|

|

|

|

|
| Sergei Kochkin, PhD, is executive director of the Better Hearing Institute, Alexandria, Va; William Luxford, MD, is an otolaryngologist at House Ear Clinic, Los Angeles, and clinical associate professor of otolaryngology at the University of Southern California School of Medicine; Jerry L. Northern, PhD, is professor emeritus at the University of Colorado School of Medicine, Department of Otolaryngology (Audiology), Denver, Colo; Pam Mason, MSEd, is director of audiology professional practices at the American Speech-Language-Hearing Association (ASHA), Rockville, Md; and Anne Marie Tharpe, PhD, is an Professor of audiology at the Vanderbilt School of Medicine, Nashville, Tenn. | ||||
Earlier in this research series on the hearing loss population,1 it was determined that there were 1.2 million children ages 0 to 17 in the United States: 1) whose parents admitted that their children had “hearing difficulties,” and that 2) the children did not use amplification. Additionally, using the Better Hearing Institute (BHI) MarkeTrak VII database, it is estimated that there are another 300,000 dependents ages 18 to 21 with unamplified hearing loss. Thus, we estimate that about 1.5 million dependents ages 0 to 21 have a hearing problem but are currently not users of hearing aids.
With hearing aid adoption rates at only 12% for the pediatric population (ie, individuals younger than age 18),1 it is important to explore this issue further. Few would disagree that, for optimum development, “every child with hearing loss has a basic human right to communication access.”2
In light of this, the above statistics raise several serious questions. What portions of the hearing difficulties experienced by this young population are due to transitory ear infections, unaidable sensorineural hearing loss, or the lack of residual hearing in one or both ears? Are these dependents in need of surgery and thus not candidates for hearing aids, or is the hearing loss so trivial that it has little or no impact on their quality of life? What are the obstacles facing children and dependents in America for receiving hearing aids or other amplification treatment for their hearing loss?
Study Methods
A detailed survey methodology is documented in earlier articles in this series1 and the reader is referred to this publication or the hearingreview.com archives for details.
In June 2005, querying the BHI MarkeTrak VII database, we identified 475 dependents under age 22 who reported having hearing difficulty but who were not hearing aid users. We sent a detailed survey to the parent of each dependent. The response rate to the dependent’s survey was 52% (n=248). However, upon further investigation of responses, 4% of the dependents were deemed to have transitory hearing problems due to ear infections (ie, the parent indicated the dependent did not have a hearing loss) and another 5%, according to their parents, did not have hearing loss but only tinnitus.
These dependents were excluded from the results to follow. Thus the responses shown here are based on a total sample size of 225 subjects, and all were reported by their parents to have hearing loss.
In the survey, parents were asked to write the BHI a letter discussing four issues:
- Nature of the dependent’s hearing loss;
- Treatment sought;
- Impact of hearing loss on the dependent’s life, and
- Reason why the dependent does not use hearing aids.
A total of 87% of parents returned letters answering one or more of our questions in support of their survey responses.
|
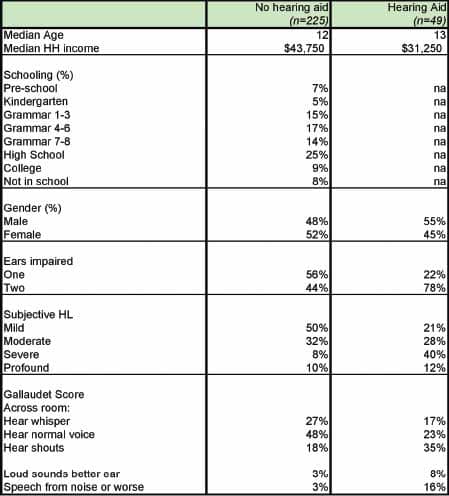
| TABLE 1. Demography of children/dependents with hearing loss who do not use amplification. Note: children with only tinnitus or transitory hearing loss due to ear infections were removed from the survey. |
Results
Demography. In Table 1, the demography of dependents with (n=49) and without (n=225) hearing aids is documented from the MarkeTrak VII database. The median age is 13 years and 12 years for aided and unaided dependents, respectively, and the households of nonaided dependents are more affluent (by about $12,000 per year). The dependents are almost equally split between males and females. However, there are significant differences in dependents with bilateral hearing loss: 78% of dependents with bilateral losses were hearing aid users compared to 44% of nonusers.
On a four-point subjective hearing loss scale (mild, moderate, severe, profound), 80% of dependents with hearing aids were more likely to be classified as having a moderate to profound hearing loss compared to 50% of dependents without hearing aids; however, as subjectively measured by the Gallaudet hearing loss scale,3 there is only a 10% point difference in their inability to “hear a whisper across a room without visual cues.”
|
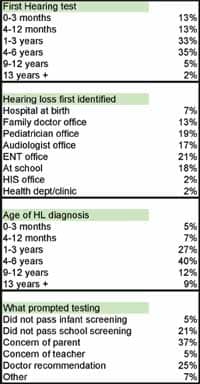
| TABLE 2. Hearing loss testing and diagnosis for the unamplified/non-owner dependent survey population. |
The Gallaudet Scale measures hearing loss subjectively. The parent indicates whether their dependent can understand speech under the following conditions: “whisper across a quiet room,” “normal voices across a quiet room,” “shouts across a quiet room,” “loud speech spoken into their better ear,” and “not able to understand loud speech in their better ear.” In addition, the test assesses if they can “tell noises from each other,” “hear loud noises at all,” or “hear any sound or any noise.” An individual’s score ranges from 1 to 8. Typically, the subject is classified into one of five groups: 1) hear whisper; 2) hear normal voice; 3) hear shouts; 4) hear loud speech in better ear; 5) can’t hear speech.
