

|
| Vishakha W. Rawool, PhD, is a member of the faculty in the Department of Speech Pathology and Audiology at West Virginia University, Morgantown, WVa. |
The cochlear implant (CI) is a well-accepted option for deaf children and adults. In most cases, the major goal of this technology is to provide sufficient hearing to promote the development of spoken language in children and adequate speech recognition in adults. However, this technology also can be a viable option for families who are planning to use only sign language with their children or for adults who exclusively communicate through sign language.
Part 1 of this two-part series provides a review of potential uses of cochlear implants for individuals who may not want to use this technology for spoken language recognition or development. Part 2 will look at issues involving cochlear implants and access to music.
Use of Technology by ASL Users
Many deaf individuals are savvy users of all types of technology, including computers, pagers, hearing aids, fax machines, and a variety of technologies that allow instant messaging. Effective use of modern technology can provide greater accessibility to deaf individuals and can help in leveling the playing field.
The Deaf community respects the rights of individuals to make personal choices—including the choice of cochlear implants. Some well-respected members of the Deaf community have opted for CIs, which suggests that some individuals who are prelingually and/or “culturally deaf” are interested in capitalizing on the added sound value offered by CIs.
The Normal Cochlea
The human inner ear or cochlea has approximately 3,500 inner hair cells and 12,000 to 20,000 outer hair cells. These sensory hair cells collaboratively assist in transferring the mechanical vibrations in the cochlea (generated by sound waves reaching the ear) into neural/electrical impulses.
In a normal cochlea, outer hair cells assist in providing high sensitivity to soft sounds and the ability to perceive very small changes in pitches. However, most of the nerve fibers that carry information from the cochlea to the brain are attached to the base of the inner hair cells. Thus, the survival of the inner hair cells is crucial for hearing. Each inner hair cell is innervated by approximately 20 different neural fibers.
Spectral resolution in the normal cochlea. Different frequencies stimulate different regions of the cochlea, more specifically the basilar membrane. For example, higher frequencies mainly stimulate basal regions. This results in the stimulation of different populations of nerve fibers that are located from the base to the apex.
One mechanism of coding of sound frequency by the cochlea can be conceptualized as division of the incoming sound into several frequency bands, with each portion of the basilar membrane highly responsive (or tuned) to a different frequency.
Each nerve fiber also has a characteristic frequency to which it is highly responsive. This type of coding of the frequencies in the cochlea and nerve fibers is partially responsible for our ability to perceive fairly small changes in pitch.
Function of Cochlear Implants
In individuals with severe-to-profound hearing loss, the number of surviving inner hair cells is very low. Thus, presentation of louder sounds to the ear via hearing aids does not necessarily help, since there are insufficient hair cells to transfer the mechanical vibrations in the cochlea into neural impulses. Nerve fibers need to be stimulated by neural/electrical impulses. Mechanical vibrations delivered to the cochlea through hearing aids cannot be directly received by nerve fibers without being converted to neural impulses.
CIs are designed to bypass the function of the inner hair cells and thus provide direct electrical stimulation to the nerve fibers. Research has shown that survival of as few as 3,500 spiral ganglions (cell bodies of the neurons of the cochlear nerve) is sufficient to provide adequate stimulation with cochlear implants. In 80% of the cases, spiral ganglion counts equal or exceed 3,500,1 and lower counts are not necessarily related to poor performance with a CI.2
Thus, some benefit from implantation can be expected in most individuals, with the exception of those who do not have an auditory nerve.
Characteristics of cochlear implants. All CIs present different frequencies of the incoming acoustic signals along the electrode array from base to apex, with higher-frequency information presented to the electrodes that are at the base and the lower-frequency information presented to those at the apex. The number of discrete pitches that can be perceived by the listener when current is delivered to different electrode locations is referred to as the number of useful spectral channels.
