

|
, PhD, is vice president of professional relations and education at Phonak Hearing Systems, Warrenville, Ill. |
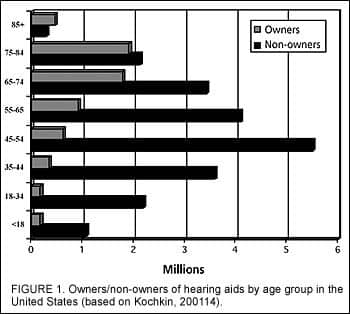
The number of patients with high-frequency sensorineural hearing loss—which may arise from noise exposure, presbycusis, ototoxicity, or combinations of these factors—is expected to increase globally, along with the age of the Baby Boomer generation, those people (ages 42-60) who were born after World War II. In the United States, 77 million people were born between 1946 and 1964, and many have acquired hearing loss due to a combination of occupational and non-occupational noise exposure. It is hard to pinpoint exactly how many patients have sloping high-frequency losses, but it is estimated that many are not wearing conventional amplification (Figure 1) due to stigma, lack of perceived benefits, and/or cost. In recent years, new hearing aid technology has focused specifically on addressing patients with these types of hearing losses.
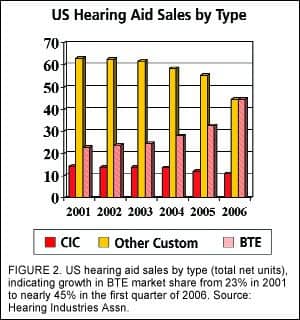
Although not a new concept, open-fitting devices have enjoyed a renaissance in popularity during the past several years. The introduction of “mini” and “micro” behind-the-ear (BTE) devices has reversed a decades-long trend of growth in the custom in-the-ear (ITE) devices in the United States (Figure 2). In 2005, most major manufacturers began offering several devices that were either specifically developed for open fitting or were modified from existing product lines. It is estimated that BTEs with size 312 or 10 batteries now constitute about 12% of the hearing aid market,1 and this may serve as a rough maximum figure for “open-fitting market share.” Whatever the exact figure, the percentage of open fittings is expected to grow in the coming years.
In order to be effective, open-fitting strategies should provide:
Minimal occlusion via a narrow (0.8 mm) tube fitting or large (greater than 3.0 mm) vented earmold or shell;
Feedback phase cancellation system;
Minimal signal processing group delays (less than 15 ms);
Precise frequency compensation with steep filter slopes;
Directional microphones to improve speech recognition in noise.
The last factor, directional microphones, has repeatedly been proven to be the single factor most related to patient satisfaction and benefit with hearing aids. Conventional wisdom, however, has suggested that open fitting and directional microphones are mutually exclusive; this is due primarily to the misconception that the acoustic properties of venting act to attenuate low-frequency gain in the frequency regions where directional microphones are most effective, rendering them useless.
Myth Directional mics are incompatible with open-fit hearing aids.
Directional microphones have proven to be one of the most significant factors related to self-perceived benefit and satisfaction with digital hearing aids.2 Consequently, the percentage of hearing instruments with directional microphones has grown steadily in recent years in the United States, and now represent 35% of the total number of hearing aids sold in 2005.1 When BTE devices are isolated, this percentage is even higher; nearly one-half (47.4%) of the BTEs dispensed last year were equipped with directional microphones.
Based on recent success, it stands to reason that directional microphone technology should extend to open-fit hearing aids. The fact that directional microphones and venting both impact low-frequency gain has led many clinicians to conclude, however, that the benefits of directional microphones will be negligible for patients with high-frequency hearing loss. Furthermore, Ricketts3 indicated that high-level environmental noise may pass through the vent, rather than the directional microphone array, in open-fit devices.
In reality, although the magnitude of benefit for open-fit hearing aids is less than that for occluded earmolds/shells, modern directional microphones do provide improved speech recognition in noise with open fittings. Despite the innovations provided by digital technology, much of the background evidence in support of using directional microphones with large vents was provided by research conducted decades ago when BTEs were a much larger part of the market. In other words, “past is prologue.”
Venting effects.
In 1985, Sam Lybarger4 conducted a series of measurements of various acoustic coupling strategies to investigate the impact on hearing aid frequency response. His results, summarized in Figure 3, illustrate the following:
1 mm, 2 mm, and 3 mm parallel vents attenuate hearing aid gain below 750 Hz, when compared to unvented response;
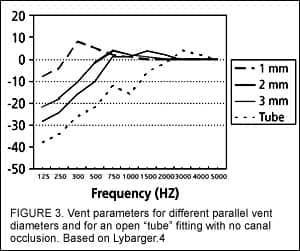
These findings suggest that, to be effective with open-fit devices, directional microphones need to provide benefits for spatially separated noises above 750 Hz for vented earmolds or 1500 Hz for non-occluding earmolds.
Directional Microphones.