The Gallaudet Scale, which has been validated against clinical information (dB loss in the better ear) has historically been used by the Centers for Disease Control and Prevention (CDC) in their quantification of the hearing-impaired population. In the present survey, both populations (hearing aid users and nonusers) have difficulty understanding whispered speech across a room—73% of unamplified dependents and 83% of dependents with hearing aids. Conceivably, in a reverberant and noisy schoolroom, this degree of hearing loss could be exacerbated.
In Table 2, information concerning the hearing loss testing and diagnosis is presented for the unamplified dependent population. The dependent’s first hearing test generally was received between the ages of 1 and 6 years, with modal diagnosis occurring between ages 4 and 6 years, usually in a physician’s office. Only 7% of hearing losses were first identified at the hospital at birth. The most frequent events that prompted the hearing test were a parent’s concern (37%), a physician recommendation (25%), and the child failing a hearing test at school (21%).
|
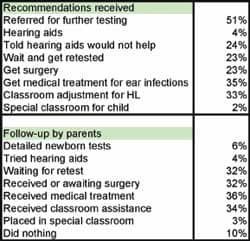
| TABLE 3. Recommendation(s) received from health care professionals and subsequent action(s) taken by the parents/caregivers in the unamplified/non-owner dependent survey population. |
Recommendations received. Referring to Table 3, about half the dependents have been referred for further hearing tests; 1 in 4 have been advised to get surgery, while a third of the dependents were referred for medical treatment for ear infection. A quarter of the subjects were told that hearing aids would not help, and 4% were referred for hearing aids. One in 3 dependents received a recommendation for classroom assistance (eg, preferential seating or assistive listening devices) while 2% were recommended for special classrooms for children with hearing loss.
It would appear that the vast majority of parents explored the options presented to them by a medical or hearing care professional. For instance, 4% were referred for hearing aids and 4% actually explored hearing aids. Only 10% of the subjects did nothing after receiving recommendations specific to their dependent’s hearing loss.
Quality of life impact. About 1 in 3 dependents received some form of classroom assistance. While a third of the subjects received preferential seating, only 3 parents mentioned that their child received assistive listening devices in the classroom.

|
| TABLE 4a. Impact of school intervention on school performance (in %). |
In Table 4a, parents indicated that 3 in 5 dependents’ grades improved (61%) and roughly half reported improvements in the dependent’s social skills (46%), classroom behavior (51%), and self-esteem (49%) following implementation of the recommended intervention.
|
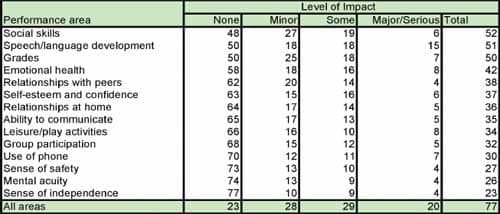
| TABLE 4b. Impact of hearing loss on quality of life (in %) sorted by total impact. |
In Table 4b, the impact of the dependent’s hearing loss on 14 quality-of-life issues was assessed using a five-point scale ranging from “no impact” to “serious impact.” Including dependents who experienced any level of impact due to hearing loss, 3 out of 4 parents indicated their dependent experienced “minor” to “serious” problems. The most serious problems experienced in rank order were: social skills (52%), grades in school and language development (50%), emotional health (42%), followed by relationships with peers (38%), self-esteem (37%), and relationships with family (36%). Figure 1 provides a summary of the percent of dependents currently not treated with amplification who experience problems as a result of hearing loss.
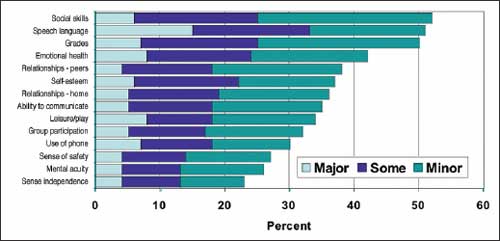
|
| FIGURE 1. Impact of hearing loss on quality of life for unamplified dependents. |
Parents’ Perspectives: Impact of Hearing Loss on Their Child’s Quality of Life
Quality-of-life issues run the gamut perceptually from personal nuisance, to the need for personal attention in school, to a major disability affecting all areas of life. The following statements reflect the feelings and observations of some of the parents and dependents who provided letters to the BHI. Some of the responses by parents seem flippant and, at times, reflect a lack of understanding or acceptance of the dependent’s experience.
In the remainder of this paper, for each key results section, we have attempted to supplement survey results with responses from the short letters received from parents. For each comment where information is available, we have tried to shed some light on the dependent’s demography (age, gender) and hearing loss (subjective classification) as described by the parent.
In many cases the reader will notice that the subjective evaluations are not in agreement with the dependent’s functioning in the world. Unless otherwise stated, the commentaries are by the parent and reflect their current understanding of their dependent’s situation—right or wrong. As an example, a parent may describe that their child has a mild hearing loss followed by behavioral indications that the child’s hearing loss is probably much worse; or the parent may indicate that they have been told that their child cannot be helped because of the uniqueness of their hearing loss (eg, the child has a high frequency hearing loss indicative of sensorineural hearing loss which, in all probability, could be addressed with hearing instruments).
