Research | March 2022 Hearing Review
A review of research on SSNHL incidence, etiology, diagnosis, treatment, and results
By Douglas L. Beck, AuD, and Jedidiah J. Grisel, MD
SSNHL remains a difficult problem to diagnose, manage, and resolve. Although treatments for SSNHL include corticosteroids and hyperbaric oxygen therapy (preferably early after onset), there are no interventions with highly predictable successful outcomes. However, a variety of new therapeutic strategies are under investigation.
Despite decades of research, Sudden Sensorineural Hearing Loss (SSNHL) remains an enigma in many respects. SSNHL is a distressing symptom for patients which may or may not be associated with tinnitus and/or vertigo. The diagnostic term SSNHL is often used interchangeably with Idiopathic Sudden Sensorineural Hearing Loss (ISSNHL) because over 90% of cases are associated with an unknown cause.1 SSNHL is generally defined as a SNHL of 30 dB or greater, involving three or more contiguous audiometric frequencies, which decline rapidly within 72 hours.2
Incidence
Although incidence reports vary year by year and with the particular population studied, the incidence of SSNHL appears to increase as the population ages from children to older adults. Contemporary estimates are approximately 5-27 cases of SSNHL per 100,000 people in the United States (eg, see Alexander & Harris 20133 and also Chandrasekhar et al, 20191). However, these estimates are likely low as many patients with mild symptoms or rapid recovery may not seek medical care. There appears to be a slight male preponderance, which is more pronounced in patients 65 years and older. Approximately 60,000-65,000 new cases of SSNHL are documented annually in the United States.
Etiology
In 2022, the etiology of SSNHL remains unknown for the majority of patients. As noted previously, SSNHL presents with no identifiable cause in >90% of cases.1 Possible etiologies include non-specific viral infections, bacterial infections, inflammation, head trauma, autoimmune disease, ototoxic drugs, attenuated blood flow or perfusion, neurological disorders, inner ear anomalies, neoplastic processes along the vestibular and/or cochlear nerves, and more.4
The cochlea is particularly vulnerable to insult given the delicate nature of inner ear structures (inner and outer hair cells, the Organ of Corti, etc), as well as the precarious status of the cochlea as an end organ. As such, the cochlea is entirely dependent on blood flow from a single artery (labyrinthine artery) without any collateral supply, making it extremely sensitive and susceptible to fluctuations in perfusion. A recent study found that the neurovascular fluctuations in migraine sufferers places these patients at increased risk for SSNHL.5
Diagnosis
The diagnostic workup of SSNHL includes a careful history, a thorough ear examination to rule out middle-ear pathology, comprehensive audiometric evaluation, and appropriate imaging studies to rule out retro-cochlear pathology. The imaging study of choice is magnetic resonance imaging (MRI) with gadolinium contrast using an internal auditory canal (IAC) protocol.
In patients who are unable to undergo an MRI scan, Auditory Brainstem Response (ABR) testing remains an acceptable (although less diagnostic) secondary alternative. When compared to MRI, ABR has relatively poor sensitivity regarding the identification of retrocochlear tumors. Approximately 20% of intracanalicular schwannomas (acoustic neuromas) may present on ABR as a false negative. Theoretically, when a small or very small tumor is present within the IAC or the cerebellopontine angle (CPA) yet is not in contact with the auditory portion of the 8th cranial nerve, it appears less likely to be identified via ABR.
Importantly, computerized tomography (CT) scans of the head and routine laboratory testing tend to not increase diagnostic profiles or accuracy (given SSNHL), and can result in false positives and increase the cost of care.1
Treatment
There is no perfectly predictable successful treatment for SSNHL. Some guiding principles for clinicians include early identification, evaluation to rule out conductive hearing loss, history and physical examination to identify an etiology or special characteristics (bilateral involvement, Meniere’s disease, focal neurological deficits), retrocochlear imaging to rule out vestibular schwannoma, patient counseling regarding the natural history and prognosis of SSNHL, administration of corticosteroids (systemic or transtympanic), and consideration for Hyperbaric Oxygen Therapy (HBOT).1
Early treatment—within the first days or week of onset—is generally associated with better hearing recovery based on clinical and anecdotal reports. Other features associated with improved recovery outcomes include younger patients, lesser degree of SNHL, and early improvements in hearing recovery.