Until recently, the number of spectral channels in CIs was equal to the number of viable electrodes that could be used to deliver electrical stimuli. Thus, in theory, the incoming signal would be divided into 16 spectral channels if 16 electrodes were stimulable, and then carried by the nerve fibers to the brain for reconstruction. Even with division of the signal in a few spectral channels (eg, 22 or less), auditory signals—including speech—can be recognized following repeated exposure to the signal.
Recent advances in cochlear implant technology. CI technology is continuously evolving. New software upgrades in some cochlear implants now have the potential to further improve spectral resolution. The improved spectral resolution is achieved by creating virtual spectral channels without the presence of actual additional electrodes, using a technique called current steering.
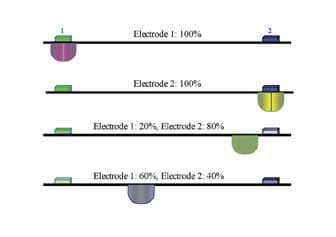
The virtual spectral channels are created by delivering the electrical current in varying proportion, simultaneously, to pairs of adjacent electrodes—thus steering the effective cochlear site of stimulation somewhere between the electrode pairs. In other words, the site of stimulation is adjusted by manipulating the proportion of current delivered to each electrode in the electrode pair. The currents delivered to the electrode pair interact in the cochlea and create an intermediate “virtual channel.”
|
| FIGURE 1. A simplified illustration of “current steering” to create more channels within a cochlear implant. The site of stimulation is adjusted by manipulating the proportion of current delivered to each electrode in the electrode pair. The currents delivered to the electrode pair interact in the cochlea and create an intermediate “virtual channel.” |
A highly simplistic view of current steering is depicted in Figure 1. The last two rows illustrate virtual channels through current steering. Note that the virtual channels that are created between the electrodes differ in site of stimulation due to the difference in the proportion of current delivered to the two electrodes.
As an example, if 16 electrodes are active, 15 pairs of electrodes are available. If, for each electrode pair, eight spectral bands are created, then (in theory) as many as 120 (15 x 8) spectral channels can be made available using the current steering technique.
Data from 57 implanted ears suggest that the numbers of spectral channels for each electrode pair can range from one (ie, subjects who could not tell any of the electrodes apart) to 52 (an individual could perceive 52 different pitches for one pair of electrodes).3 All individuals included in this study had at least 3 months of experience with the implant and 12 or more usable electrodes. For the 57 ears, the number of available spectral channels ranged from 8 to 466, with an average of 93.
Access to Soundscapes Through CIs
If we are in a desert, we may see a dull landscape with miles and miles of sand and nothing else. We enjoy the landscape better when we see a waterfall surrounded by green trees blooming with flowers, green grass populated by butterflies, blue skies occasionally sprinkled by a flock of birds, or a skyline that is lit up with bright vibrant colors at sunset or sunrise. Our life-experience can be enhanced with exposure to such landscapes.
The soundscapes that accompany such landscapes play an important role in enhancing the sensory experience. For example, the landscape described above is generally accompanied by a soundscape that includes the soothing sound of water from the waterfall, the chirping of birds, and the rustling of leaves. In addition to enriching the overall sensory experience, such sounds can be enjoyed even in the absence of the visual landscape by closing our eyes, providing a calming and soothing effect.
Movies often use sound effects to intensify the drama by arousing emotions and creating mood. Special sound effects engineers are employed to achieve these effects, and the best efforts are recognized by the movie industry at its annual Academy Awards presentations. This underlines the significance of soundscapes.
The implication of soundscapes is obvious in individuals with sudden severe acquired hearing loss. Such individuals often report depression due to the lack of access to soundscapes and the ensuing feeling that the world around them appears dead.
CIs have the potential to provide access to soundscapes for individuals with severe to profound hearing loss. Following implantation, CI users often report enjoying listening to raindrops, the giggles of babies or grandchildren, or simply the voices of their children. They also feel more relaxed, calmer, and more connected to the world.