“Sometimes I can’t hear some things people say to me if they speak softly or from a distance. I listened to loud music too much. Mom gets upset with me when I still listen too loudly to music and then she says I didn’t hear her when she talks to me. When I’m in school, I sit in the front so I can hear.”—18-year-old dependent with a mild hearing loss
“She gets very frustrated and wants to give up because she isn’t like other people.”—Parent of a 17-year-old girl with perforated eardrum that required surgery and resulted in subsequent scarring and moderate hearing loss
“She has difficulty hearing voices if there are background voices. Professionals find nothing abnormal. She is frustrated when she can’t hear her friends in the hall or cafeteria at school. We tell her to turn down the TV and lower her voice.”—Parent of a 15-year-old female with a mild hearing loss
“She has always not heard something. Recent physical included a hearing test, which she did not pass. School tests did not indicate any problems. Minor effect. When she does not hear being told something it [is] because she did not want to hear it, of course. She does not want a medical solution. The doctor’s opinion is that’s OK. We just make sure she [does] hear us when it’s important.”—Parent of a 14-year-old female with moderate hearing loss who cannot hear whisper
“Evan is a happy, well-adjusted 10 year old who has been in an after school program now since second grade. His hearing loss is treated matter-of-factly by Evan, his family, and his teachers.”—Parent of a 10-year-old male with congenital cholesteatoma who required surgery twice and now experiences a 25% hearing loss
“The only effects so far are having to sit in the front of the class and if someone walks on his right side he does not always hear them so we walk on his left side and everyone who needs to know about his hearing loss is informed.”—Parent of a 14-year-old male reported to have a moderate binaural hearing loss due to childhood otitis media at age 4 years
“I am always second guessing if she hears well enough in school or well enough to make progress with her disability and speech delays.”—Parent of a 16-year-old female with otitis media up through age 11 years, requiring PE tubes. She has hearing loss in low frequencies and is described as having moderate hearing loss
“Hearing loss has affected every aspect of her life. We can understand only part of what she says. Some words no one can understand, not even her speech and hearing teacher.”—Parent of an 8-year-old female with a reported moderate hearing loss
“Hearing loss had dramatic negative effects on my daughter’s social development, making and keeping friends, and generally feeling good about herself. Professional at the time said there did not appear to be any reason for the hearing loss, that she just could not hear, and that a hearing aid would not help. Her hearing loss isolated her almost completely. She received classroom adjustment, but in the end she dropped out of school then dropped out of job corps.”—Parent of a dependent (age unknown) with profound hearing loss in one ear
“I noticed I had to yell really loud for him to hear me if I were to ask him a question. A lot of time nobody wants to talk to him because, if they don’t talk loud, then when they ask him a question and he can’t hear so he doesn’t answer them and they think he is ignoring them. Have not sought any solution for child’s hearing. Doctor said he could adjust. Maybe a wax build up. He would check it at a later date. I don’t think my child would be comfortable with a hearing aid in his ear. He might lose it.”—Parent of a 4-year-old boy described as having a moderate hearing loss and an inability to hear normal speech across a room
“I believe it has not affected his life at all. He couldn’t miss what he never knew he had.”—Parent of a 16-year-old male having ear infections at 2 years old requiring removal of eardrum and 2 of the 3 bones in his middle ear (reported her child was found to have a slight hearing loss)
“She grew up with the hearing loss. Knows nothing different.”—Parent of an 18-year-old female with CMV virus when born, leading to total deafness in one ear
“We have to talk louder or directly to him. He keeps his music and the TV turned up too loud for my comfort. My son is an avid gun user and hunter. He is on the rifle team in ROTC. He did a lot of target shooting without head gear, so the frequent loud noise in his ear caused hearing loss.”—Parent of a 17-year-old male with moderate hearing loss
“My son was in the 5th grade and they had a school check-up. He did not pass and I received a note to get a 2nd check-up, and that’s when it was noted that there was some hearing loss. Then we went to an audiologist and it was noted that he had a great hearing loss, but my spouse put it off and stated that he would grow out of it as he got older. This year I took him again for a regular check-up on his ears and it was noted again, but it was a lot worse and if he doesn’t get the hearing aid soon it’s going to be too late. But now he is going into the 8th grade and does not want to wear a hearing aid at this time.”—Parent of a 14-year-old male with severe hearing loss
“By age 4 she was not talking right, I got her checked out, and it was found that when her dad had her for visitations he would let her play in toxic water and thus she was always having ear infections every other week. She’s very quiet and keeps to herself. She has to miss classroom activities to go to speech therapy to help her learn to speak on the level she should be at. She is also behind in reading because of everything.”—Parent of a 9-year-old female with moderate hearing loss

|
| TABLE 5. Reasons why children or dependents with hearing loss do not use hearing aids (in %).(Click to view as pdf) |
“My daughter had a lot of ear infections and had her tonsils and adenoids removed. She is very hard of hearing. I started noticing that when she was in school. While sleeping she is hard to arouse. It seems to affect how my daughter catches on to things such as school. She does not use hearing aids because it doesn’t seem to be that terrible and seems something that can be dealt with.”—Parent of a 14 year old female with moderate hearing loss who cannot hear normal speech across a room
“My life is only affected because my daughter’s feelings get hurt and I’m told her hearing loss isn’t severe enough. She speaks very loud, can’t hear TV, can’t concentrate with background noise and is very self conscious about her speech. Her school work suffers because she can’t hear the instructions, but she passes the school hearing test.”—Parent of a 9-year-old female with moderate hearing loss
Why Hearing Aids Have Not Been Used
Sixty-one possible reasons for not getting hearing aids were listed in the survey. Referring to Table 5, parents were asked to rate whether or not any of the 61 reasons impacted their decision not to have their dependent fit with hearing aids. For each reason, parents were asked to rate on a three-point scale whether the reason was “definitely,” “somewhat,” or “definitely not” a factor in their decision. These ratings have been collapsed into 10 general categories in Figure 2. The top three reasons for non-adoption of hearing aids are “minimization of hearing loss” (84%), “recommendations from a professional” (80%), and “degree or unique nature of hearing loss” (76%).
