
Revisiting the research of Jurgen Tonndorf
On a routine basis, we conduct audiometric testing and expect the bone conduction (B/C) thresholds to accurately measure a patient’s cochlear reserve. This paper describes a phenomenon called pseudosensorineural hearing loss caused by a “loading effect” of middle ear pathology on the oval and/or round window of the cochlea.

|

|
| C. Michael Hall, AuD, is an audiologist who lives in Walnut Creek, Calif, is retired from private practice, and is now serving as a consultant in the hearing industry. Carl Croutch, AuD, is an audiologist at Kaiser Permanente Hearing Center in Daly City, Calif. | |
Audiometric threshold measurements of bone conduction (B/C) are assumed to be a valid measure of a patient’s cochlear reserve. However, there are a number of factors that can cause the B/C measurements to be inaccurate. The bone oscillator that we use in audiometric testing is one of the most sensitive pieces of equipment utilized for diagnostic testing. One of the first things we learn when we are training to administer a hearing test is to be careful with the bone oscillator: don’t drop it, don’t let patients handle the oscillator, always ensure that the spring-loaded headset is fairly tight, and that it is placed on the part of the mastoid promontory that is most sensitive.
Because the bone oscillator is so sensitive, a “red flag” goes up if we frequently get B/C thresholds that are not compatible with air conduction (A/C) thresholds. For example, if we consistently get B/C thresholds that are worse than A/C thresholds, we are alerted to either a malfunctioning oscillator, or an oscillator that is out of calibration. Further, because the oscillator’s maximum output is limited and there is distortion at the higher levels of output, B/C has innate problems other than loading or miscalibration.
In addition to errors that can be caused by faulty equipment, we can get “pseudosensorineural” measurements as a result of malfunctions of the middle ear. Pseudosensorineural thresholds are audiometric B/C losses caused by a “loading effect” of a lesion on the oval and/or round window of the cochlea.
What Is a Pseudosensorineural Hearing Loss?
As stated earlier, we assume that B/C measurements with calibrated and functioning equipment provide us with valid clinical measurements of a patient’s sensorineural reserve. When an initial audiogram shows a sensorineural hearing loss and also a conductive hearing loss, a mixed hearing loss is typically the interpretation of the results.
However, sometimes following the correction of the middle ear pathology, we get B/C thresholds that are better than the initial thresholds. Historically, many clinicians and ENTs interpret medical/surgical intervention to be the reason for improved B/C thresholds. The improved thresholds are frequently referred to as being “over-closures,” meaning that the patient had a sensorineural loss, and through medical intervention, the sensorineural component was corrected.
There are a number of factors that make that assumption invalid. First, the concept of “over-closure” does not fit into any of the current models of how B/C works. Second, there have never been any documented cases where a sensorineural hearing loss has been surgically corrected, except for instances of a perilymph fistula—cases where the oval or round window has developed a leak of perilymph fluid. Patients with these disorders would manifest themselves typically as having equilibrium problems and changes in hearing. (We also are not talking about Méniere’s disease in which the sensorineural hearing fluctuates in the early stages due to changes occurring in the cochlea.)
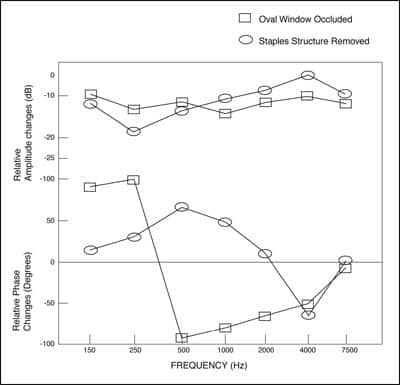
However, based on clinical observations and lab studies with animals, we have learned that the improved (pseudosensorineural) thresholds are typically not a result of an “over-closure,” but a result of the initial middle ear pathology causing a “loading effect” on the functioning of the oval or round window of the cochlea (Figure 1).
|
| FIGURE 1. Two bone-conduction components calculated from the experimental results of Tonndorf.5 |
Looking Back to Bárány, Carhart, and Tonndorf
The first report in the medical literature that a “loading effect” can cause a pseudosensorineural hearing loss was made by Bárány in 1910.1 Carhart2 in the early 1950s noted a notch at 2 kHz on occasion with patients who had otosclerosis. The notch has come to be called the “Carhart notch.”2
|
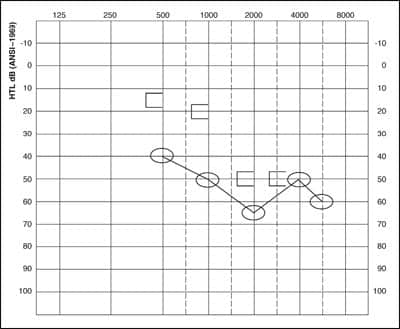
| FIGURE 2A. Initial audiogram of a patient with otosclerosis. |
|
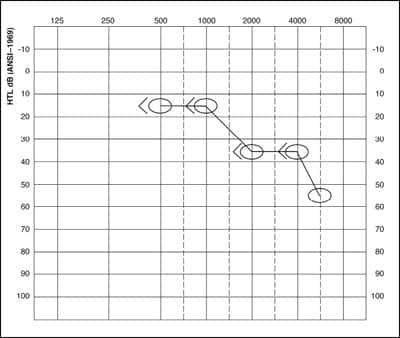
| FIGURE 2B. Post-treatment audiogram of a patient with otosclerosis. |
Figure 2a is an example of an audiogram showing a Carhart notch with otosclerosis present. Figure 2b shows the same patient’s audiogram following a successful stapedectomy surgery. Note, Figure 2b indicates that the B/C thresholds were improved following the surgery. This is a characteristic finding sometimes seen in patients with otosclerosis.
