (SSNHL): A Status Report 2022, by Douglas Beck, AuD, and Jed Grisel, MD
Sudden Sensorineural Hearing Loss (SSNHL) is one of the few sensorineural losses known to be reversible in some cases. The chance to improve hearing with the application of steroids can be very rewarding for an otolaryngologist and audiologist, and this depends upon early diagnosis of the cases where such an outcome is possible. SSNHL is characterized by new-onset unilateral sensorineural hearing loss that develops within 72 hours. It is very often accompanied by a feeling of fullness and, occasionally, by tinnitus and vertigo.1 Audiologic evaluation establishing a sensory rather than a conductive pathology is critical to the diagnosis.
In a recent 10-year retrospective study2 of 318 patients, 88% had little or no pre-existing hearing loss on the contralateral side and, as a result, were not previously under the care of an audiologist or otolaryngologist. In these cases, the initial symptoms were often a combination of hearing loss and a pronounced “blocked” sensation that frequently led primary care physicians to a mistaken preliminary diagnosis of otitis media. Ultimately audiologic evaluation demonstrating elevated bone conduction thresholds and normal tympanometry is needed to establish the correct diagnosis.
Once referred to an otolaryngologist, such cases may benefit from the application of steroids (typically Prednisone) for several weeks. There are two important factors regarding this treatment. First, there appears to be a time window of no more than 2-4 weeks from onset of deafness during which treatment must be started to be effective. Second, there is a range of outcomes, including some untreated cases where spontaneous recovery is seen and some treated cases that do not respond at all.
Even though outcome is variable, the 10-year study noted above showed a significant benefit to the use of steroids for SSNHL.2 Because of the possibility of improved outcome with steroids, and the narrow window of opportunity for initiating treatment, SSNHL should be considered an emergency of the ear.
The Cochlear Mechanism
SSNHL has an estimated incidence between 5 and 20 per 100,000 persons per year.3 This is approximately the same incidence as Meniere’s syndrome (15 per 100,000) and an order of magnitude more common than acoustic neuroma (1 per 100,000).4 Several mechanisms in the cochlea have been put forward as the cause of SSNHL. The primary candidates are vascular problems and viral infections.
Vascular insufficiencies were proposed by several authors, based primarily on the brief time course of the onset, as if blood supply to the cochlea had been interrupted. There have also been reports of SSNHL or similar losses in patients with known disorders of the vascular system.3 On the other hand, treatment with vasodilators has not been shown to be effective.5 Also, histopathologic examination of postmortem human temporal bones from patients with SSNHL does not show new growth of bone in the cochlea (labyrinthitis ossificans), as is seen in cases where there was clear vascular interruption.6
Several authors have shown an association of SSNHL with active viral upper respiratory illness. Patients with SSNHL have also been shown to have antibodies to certain viruses.7 Postmortem examination of SSNHL temporal bones have shown atrophy of the organ of Corti, spiral ganglion, and tectorial membrane, with relatively good preservation of spiral ganglion cells. These findings are consistent with viral disease.6 Animal experiments have clearly demonstrated the mechanisms of virus penetration of the inner ear.8
On the other hand, it is not necessary for infection of the cochlea itself to occur in order to provide a viral-based mechanism for SSNHL. Adams9 has shown that bio-molecules known as inflammatory cytokines are produced in the cochlea as a response to viral disease in the upper respiratory tract. These molecules may interrupt the gap junction ion pathways in the cochlea. Gap junctions function as gates between the supporting cells in the cochlea, allowing the proper ions to be transported to maintain the fluid “battery” necessary for normal hearing. Besides this function, gap junctions transport other necessary chemicals and so, if this system is stopped, the result is expected to be a sudden decrease of sensorineural function, and eventual death of hair cells. Adams has also shown that early introduction of steroids will effectively reverse this process.
Although corticosteroids are known to cause a host of side-effects, the vast majority of these are dose-related. Therefore, they are unlikely to occur during the relatively short “burst and taper” treatment used for SSNHL. The two corticosteroid side-effects most likely to be seen during SSNHL treatment are gastritis/stomach irritation and blood sugar elevation. The latter is generally only seen in diabetic patients, but it is prudent to alert the patient’s primary care physician to the treatment plan so he/she can monitor blood sugar throughout. Stomach problems are generally only seen during the early phase of treatment when steroid dose is higher, and it can often be avoided by giving the medication with a meal. Stomach problems can also be prevented by antacids and other over-the-counter drugs used for ulcers and reflux.