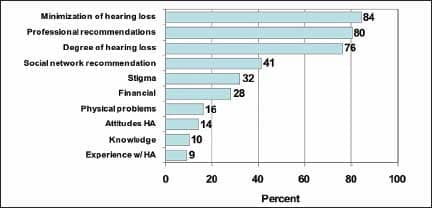
|
| FIGURE 2. Reasons why children with hearing loss do not use hearing aids (see details in Table 5). |
Minimization, Denial, or Neglect?
A review of Table 5 suggests that the majority of respondents had dependents with very mild hearing losses that do not require amplification (hearing aids, FM, sound field, etc) according to a recognized professional. When we combine this information with parental perceptions of their quality of life, and the letters we received from parents, there is a reasonable doubt that these dependents all have a benign hearing loss or a hearing loss that is untreatable with amplification. Many of these responses are indicative of minimization of the hearing loss or denial. Examples of these parental comments follow:
“Kept saying ‘what’ at a young age of 4. Doctor said it may get worst or better not sure, but so far stayed the same. She was in special education so school was OK most of the time. At school she sits up close. Music, TV and games she turns up loud. Did not get hearing aids because doctor said it wasn’t bad enough.”—Parent of 20-year-old female described as having a moderate hearing loss in one ear
“The hearing loss was discovered from my daughter’s speech. She doesn’t talk as well as she should. The family doctor has her going to Easter Seals for speech. Hearing testing was mild but not real bad hearing loss.”—Parent of 4-year-old female with mild hearing loss
“When you talked to him, he wouldn’t answer you or he would say, huh? You have to repeat what you say to him. The teacher sets him closer up front of the class. He does not have hearing aids because his hearing isn’t that bad yet.”—Parent of 8-year-old child, with hearing loss described as moderate and inability to hear normal speech across a room
“I believe it was first noticed when he looks at television he sits directly in front of it and it is sky high in volume. I now think it’s a minor hearing loss in one ear rather than both. I know the family members are always saying he can’t hear. A lot has to do also with he doesn’t pay attention.”—Parent of 6-year-old child, described as having moderate hearing loss and inability to hear normal speech across a room
“Had some difficulty with phonetic based hearing program when in kindergarten and first grade. This hindered confidence in performance in language arts and is still 3 years behind peers. The reason for not using hearing aids is hearing loss is very mild at this time but will be monitored by physicians.”—Parent of 14-year-old boy with mild hearing loss
“She has requested seating at the front of the room in school in some classes. She will turn the TV up to a point where it is almost uncomfortable to others. Surgery repaired the rupture to her ear drum and she just lives with the mid to moderate hearing loss. Her hearing loss is not severe enough to warrant hearing aids.”—Parent of 14-year-old female with infection as a child, ruptured eardrum, and subsequent scarring from surgery, described as having a moderate hearing loss
“If she is in a room next to the room I am in, I have to shout or use the phone to call her. If she is in the same room, I have to speak loud and slow. I do not think her hearing is bad enough to warrant hearing aids.”—Parent of 15-year-old female with mild hearing loss and inability to hear normal speech across a room
“The school audiologist told me it was a genetic defect and her hearing was comparable to a 70 year old person.”—Parent of 7-year-old female with bilateral mild hearing loss requiring front-row seating with attempts to get her FM at school
Degree of Hearing Loss and Professional Recommendations
Often parents’ decisions not to explore hearing aids for their dependents are based on the advice of pediatricians, audiologists, family physicians, or otolaryngologists. Some parents received conflicting information from two or more professionals. However, some of the advice would appear to be misinformation.
Some professional reasons for not getting hearing aids are that hearing aids would not help the dependent with high frequency hearing loss (21%), low frequency hearing loss (22%), or unilateral loss (42%). Only 14% of parents indicate that their dependent’s hearing loss was too severe for hearing aids and, in fact, a content analysis of letters from parents indicate that only 8% of the dependents had one or two ears without residual hearing.
Comments from parents regarding the recommendations they received from professionals for management of the dependent’s hearing loss follow:
“Basically my child hears very loud sounds; if you are talking to her in a low pitch voice she would not understand. The ENT said she needs to have her tonsils removed because this is affecting her hearing. Sometimes it gets to be a little upsetting to keep repeating the same thing over to her. The doctor informed me to try and speak to her facing her and use a lot of mouth movement so she will be able to read my lips. My daughter has to listen to the TV at least 5 volumes louder than me. Hearing aids were never offered to my dependent. I don’t think her problem is that severe at this time. The doctor stated I shouldn’t worry; there is a lot of people like her.”—Parent of 11-year-old female with moderate hearing loss
“Both the audiologist and the ENT felt they were not necessary at this time even though she plays radio very loud and TV as well.”—Parent of 16-year-old female with otitis media up through age 11 years requiring PE tubes. Has hearing loss now in low tones and described as having moderate hearing loss
“When my son was about 7, I had him developmentally tested. This was just a precaution as a result of home schooling. He failed the hearing exam. We were referred to an audiologist who also failed him. So we went to his pediatrician. She tested him again in the office using her little machine, which she swears is very accurate. Her test came back with no problems whatsoever. My son is now 10 and he still complains of not being able to hearing some things. The only thing [the pediatrician] did, however, is to keep testing him with her machine and nothing ever comes back bad, and she has refused on two different occasions to give me a referral to go back to the audiologist. She also has stated that he’s just a boy, and he’s probably ignoring us, or even having selective hearing. The reason for not getting amplification is his doctor does not acknowledge he has a problem.”—Parent of 10-year-old boy with a reported mild hearing loss who cannot hear speech across a room; has had behavioral problems at school and difficulty with family relationships