When a causative etiology is identified, treatment recommendations are tailored to that specific etiology. For example, antibiotics would be useful for patients with a bacterial infection, and vestibular schwannomas can be treated with surgery or radiation therapy and/or can be watched over time to see if growth is apparent. Patients with other focal neurological findings should be referred for neurology workup.
For idiopathic causes of SSNHL, corticosteroid therapy remains the current mainstay of treatment in the United States. Corticosteroids can be administered via intratympanic injection (through the eardrum by an otolaryngologist) and orally (see NIDCD text in sidebar).4,6 The timing of corticosteroid delivery appears to be important and should be administered, ideally, during the first few days or first week of hearing loss onset.
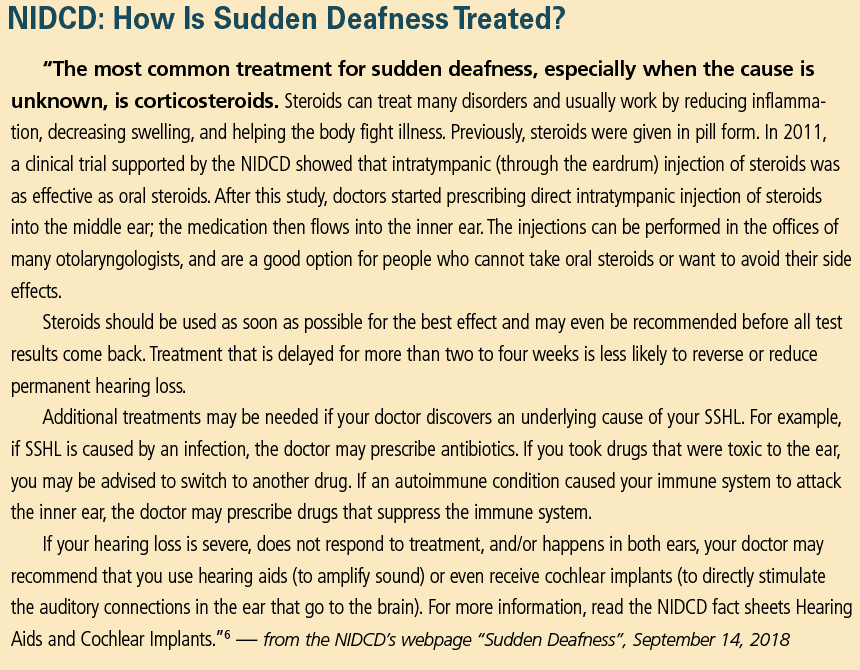
There is some evidence to support both oral corticosteroid administration and intratympanic steroid delivery.1 Oral steroids avoid a perforation in the tympanic membrane, but may have adverse systemic effects including weight gain and hyperglycemia in diabetic patients.
Intratympanic steroid injection avoids these systemic effects although it requires a simple office procedure which is typically well-tolerated by most patients. Up to four injections may be offered, and a tympanostomy tube may be placed to avail easy administration. Intratympanic steroid administration has also been used for salvage therapy (incomplete recovery after 4 weeks of onset).
A number of researchers have suggested that HBOT offers a potential benefit when used in tandem with corticosteroid therapy.7,8 Joshua et al8 recently examined the potential benefit of HBOT used in combination with medical treatment via meta-analysis and concluded HBOT was significantly associated with improved hearing outcomes (approximately a 10 dB improvement) in patients with SSNHL when compared to control treatment. HBOT has been used for both primary and salvage therapy.