Audiologic Evaluation and Results
A unilateral loss of practically any audiogram type can develop suddenly and present in the audiology clinic or practice. Not all of these should be considered reversible SSNHL. In the retrospective study by Chen et al.,2 a large number of flat losses were found (37%), but both high (6%) and low frequency (12%) steeply sloping losses were also seen. Twenty-three percent of cases reported profound loss on the affected side. As is usually the case, there was also a good number of audiograms (22%) which did not neatly fall into a single category.
The low frequency category was given special consideration since low frequency sensorineural loss can be a symptom of Meniere’s syndrome. In Meniere’s syndrome, fluctuations in low frequency hearing can occur in the same timeframe as in SSNHL. In the Chen et al.2 study, low frequency cases were excluded in order to prevent any mixing of the SSNHL and Meniere’s etiologies. In clinical practice, a similar caution is in order, requiring careful follow-up by an otolaryngologist and audiologist to establish a clearer picture of the disease. If Meniere’s syndrome emerges as the diagnosis, steroid therapy is unlikely to be effective.10
On the other hand, when sudden, unilateral sensorineural loss first presents, it may be impossible to know if it is SSNHL or Meniere’s syndrome. It is prudent to err on the side of treating the potential emergency condition, SSNHL, with a tapering course of oral steroids. If the the ear goes on to fluctuate and cause vertigo attacks, the Meniere’s diagnosis will eventually become apparent.

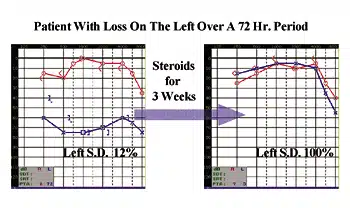
Figure 1. Audiograms taken one month apart showing the reversal of SSNHL after a course of steroid medication. This patient presented at the clinic complaining of both hearing loss and a “blocked” sensation on the left ear during the previous week.
Figure 1 shows the result of audiologic evaluations done when the patient first presented and then 1 month later after receiving a standard 3-week course of steroids. The medication is given with a “blast and taper” approach in which a large dose (for example, Prednisone 60mg/day) is given for the first few days, and then systematically tapered to lower and lower doses. This approach minimizes possible side-effects.
Any improvement should be well established by about 1 month after treatment begins. Thus, a follow-up audiologic evaluation should be done at that time. Most authorities advocate testing hearing again at 6 months and 1 year after treatment to confirm that recovery is stable and assure that no other problems have arisen in the contralateral ear. Bone conduction with masking and word recognition testing are essential in order to evaluate the sensorineural nature of the disorder and the improvement, if any. These losses are not associated with any middle ear involvement and so tympanometry and clinical otologic examination should be normal. As can be seen in the case in Figure 1, both initial decreases and then improvements are expected for speech discrimination as well. As always, a full 50-item standard list (ie, CID W-22), presented via compact disk is the minimum for effective assessment of changes in speech intelligibility over time.
While Figure 1 shows an example of good improvement, not all cases have the same outcome. Nearly 40% of steroid-treated cases did not recover at all, or the hearing worsened over the treatment period and these hearing losses remained permanent. In the other 60% of cases, the steroid-treated group improved by an average of 29 dB PTA (500 Hz, 1000 Hz, 2000 Hz and 4000 Hz). This was a better outcome than seen in the untreated cases, where a spontaneous improvement mean of 11 dB PTA was seen. Prompt steroid treatment also resulted in better recovery of word recognition scores. Speech intelligibility improved in both treated and untreated groups, but a significantly larger number of patients improved among those receiving steroids.