“Couldn’t understand anything she said. Doctors said was nothing to worry about. When she still could not be understood at the age of 4, we knew she needed help. Her doctor still would not help us. She started Pre-K, and the teachers and counselors requested that she be tested. That’s when we were able to get her help. We have sought all methods of help with her hearing. All the doctor specialists, audiologists, and other experts, have told us hearing aids will not work for her. She has no damage to her eardrum. She has a blockage in her ear canal. They will not do surgery. She has been in speech and hearing classes from Pre-K to first grade. She is going into 2nd grade and her speech has improved but not her hearing”—Parent of 8-year-old female with moderate hearing loss who can not hear normal speech across a room “At approximately 18 months of age I noticed my daughter walked like a drunken sailor. She did not respond if I stood behind her and talked to her. I took her to our pediatrician’s office. At first he brushed me off. I persisted until he did a basic audio test. She was flat line—the test would have had a bell curve if she could hear. He referred me to an ENT doctor.”—Parent of 9-year-old female with mild hearing loss requiring speech therapy
“My son started complaining about feeling pressure in his ears. It often hurt. Took him to a pediatrician for ear infections. Time and time again nothing. Pediatrician said he will have to learn to deal with pain. I took him to an ENT who said there was a problem and referred to a specialist. After MRI and CAT scan, it was determined that there was no abnormalities in the ear canal. Not knowing what caused it, they have no way to fix it. He is still being tested to make sure he doesn’t loose hearing in the other ear.”—Parent of 17-year-old describes his unilateral hearing loss as profound in that he can only hear shouts across a room
“I was concerned because Steven wouldn’t turn to look when a loud noise was made. The pediatrician referred us to have his hearing tested, and they say he is hearing within normal ranges. He still does not seem to hear well. For awhile he had fluid in his ears, but now it is gone. He still has a speech delay.”—Parent of 11-year-old male with mild hearing loss now home schooled by parents and described as introverted
“My son was having a speech problem at age 3 and the doctor wanted to check all aspects; he was found to have a high frequency loss in his left ear. The doctor said hearing aids would not help this type of hearing loss.”—Parent of 18-year-old male with high frequency moderate hearing loss requiring school adjustment and speech therapy most of his childhood
“My son had an ear infection when he was 5 years old that his doctor left untreated. I believe that he should have been treated with antibiotics. He now has major hearing loss. I noticed because he only uses his left ear to talk on the phone and he turns his head when someone is speaking to him. At this time we do not know if he needs a hearing aid; however, if he needs one, we would get one.”—Parent of 7-year-old boy with severe hearing loss believed by parent to be the result of ear infection at an early age
“Loss of high pitch in left ear and was told only old farmers have had this hearing loss. Nurse in school informed me. Was told that hearing aids would not help. He adjusts himself if unable to hear.”—Parent of 14-year-old boy with high frequency hearing loss
“The reason for no hearing aids was the audiologist said it probably wouldn’t help with his bilateral hearing loss and that he was growing and hearing aids would need to change frequently.”—Parent of high-school age male described as having profound hearing loss in both ears
“She started getting sick to her stomach. Her pediatrician doctor said that she couldn’t find anything wrong with her. So I changed pediatrician doctors, and this other one checked her from top to bottom and noticed her left ear was full of gunk. So went to an ear doctor [and] got treatment for it. After treatment, noticed hole in her ear. He tried patching it up and that didn’t work. He put tubes in ears. The tube in her left ear and she had to get that removed. She had to wait for the hole to close up. Then she still couldn’t hear well enough in that ear. So, he went in to reconstruct the eardrum. Still didn’t do anything for her hearing, so we are going in every 3 months for treatment. She does not use hearing aids because she can still hear from her good ear, and her doctor thinks she will improve over time.”—Parent of 17-year-old girl with moderate hearing loss unable to hear normal speech across a room
“In pre-kindergarten she was tested and failed the school hearing test. We immediately sought the advice of her pediatrician, who retested her. She failed the second test and we were asked to go to a specialist. The specialist did a series of tests and determined that her hearing loss was minor and that a hearing aid would be too costly for us when she really didn’t need one yet. The specialist suggested yearly reviews to track the problem. If the day comes when she will benefit due to more loss of hearing or new technology, then we will fully investigate our new options and make an informed decision.”—Parent of 10-year-old female with bilateral hearing loss described as mild
“Because of several ear infections, she has to have PE tubes inserted in both ears. After second pair of tubes came out we noticed that she sat up close to the television, played it and the radio very loud, and talked extremely loud all the time. Although we had her hearing tested, her ENT does not think there is any hearing loss. But now, at the age of 8, we have never heard her talk softly or low. School performance is good, but have reports that she talks too loud in class. I can’t really be sure that there is a hearing loss.” —Parent of 8 year old with moderate hearing loss
“Discovered hearing loss in 4th grade by teacher who suggested a hearing test. The audiologist diagnosed that there is some loss in both ears, more in the right. “Th” and “ch” sounds are not heard. Asked for an annual check-up. Aids would not make a significant difference at present times.”—Parent of 15-year-old female with moderate high frequency hearing loss
“Our daughter attended a preschool screening and the audiologist noted a hearing loss in her ear. She had exhibited some speech irregularities that could be attributed to developmental or learning loss. The on-site audiologist recommended a consultation at the health department and then on to a specialist. The specialist did initial exams and retested her hearing. He stated she had a 65-70 percent hearing loss in her left ear. She had great hearing in the other ear. Her hearing loss would probably need to be monitored annually. She would probably exhibit loss in crowds. It has impacted her school performance via grades. The older she gets, the less she desires to draw attention to something she doesn’t know. No changes have occurred in her hearing loss so we have sought no adjustments. We were initially told that hearing aids wouldn’t help her in classroom or crowd situations.”—Parent of 15-year-old female with severe hearing loss in one ear
“Doctors told us that hearing aid would hinder her as they would pick up so much background noise and then that would confuse him or make it worse.”—Parent of 20-year-old male with 80% hearing loss in one ear described as moderate hearing loss
Stigma
As noted in Table 5, about a third of parents indicated that the stigma associated with hearing aids impacted their decision not to pursue hearing aids for their dependents’ hearing loss. Some physicians concurred that the stigma of hearing aids outweighed the benefit.