|
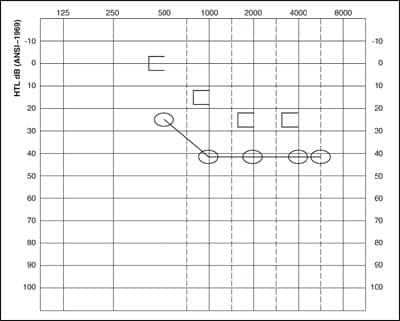
| FIGURE 3A. Initial audiogram of a patient with otitis media. |
|
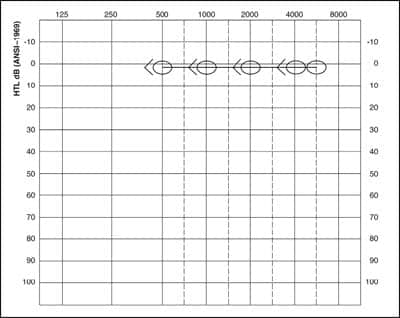
| FIGURE 3B. Post-treatment audiogram of a patient with otitis media. |
Figures 3a and 3b are “before and after audiograms” of an 8-year-old with otitis media. The initial audiogram (Figure 3a) shows a mixed hearing loss. When tubes were inserted, the follow-up audiogram in Figure 3b shows normal hearing.
These conundrums are demonstrative of pseudosensorineural hearing loss. Understanding what causes this and how B/C actually works was explained by studies made by the great otologist/scientist Jurgen Tonndorf, as well as others, following years of clinical observation and laboratory experiments. With these various types of studies, Tonndorf went on to develop a more plausible understanding of how B/C and the “loading effect” can affect B/C thresholds.
Tonndorf’s laboratory studies3-5 involved anesthetized animals. Using very controlled conditions that he developed, he was able to take various laboratory animals, such as cats, mice, and dogs, and then open their middle ear. Using cochlear microphonics, he then loaded various parts, such as the disarticulation of the ossicles, stapes footplate, and the oval and/or cochlear windows. Although the hearing thresholds of laboratory animals are not the same as those of humans, the amount of loss or improvement is comparable with what would be observed with humans. This “loading effect” produced repeatable laboratory measurable pseudosensorineural hearing losses.
The following is a list of the various middle ear lesions that have the potential to cause a pseudosensorineural hearing loss:
- Otosclerosis
- Slipped stapedial strut
- Cerumen impaction occluding the tympanic membrane
- Sclerotic middle ear
- Otitis media
- Negative middle-ear pressure
Although Tonndorf could replicate the “loading effect” in the laboratory by loading various parts of the middle ear, he went on to observe that, clinically speaking, pseudosensorineural hearing loss is not consistently observed in patients with middle ear pathology.
However, it obviously does occur. Usually when it is present, it manifests itself on the order of a range from a 15 dB to 20 dB sensorineural loss. To briefly summarize, he stated that the presence or absence of a pseudosensorineural loss is determined by the effect that a particular middle-ear lesion has on the various components that determine phase relations of B/C thresholds.
Summary
This article discusses a phenomenon of pseudosensorineural hearing loss that can occur when various middle ear lesions are present and a “loading effect” occurs. The pseudosensorineural hearing loss has mistakenly been termed “over-closure” by clinicians for years. A factor that limits us in specifying a particular hearing loss as a pseudosensorineural loss is that a patient has to have treatment of the middle ear lesion or lesions and a post-treatment audiogram must be performed. Although hearing aid clinicians rarely see this phenomenon in their hearing aid clientele, they should be aware of it as an additional reason why patients presenting with a mixed hearing loss should be referred for medical examination.
References
- Bárány R. Mschr Ohrenheilk Lar-Rhinol. 1910;44:549.
- Carhart R. Acta Otolaryngol. 1951;511:798.
- Tonndorf J. Compressional bone conduction in cochlear models. J Acoust Soc Am. 1962;34:1127-1131.
- Tonndorf J. A new concept of bone conduction. Arch Otolaryngol. 1968;87:595-600.
- Tonndorf J. Bone conduction: studies in experimental animals. Acta Otolaryngol. 1966:suppl 213:1-132.
Correspondence can be addressed to or C. Mike Hall, AuD, at .
Citation for this article:
Hall CM, Croutch C. Pseudosensorineural Hearing Loss. Hearing Review. 2008;16(1):18-22.