New current steering techniques can be expected to make it easier to differentiate among different environmental sounds and thus further enhance the perception of soundscapes.
Access to warning sounds. A potential use of cochlear implants for sign-language users is to provide awareness of sounds that are important for the individual’s safety, such as the sound of an approaching vehicle from behind the listener, fire alarms, or other alerting signals. Prelinguistically deaf adults report feeling safer following cochlear implantation.4
Relief from Tinnitus Due to CI Use
The ability to hear silence or be surrounded by quiet is as important as the ability to hear environmental sounds. Some individuals do not have the luxury of being able to hear silence due to the continuous ringing (tinnitus) they experience.
Impact of tinnitus. Tinnitus, in some cases, can dramatically affect a person’s quality of life. Imagine going to a quiet place and instead of surrounded by silence, you hear a continuous high-pitched ringing or feel that a bug is constantly buzzing in your ears. A visual analogy of tinnitus would be seeing a red dot or dots of several different colors that are constantly within your eyesight.
The effect of tinnitus may be even worse for individuals who have severe-to-profound congenital hearing loss and thus have not heard many environmental sounds, but instead constantly hear a meaningless buzz or tone in their ears. The sounds due to tinnitus may even make them averse to the idea of hearing any other sounds unless they are properly informed. Among individuals with hearing loss, troublesome tinnitus has been shown to be associated with lack of paid employment.5
The risk of tinnitus in CI candidates. The risk of tinnitus increases with hearing loss.6 Coles et al7 investigated the occurrence of tinnitus, which they defined as the ringing or buzzing sound in the head or ear(s) that lasts for 5 minutes or more and does not occur after a loud noise. With every 10 dB increase in hearing level measured at 4,000 Hz in the better ear, the odds of moderate-to-severe tinnitus were higher. Compared to individuals with 10 dB HL thresholds, individuals with thresholds of 80 dB or higher (severe-to-profound loss) were 27 times more likely to suffer from moderate-to-severe tinnitus. Preoperatively, tinnitus has been reported in as many as 84% to 85% of CI recipients.8,9
Effect of CIs on tinnitus. Several investigators have reported significant relief from tinnitus following cochlear implantation. Overall, 71% to 92% of the patients report tinnitus suppression or elimination due to CIs, especially in the ear with the implant. In addition, many patients report relief in the nonimplanted ear.8-11 Furthermore, several patients experience relief for 60 seconds to several hours after the CI is turned off.9 Up to 9% of patients may report exacerbation of tinnitus, suggesting a relatively small risk of increase in tinnitus following cochlear implants.12
Mo et al5 compared the effect of hearing aid use and CI use on troublesome tinnitus. A reduction in troublesome tinnitus was reported by 54% of the CI patients, while only 23% of the hearing aid users who were candidates for CI reported reduction.
Overall, the above findings suggest that CIs can provide at least some, if not complete, relief from tinnitus for a majority of patients.
Access to Music Through CIs
For individuals with severe-to-profound hearing loss, CIs can provide better access to music compared to hearing aids. This important topic is reviewed in greater detail in Part 2 of this article.
Improvement in Overall Quality of Life
Wyatt et al13 concluded that profound hearing loss has a significant impact on quality of life, and CIs can significantly improve the quality of life in a cost-effective manner. CIs also have a significant impact on the quality of life of older deaf patients and are shown to be cost-effective for this population.14 The benefits of CIs are not limited to auditory benefits, but are extended to improvement in physical, psychological, and social functions.14,15 Enhancement in audition with an implant is mainly responsible for the overall rise in quality of life following cochlear implantation.14 CIs may also enhance family life.16
In general, CI recipients report an increase in confidence, self-esteem, and social activities. Recent studies have also shown that, although prelingually deafened adults do not perceive speech as well as postlingually deafened adults through CIs, they report significant benefits after implantation in several areas, including overall improvement in quality of life and decrease in the feeling of isolation.4
Summary
Many ASL users are savvy at capitalizing on several technologies for their benefit, and thus they can be expected to benefit from CIs as well. Individuals who have severe-to-profound deafness often have very few surviving inner hair cells. Thus, providing amplified sounds through hearing aids is often inadequate since inner hair cells are necessary to transfer the mechanical vibration in the inner ear caused by sounds presented to the ear into neural/electrochemical impulses. CIs bypass the function of the inner ear and directly stimulate the nerve fibers.