In rank order, parents indicated hearing aids would make their dependents or themselves embarrassed (22%); there was an aversion to wearing the devices in front of friends (20%); peers make fun of the dependent with hearing aids (19%); people will treat the dependent differently (19%); they are too noticeable (18%), and/or make the dependent look disabled (17%) or mentally slow (14%).
Here are some examples of parental and dependent comments regarding the stigma attached to wearing hearing aids:
“The stigma attached to wearing a hearing aid has been negative for C___. She does not like to admit there is anything wrong. It’s not cool to wear a hearing aid in her opinion. Hearing aids are really only for old people.”—Parent of 21-year-old female who had childhood ear infections
“As a high school student she doesn’t want that stigma of wearing a hearing aid. Her hearing loss has not affected her schooling, friendships, etc, that greatly.”—Parent of 16-year-old female with ear infections, adenoid removal, PE tubes, and eardrum perforations requiring surgery that did not heal properly. Described as moderate hearing loss by parent
“They [hearing aids] are ugly, don’t work in crowds, are too noticeable. I do fine without them.”—21-year-old male described as having a severe hearing loss in one ear. Hearing loss first became noticeable when talking on the phone. Reported to have mixed hearing loss.
“Kids made fun of me. I lost them [the hearing aids] frequently on the playground or left them in my pants so they got washed.”—17 year old with severe high frequency hearing loss, who was fitted with hearing aids in 3rd grade and refused to wear them
“His hearing loss is not too severe. He has special seating in school which helps him pay attention more. It’s difficult with new relationships. We must tell people to speak to him face-to-face or on left side. Family was saddened by many surgeries but we speak slow and clear, and louder than normal. He gets very frustrated often. He doesn’t want hassle at this time with hearing aids. Maybe when young adult he may change mind.”—Parent of 8 year old described as having moderate hearing loss in one ear
“Teacher and audiologist didn’t want to make him uncomfortable with learning and made suggestion that, as long as the special seating in classroom was helping, then a hearing aid would not be needed.”—Parent of 18-year-old male with mild hearing loss in one ear and moderate in the other
“The doctor told me, after taking a hearing test, that hearing aids would only worsen my problem. Though, even if hearing aids were an option, I would feel uncomfortable wearing them due to the affect it would have on other people and their opinions of me, the way they would view my competency, etc.”—20-year-old female with severe hearing loss due to scarring of the eardrum as a result of childhood ear infections
“The doctor indicated that hearing aids were not an option since her hearing loss wasn’t serious enough to put him through self-esteem problems at this time. He speaks very loudly and can tend to get in trouble at school because of it.”—Parent of 9-year-old male with a 10% loss in his right ear due to damage from prolonged high fever
Financial Considerations
Nearly 3 in 10 respondents indicated that financial or value considerations impacted their decision not to get hearing aids for their dependent; 22% indicated they could not specifically afford hearing aids.
“We have not gotten hearing aids. I did look into them. The cost was none that I could afford. But he has done very well without them.”—Parent of 14-year-old dependent with otitis media at age 4 and 8 years, and previous surgeries for PE tubes
“Insurance does not cover cost and doctor has not recommended.”—Parent of 14-year-old boy with moderate hearing loss and inability to hear normal conversation across a room
“We stopped at a hearing store one day when she was about 7 or 8 years old. They were offering free testing. Laura threw a big fuss at first but finally agreed. We were told her loss was about 20% in her right ear and 35% in her left ear, but our insurance didn’t cover the devices then, and she hated the idea so much we decided not to buy them.”—Parent of 16-year-old female with otitis media as a child believed by parent to result in eardrum scarring and hearing loss
“Do not buy hearing aids mostly due to the high cost and we can’t afford them. I hate to deny his need of them if we can’t afford them. We have a hard time paying bills, but yet we never seem to qualify for financial assistance because we make too much money.”—Parent of 8-year-old male with moderate hearing loss according to parent
“First, hearing aids are too expensive. The audiologist said I would eventually need one.”—21-year-old female with moderate hearing loss and difficulty hearing high frequency sounds and especially speech in noise. Problem found in elementary school and main intervention was front of class seating
“When we moved to El Paso, the doctors have told us that the problem was a minor one and did not require any medical treatment or hearing aids. It is my opinion that the military did not want to pay to look at her and this is why were told it was a minor problem. We will be transferring to Hawaii and were told that they have a better track record and will actually try to help our dependent to hear.”—Parent of 7-year-old female with bilateral mild hearing loss requiring front-row seating with attempts to get her FM at school. The school audiologist told the mother it was a genetic defect and her hearing was comparable to that of a 70-year-old
“I do not like the way they look in people’s ears and some are so expensive too. It affected my child’s performance at school because she would have to lipread to understand what the person is saying to her.”—Parent of 6-year-old female with moderate hearing loss unable to hear speech across a room
“It is simply a matter of money. I’m on SSI and cannot afford hearing aids for my daughter. She cannot communicate viably and therefore other children and sometimes their parents look at her as mentally disabled when, in fact, she has a very high intelligence and has learned to communicate with some sign language and pointing much like playing charades.”—Parent of 3-year-old female with moderate hearing loss with aphasia speech disorder; she cannot hear normal speech across a room
Other Considerations
Some dependents had other significant physical or developmental problems (16%) believed to exceed their hearing loss problem. Only a minority of these dependents did not purchase hearing aids due to negative attitudes (not including stigma) concerning the product (14%), or lack of knowledge concerning hearing aids or where to go to get audiological testing (10%). Less than 1 in 10 (9%) had tried hearing aids.