Regarding medical therapies such as antivirals, thrombolytics, vasodilators, or vasoactive substances in cases of SSNHL, these medications have not been shown to provide benefit.1 Antioxidants may or may not be helpful. However, the physician must make these treatment decisions based on the clinical presentation, the needs of the specific patient, as well as the patient’s desires and goals.
Recovery
Recovery of hearing thresholds following SSNHL may not occur, may be partial, or may be complete. In 2020, Singh and Irugu9 reported some two-thirds of all cases may recover spontaneously, and other studies have reported a spontaneous recovery rate between 32% and 65%.1
At this moment (March 2022), it appears unlikely that a specific prognosis can be determined in most cases. An often-heard “rule of thumb” with regard to the natural progression (without treatment) of SSNHL is one-third get better, one-third stay about the same, and one-third get worse over time.
Generally, early intervention is associated with an increased chance for hearing recovery. Of note, when patients present later in the course of SSNHL (4 weeks after onset of hearing loss) they may still undergo “salvage therapy,” although such cases have a reduced expectation of recovery.
Factors associated with hearing recovery include age at onset of hearing loss, hearing loss severity, frequencies affected, presence of vertigo, and time between onset of hearing loss and visit with the treating physician.2 However, there may be features or characteristics yet unknown or unidentified in patients who seek early diagnosis and treatment (independent of time to treatment) which may facilitate a more beneficial outcome.
Hearing Rehabilitation
When SSNHL results in permanent hearing loss, the impact on quality of life (QOL) can be significant.10 Since most SSNHL is unilateral, affected patients will experience challenges similar to those with single-sided deafness (SSD). These challenges including difficulty with sound localization, speech understanding in noise, and (often) tinnitus. Hearing rehabilitation options for these patients include traditional amplification with hearing aids, CROS/BICROS amplification, bone-conduction devices (including osseointegrated implants), and cochlear implantation.11 Cochlear implants, recently FDA approved in the United States for SSD,12 offers the best chance to improve sound localization, hearing in noise, and tinnitus.
Future Treatments
Opportunities to medically treat permanent hearing loss from SSNHL exist on the horizon. A variety of new therapeutic strategies are under investigation that utilize small bioactive molecules delivered via transtympanic injection which diffuse across the round window membrane to act on specific targets in the inner ear. For example, one molecule has been designed to repair damage to synapses between inner hair cells and spiral ganglion cells, a pathology suspected to interfere with speech intelligibility (Alan Foster, Otonomy, personal communication, January 2022). Another combination of small molecules acts to stimulate progenitor cells in the cochlea, which are typically quiescent, into generating new hair cells without depleting the progenitor cell pool (Carl LeBel, PhD, Frequency Therapeutics, personal communication, January 2022). Bioactive molecules designed for inner ear delivery have demonstrated an acceptable safety profile, effective pharmacokinetic distribution in the perilymph, as well as improvements in tinnitus (see Maxwell et al13) and speech intelligibility.14
SSNHL and COVID-19
Although many have speculated about the relationship between SSNHL and COVID-19, it is relatively early and there remains a plethora of things we do not know (see the article by Robert DiSogra, AuD, in this edition of Hearing Review). However, a January 2022 publication in JAMA Otolaryngology-Head and Neck Surgery Research by Doweck et al15 studied over 3 million people with regard to SSNHL in 2018 and 2019, compared to the first pandemic year (2020). They reported a significant decrease in the incidence of SSNHL prior to vaccines being available. They note the decrease may be due to fewer people going to doctors’ offices unless the need was perceived as critical. The authors also note that perhaps the decrease was due to a reduction in respiratory viral infections, arguably due to less socialization, masking, and social distancing.
Conclusions
In 2022, Sudden Sensorineural Hearing Loss (SSNHL) remains a difficult problem to diagnose, manage, and resolve. SSNHL is a frustrating and difficult problem for patients. Very early diagnosis and treatment appear to be more successful and are highly recommended. Real-life difficulties secondary to SSNHL are significant and negatively impact the patient’s quality of life.