It is unethical in clinical research to withhold treatment of proven effectiveness. In the retrospective study of Chen et al,2 52 patients declined treatment or had medical contraindications to the steroid therapy. This cohort of subjects provides an opportunity to study the natural history of the disorder. In this group, as in the steroid-treated group, 40% of cases showed no recovery. Of those who did improve, a large range was seen, with a few cases even showing a large spontaneous recovery. Overall, however, the steroid-treated group showed larger improvements than the spontaneous improvements in the untreated group. The retrospective study showed that, while about 40% of each group failed to improve, in those cases where some recovery did occur, steroids seemed to assist the natural healing process resulting in larger hearing improvements.
The Future
Some studies have been undertaken to evaluate the benefit of antiviral drugs in combination with steroids for treatment of SSNHL. To date, none have shown efficacy above steroid treatment alone.11,12 While steroids themselves are likely to remain the medication of choice for SSNHL, there is an emerging new delivery system which may prove to be beneficial. Instead of tablets taken orally, the medication can be injected through the anesthetized tympanic membrane and will diffuse through the round window directly into the cochlea. This is known as Intra-Tympanic (IT) application. The possible advantage of IT administration is that it delivers a relatively high drug dose directly to the ear, thereby lowering the risk of systemic side-effects associated with oral steroids. Research is underway to study whether IT steroids are as good or better than oral steroids, and whether the side effects are actually reduced. Until this research is complete, a tapering course of oral steroids remains the standard of care for SSNHL.
There is no question that early diagnosis and treatment are needed in order to get the best outcome for patients with SSNHL. Every effort must be made to spread the word about this condition to primary care physicians and other primary care providers so they will make prompt referrals to audiologists and otolaryngologists who can initiate appropriate evaluation and treatment.
| Chris Halpin, PhD, is a clinical associate in audiology at the Massachusetts Eye and Ear Infirmary in Boston, and is assistant professor of Otology and Laryngology at Harvard Medical School. Steven D. Rauch, MD, is a surgeon in otolaryngology at Massachusetts Eye and Ear Infirmary and is associate professor of Otology and Laryngology at Harvard Medical School. |
References
1. Mattox D, Simmons F. Natural history of sudden sensorineural hearing loss. Ann Otol Rhinol Laryngol. 1977;86:463-80.
2. Chen C, Halpin C, Rauch S. Oral steroid treatment for sudden sensorineural hearing loss: a ten year retrospective analysis. Oto Neurotol. 2003;24:728-733.
3. Byl F. Sudden hearing loss: eight years’ experience and suggested prognostic table. Laryngoscope. 1984;94:647-61.
4. National Institutes of Health. Found at: www.nidcd.nih.gov. Accessed Nov 18, 2003.
5. Cinamon U, Bendet E, Kronenberg J. Steroids, carbogen or placebo for sudden hearing loss: a prospective double-blind study. Eur Arch Otorhinolaryngol. 2001;258:477-80.
6. Schuknecht H, Kimura R, Naufal P. The pathology of sudden deafness. Acta Otolaryngol. 1973;76:75-97.
7. Wilson W. The relationship of the herpesvirus family to sudden hearing loss: a prospective clinical study and literature review. Laryngoscope. 1986;96:870-877.
8. Woolf NK, et al. Hearing loss in experimental cytomegalovirus infection of the guinea pig inner ear: prevention by systemic immunity. Ann Otol Rhinol Laryngol. 1985;94:350-6.
9. Adams J. Clinical implications of inflammatory cytokines in the cochlea: a technical note. Otol Neurotol. 2002;23:316-322.
10. Silverstein H, et al. Dexamethazone inner ear perfusion for the treatment of Meniere’s disease: a prospective, double blind crossover trial. Am J Otol. 1998;19:196-201.
11. Stokroos RJ, et al. Antiviral treatment of idiopathic sudden sensorineural hearing loss: a prospective, randomized, double-blind clinical trial. Acta Otolaryngol. 1998;118:488-95.
12. Tucci DL, et al. Treatment of sudden sensorineural hearing loss with systemic steroids and valacyclovir. Otol Neurotol. 2002;23:301-308.
Correspondence can be addressed to HR or Chris Halpin, PhD, Department of Audiology, Massachusetts Eye and Ear Infirmary, Boston MA 02114; email: [email protected].
Original citation: Halpin C, Rauch SD. Steroid therapy for sudden sensorineural hearing loss. Hearing Review. 2003;10(13)[Dec]:32-35.