Discussion
Optimum communication access by children—not just in the classroom—is critical for language competence, cognitive development, social and emotional well-being, academic competence, and ultimately, development as productive citizens.2 When communication access is denied through misinformation, minimization, neglect, stigma, or where there are financial barriers to communication access, then it is likely that children with untreated or undertreated hearing loss may eventually join the ranks of adults with untreated hearing loss, leading to lives of underperformance and broken dreams.
The literature is quite clear that untreated hearing loss affects nearly all dimensions of the human experience.4 And the pediatric literature is quite clear that even children with “minimal” hearing loss are at risk academically compared to their normal-hearing peers.5-12
When we review the survey data and parental commentary in this study, it is evident that the majority of these children and dependents do not have benign or trivial degrees of hearing loss. There is little evidence in this study that these children received hearing aids, FM, or soundfield amplification in the classroom. The main school intervention in this sample was front-row seating in the classroom.
Why are only a minority of children or dependents in America with hearing loss recipients of amplification, and what can be done in the medical and hearing health profession to make sure that all children have received adequate help for their hearing loss? A recent CDC sponsored workshop6 on mild and unilateral hearing loss identified a number of areas for improving America’s hearing health care system for dependents. Drawing on the recommendations from this study, as well as the findings in the current study, some key issues for improving hearing health care for dependents are summarized below.
Prevalence of Childhood Hearing Loss
The prevalence of hearing loss in the MarkeTrak VII study for children under the age of 18 is approximately 1.67%1; by comparison, the CDC, using similar methodology in 1991, reported an incidence of 1.8% for dependents under age 18.13
The CDC and MarkeTrak surveys evaluate hearing loss subjectively. However, some local estimates place the figure of hearing loss among children as high as 11% based on on-site objective audiological testing.12 At a national level, other researchers estimate that nearly 15% of children may have either a low- or high-frequency hearing loss of at least 16 dB.14 They further estimate that 12.5% of children show evidence of noise-induced hearing threshold shifts in one or both ears.15 Given these latter estimates, based on objective hearing loss measures, then conceivably the number of children and dependents with untreated hearing loss could be significantly greater than that reported in this study.
Use of Amplification
The low incidence of amplification in the pediatric population, whether by hearing aids, FM, or soundfield, would appear to be due to the following:
- Audiological pediatric protocols emphasize that hearing aids are for children with significant hearing loss.16 Although the impact of untreated hearing loss for mild and unilateral losses has been well documented, these losses tend to be relegated to “special considerations” in existing protocols, ensuring that parents will not be given strong guidance with respect to optimizing their dependent’s communication access.16
- Parents may be receiving misinformation from both medical doctors and hearing health professionals with respect to amplification candidacy, especially as it pertains to high frequency hearing losses, unilateral losses, and current and post-otitis media care where there is evidence of permanent hearing loss. A second explanation is that parents do receive accurate information concerning the children’s hearing loss but misunderstand it.
- Undoubtedly, parent’s statements regarding the severity of their child’s hearing loss had its origins in professional opinion. In fact, the medical and academic consensus view is that a hearing loss below 35 or 40 dB in the better ear is considered “mild.” Yet, we know that, for a child in a classroom, this is worse than stuffing their fingers in their ears. Objective measures of candidacy for amplification would appear to support treatment for those children whose hearing losses exceed 35 or 40 dB. Many times it would appear that the decision to treat the child is controlled by a local pediatrician who is not expertly trained in the issues of hearing health care.
- It is perplexing why ENT and audiological professional recommendations to the parent often included only front row seating in a classroom as a treatment objective during the child’s school years.
- Where there are objective results from an audiologist on a dependent’s hearing loss, pediatricians at times dismiss or minimize those results. In fact, a recent study17 determined that 59% of children failing an audiological screening performed at medical clinics were not referred for follow-up to an audiologist by pediatricians. Since this study was conducted in 8 medical practices, results cannot be generalized to the entire pediatrician population; yet it serves to illustrate the possible deficiencies in pediatrician protocols for identification, referral, and treatment of childhood hearing loss. A national study of pediatrician practices would be of value in shedding light on this important topic.
- One third of parents report that hearing aids were not adopted due to stigmatization of either themselves or their dependent. At times, the medical doctor, audiologist, or teacher agreed that the benefits did not outweigh the stigma or impact on the child’s self-esteem, and therefore recommended against hearing aids for the child. While parents’ final decisions are to be respected by the professional, the parent should be acutely aware that using stigma as a reason for not addressing their child’s serious communication deficits may not be in the best interest of the child, and is likely to result in reduced academic, social, and physical status. Using such labels as “mild hearing loss” gives the parent a convenient out in addressing their dependent’s hearing loss. Clearly, counseling protocols that handle the concerns of the parents regarding stigmatization of their dependent, while adequately informing them of the consequences of undertreatment, is necessary.
- Three in 10 parents indicate they either cannot afford or question the value (eg, benefit relative to cost) of hearing aids. In a country as financially advanced as America, no dependent should be denied equal access to communication due to financial considerations. State and local social service and educational programs (eg, IDEA legislation), not to mention medical insurance programs, should extend coverage to all dependents with hearing loss. It would appear that existing programs are designed to administer only to the hearing needs of the minority of dependents—that is, those with more severe hearing losses.
-

- • Cochlear Implants and the Education of the Deaf Child, by Ann Geers, PhD, May 2003 HR.