Correspondence can be addressed to HR or Dr Beck at: [email protected].
Citation for this article: Beck D, Grisel JJ. Sudden sensorineural hearing loss (SSNHL): A status report 2022 Hearing Review. 2022;29(3):14-18.
References
- Chandrasekhar SS, Do BST, Schwartz SR, et al. Clinical practice guideline: Sudden hearing loss (update) executive summary. Otolaryngol–Head Neck Surg. 2019;161(2):195-210.
- Kuhn M, Heman-Ackah SE, Shaikh JA, Roehm PC. Sudden sensorineural hearing loss: A review of diagnosis, treatment, and prognosis.Trends Amplif. 2011;15(3): 91-105.
- Alexander TH, Harris JP. Incidence of sudden sensorineural hearing loss. Otol Neurotol. 2013;34(9):1586-1589.
- National Institute on Deafness and Other Communication Disorders (NIDCD) website. NIDCD Fact Sheet, Hearing and Balance, Sudden Deafness. https://www.nidcd.nih.gov/health/sudden-deafness. Published March 2018.
- Akbarpour M, Lee A, Tawk K, Martin E, Mehdi A, Djalilian H. Migraine Features in Patients with Sudden Sensorineural Hearing Loss. Poster presented at: The 2022 Triological Society Combined Sections Meeting; January 20-22, 2022; Coronado, CA.
- National Institute on Deafness and Other Communication Disorders (NIDCD) website. NIDCD Fact Sheet, Hearing and Balance, Sudden Deafness. https://www.nidcd.nih.gov/health/sudden-deafness. Published March 2018.
- Moody-Antonio SA, Chandrasekhar SS, Derebery MJ. Is it time to encourage hyperbaric oxygen therapy in combination with medical treatment for sudden sensorineural hearing loss? JAMA Otolaryngol Head Neck Surg. 2022;148(1):11-12.
- Joshua TG, Ayub A, Wijesinghe P, Nunez DA. Hyperbaric oxygen therapy for patients with sudden sensorineural hearing loss: A systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2022;148(1):5-11.
- Singh A, Irugu DVK. Sudden sensorineural hearing loss – A contemporary review of management issues. J Otol. 2020;15(2):67-73.
- Galloway J, Zhang V, Marnane V, Hou S, Stewart G, Bardy F. The impact of unilateral hearing loss on adult life. Hearing Review. 2019;26(4):10-14.
- Beck DL, Ramachandran V. Contralateral routing of signal: A status report 2019. Hearing Review. 2019;26(10):12-16.
- Cochlear Nucleus Receives FDA Approval for UHL/SSD. News release. Hearing Review. January 11, 2022. https://hearingreview.com/hearing-products/implants-bone-conduction/cochlear-implants/cochlear-nucleus.
- Maxwell KS, Robinson JM, Hoffmann I, et al. Intratympanic administration of OTO-313 reduces tinnitus in patients with moderate to severe, persistent tinnitus: A phase 1/2 study. Otol Neurotol. 2021;42(10):e1625-e1633.
- McLean WJ, Hinton AS, Herby JTJ, et al. Improved speech intelligibility in subjects with stable sensorineural hearing loss following intratympanic dosing of FX-322 in a Phase 1B study. Otol Neurotol. 2021;42(7):e849-e857.
- Doweck I, Yanir Y, Najjar-Debbiny R, Shibli R, Saliba, W. Sudden sensorineural hearing loss during the COVID-19 pandemic. JAMA Otolaryngol Head Neck Surg. 2022. DOI:10.1001/jamaoto.2021.4105.
From the HR Archives…
Special Issue: Sudden Sensorineural Hearing Loss, guest edited by Maurice Miller, PhD | December 2003 Hearing Review