An obvious benefit of the CI technology for profoundly deaf individuals is access to warning signals for safety. For many patients who are suffering from tinnitus, the CI may provide partial or total relief from it. In addition to this, the current cochlear CI technology may lead to enhanced access to soundscapes and music. All of the above can have a significant impact on the quality of life of CI users and their families.
References
- Linthicum FH, Anderson W. Cochlear implantation of totally deaf ears: histologic evaluation of candidacy. Acta Otolaryngol. 1991;111:327-331.
- Fayad JN, Linthicum FH Jr. Multichannel cochlear implants: relation of histopathology to performance. Laryngoscope. 2006;116:1310-20.
- Koch DB, Downing M, Osberger MJ, Litvak L. Using current steering to increase spectral resolution in CII and HiRes 90K users. Ear Hear. 2007;28:38S-41S.
- Koch DB, King CD, Vujanovic I, Osberger MJ. Everyday cochlear implant benefit in prelingually deafened adults. Paper presented at: American Auditory Society; March 7-9, 2004; Scottsdale, Ariz.
- Mo B, Harris S, Lindbaek M. Tinnitus in cochlear implant patients—a comparison with other hearing-impaired patients. Int J Audiol. 2002;41:527-34.
- Mitchell P. Factors predicting severity of tinnitus: a population-based assessment. J Am Acad Audiol. 2004;15:29-280.
- Coles R, Davis A, Smith P. Tinnitus: its epidemiology and management. In: Jensen JH, ed. Proceedings of the Fourteenth Danavox Symposium. Copenhagen: Danavox Jubilee Foundation; 1990:377-402.
- Ito J, Sakakihara J. Tinnitus suppression by electrical stimulation of the cochlear wall and by cochlear implantation. Laryngoscope. 1994;104:752-754.
- Souliere CR Jr, Kileny PR, Zwolan TA, Kemink JL. Tinnitus suppression following cochlear implantation: a multifactorial investigation. Arch Otolaryngol Head Neck Surg. 1992;118:1291-1297.
- Yonehara E, Mezzalira R, Porto PRC, et al. Can cochlear implants decrease tinnitus? Int Tinnitus J. 2006;12:172-174.
- Ruckenstein MJ, Hedgepeth C, Rafter KO, Montes ML, Bigelow DC. Tinnitus suppression in patients with cochlear implants. Otol Neurootol. 2001;22:200-204.
- Quaranta N, Wagstaff S, Baguley DM. Tinnitus and cochlear implantation. Int J Audiol. 2004;43:245-251.
- Wyatt JR, Niparko JK, Rothman M, deLissovoy G. Cost utility of the multichannel cochlear implant in 258 profoundly deaf individuals. Laryngoscope. 1996;106:816-121.
- Francis HW, Chee N, Yeagle J, Cheng A, Niparko JK. Impact of cochlear implants on the functional health status of older adults. Laryngoscope. 2002;112:1482-1488.
- Hinderink JB, Krabbe PFM, Van den Broek P. Development and application of a health-related quality-of-life instrument for adults with cochlear implants. The Nijmegen Cochlear Implant Questionnaire. Otolaryngol Head Neck Surg. 2000;123:756-765.
- Faber CE, Grontved AM. Cochlear implantation and change in quality of life. Acta Otolaryngol. 2000;543(suppl):151-153.
Correspondence can be addressed to [email protected] or to Vishakha Rawool, PhD, at .