• Newborn Hearing Screening Follow-Up: The Essential Next Step, by Michael Primus, PhD, January 2005 HR.
• Parent Involvement: The Magic Ingredient in Successful Child Outcomes, by Karen Anderson, PhD, November 2002 HR Archives
Infant Hearing Loss Screening
Although more than 90% of infants in America are now screened for hearing loss at birth, historically only half of parents come back for more detailed audiological testing in a timely manner—some as late as age 3 years, when the dependent is already experiencing severe language development problems; recently this has improved to 66% follow-up.18 Clearly, audiological advocacy after infant screening could be strengthened by more robust follow-up efforts that might include state-centralized coordination/assistance in tracking these infants, involvement of Public Health and WIC (Women/Infant/Children) nurses, or virtually any other means available for getting these infants to return for testing.
Admittedly, in a subjective study, based on the survey responses and commentary of 225 parents of dependents, it is difficult to form definitive conclusions on the state of hearing health care for America’s children and older dependents with hearing loss. But we believe the data is sufficiently strong enough to raise some serious questions:
- In determining which child should receive amplification for his/her hearing loss in an educational setting, is there a systematic bias towards those children with serious or profound degrees of hearing loss?
- Is the prevalence of treatable hearing loss among children under-represented in the United States when subjective methodology is used to assess hearing loss?
- Are pediatricians sufficiently trained to measure hearing loss in children and to advise parents on treatment options?
- Do educators, physicians, and hearing health care professionals minimize the impact of mild and unilateral hearing loss on children?
- What can be done to assure timely follow-up for infants failing infant screening tests?
- How do parents form erroneous beliefs that certain types of hearing loss—such as high frequency hearing loss—cannot be helped with amplification when scientific evidence clearly states otherwise?
- In the event that they cannot personally pay for their children’s hearing aids, do parents have viable options to obtain the devices? In cases where financial aid may be available, how is that information transmitted to the parent?
- Is there a way that the stigma of hearing aids could be mitigated in the schoolroom when it is determined that a child needs hearing aids, especially given the critical need in terms of academic performance and language development? Can vanity on the part of either the parent or dependent be allowed to serve as a barrier to communication access in the classroom?
- Is there a sizable population of young people in America being left behind because they do not fit existing paradigms of hearing disability?
Acknowledgement
This study was made possible by a special grant from Knowles Electronics Inc, Itasca, Ill. Knowles has been funding the MarkeTrak studies since 1989.
References
- Kochkin S. MarkeTrak VII: Hearing Loss Population Tops 31 Million People. Hearing Review. 2005; 12(7):16-29.
- Johnson C. What Parents Should Know: The Educational System. In: Luterman D, ed. Children with Hearing Loss: A Family Guide. Sedona, Ariz: Auricle Ink Publishers; 2006.
- Schein JD, Gentile A, Haase KW. Development and evaluation of an expanded hearing loss scale questionnaire. National Center for Health Statistics. Vital Health Statistics. 1970;2(37).
- Kochkin S, Rogin C. Quantifying the obvious: The impact of hearing aids on quality of life. Hearing Review. 2000;7(1):8-34.
- Northern JL, Downs M. Hearing in Children. 5th ed. Baltimore: Lippincott Williams and Wilkins; 2002.
- National Workshop on Mild and Unilateral Hearing Loss. Breckenridge, Colo, July 26-27, 2005. Sponsored by the Centers for Disease Control and Prevention, Early Hearing Detection and Intervention Program, and Marion Downs Hearing Center.
- American Speech and Hearing Association. Access Audiology: Mild and Unilateral Hearing Loss in Children. 2006;5(2).
- Bess F, Tharpe AM, Gibler AM. Auditory performance of children with unilateral sensorineural hearing loss. Ear Hear. 1986;7(1):20-26.
- Culbertson JL, Gilbert LE. Children with unilateral sensorineural hearing loss: cognitive, academic and social development. Ear Hear. 1986;7(1):38-41.
- Hicks CB, Tharpe AM. Listening effort and fatigue in school-age children with and without hearing loss. J Speech Lang Hear Res. 2002;45:573-584.
- Kenworthy OT, Klee T, Tharpe AM. Speech recognition ability of children with unilateral sensorineural hearing loss as a function of amplification, speech stimuli and listening condition. Ear Hear. 1990;11(4):264-270.
- Bess F, Dodd-Murphy J, Parker RA. Children with minimal sensorineural hearing loss: prevalence, educational performance, and functional status. Ear Hear. 1998;19(5):339-354.
- US Department of Health and Human Services. Prevalence and Characteristics of Persons with Hearing Trouble: United States, 1990-1991. Washington, DC: HHS. Series 10, No 188; March 1994.
- Niskar AS, et al. Prevalence of hearing loss among children 6 to 19 years of age: the Third National Health and Nutrition Examination Survey. JAMA. 1998;279(14):1071-1075.
- Niskar AS, et al. Prevalence of noise-induced hearing threshold shifts among children 6 to 19 years of age: the Third National Health and Nutrition Examination Survey. Pediatrics. 2001;108(1):40-43.
- American Academy of Audiology. Pediatric Amplification Protocol. Reston, Va: AAA. October 2003. Available at www.audiology.com.
- Nagourney E. Childhood testing: Hints of hearing problems are often ignored. New York Times. November 8, 2005.
- White KR. Early identification of hearing loss: the best of times…the worst of times. Hearing Health. 2007;23(3):16-18.
Citation for this article: Kochkin S, Luxford W, Northern JL, Mason P, Tharpe AM. MarkeTrak VII: Are 1 million dependents with hearing loss in America being left behind? Hearing Review. 2007;14(10):10-37.