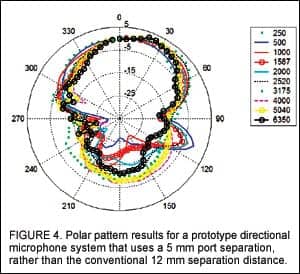
For a dual-microphone directional microphone system, the process of signal subtraction of energy received at the two microphones adds the power from the two microphones, which increases the internal noise relative to an omni-directional microphone system. Closer microphone spacing increases internal noise, but it also improves high-frequency directionality, which is critical for open fittings for high-frequency hearing losses. The industry standard port separation between microphones is 12 mm, which provides a reasonable compromise between high-frequency directionality (with benefits up to 4000 Hz) and low internal noise that is not audible to hearing aid users with mild-to-moderate low-frequency hearing loss.
Recently, a directional microphone system developed by Phonak uses a port separation of 5 mm, which is designed to improve high-frequency directional benefits through 6350 Hz (Figure 4). Directivity indices (DIs) as a function of frequency for an unvented acoustic coupling system are presented in Figure 5, revealing DIs in excess of 6 dB across the entire hearing instrument bandwidth. Obviously, reducing the low-frequency gain below 750 Hz or 1500 Hz will impact low-frequency DIs—and ultimately speech recognition in noise. However, significant benefits remain for systems that provide directionality between 1500-6350 Hz for patients with high-frequency sensorineural hearing loss.
To test this idea, a recent field study was conducted using 20 adult subjects with moderate-to-severe high-frequency sensorineural hearing loss. The subjects were fit binaurally with hearing instruments utilizing the smaller microphone port spacing (MicroSavia). Subsequently, an adaptive speech recognition threshold (SRT) in noise metric was used to evaluate the 50% recognition threshold for speech originating from 0° azimuth, with four “noise jammers” originating from 45°, 135°, 225°, and 315° relative to the midline. The average SRT in noise improvement for the aid in directional mode was 2.3 dB versus the omni-directional condition (Figure 6), translating into approximately 20-30% improvement for conversational speech.
Fact Appropriate manual or automatic program selection improves benefit and satisfaction with open-fit hearing aids.
As stated above, the concession for improved high-frequency directivity is increased internal noise, which may be audible to patients with normal low-frequency hearing sensitivity. Therefore, it is important that hearing aids (especially those with reduced directional microphone port spacing) have a mechanism for switching between directional and omni-directional mode.
Cord, Surr, Walden, and Olson5 reported that patients who were fit with instruments and who had a manual “mode” switch used their directional microphones, on average, approximately 25% of the time. This was due, in part, to confusion over when omni- and directional microphone modes would be of benefit. The authors report that those patients who persist in using their directional microphone mode eventually determine when it will be of benefit and set their hearing aids in that mode when appropriate. However, the study also suggests that the use of automatic program switching between microphone modes may minimize the impact of increased circuit noise by engaging the directional microphones only when noise is present.
The issue of automatic or manual control depends on patient preference, but the bottom line is that increased internal noise is a moot point if the patient cannot hear it. This is especially critical for patients with sloping high-frequency hearing losses and normal low-frequency hearing sensitivity.
Myth Open-fit hearing aids with omni-directional microphones provide improved speech recognition in noise by providing improved audibility.
Numerous studies have reported that, for subjects with moderate to severe hearing loss, speech recognition in noise performance may be predicted on the basis of the long-term average speech levels, audiometric thresholds, and noise spectrum levels.6,7

|

|
For patients with more significant hearing losses, hearing aid gain compensates for elevated audiometric thresholds by providing improved speech audibility and speech recognition scores, both in quiet and in noise. For open fittings, however, this advantage is less clear, because processed and unprocessed sound enter the ear canal through the hearing aid microphone and vent path, respectively.
Furthermore, with BTE open fittings, pinna and concha bowl resonances are lost for over-the-ear microphone placements. As a result, there is some evidence that speech recognition in noise performance with open-fit omni-directional microphone systems is not statistically significant from unaided performance.8
Similarly, as Figure 6 shows, a recent study on SRT in noise performance for 20 subjects with sloping high-frequency hearing loss suggests worse performance for the omni-directional microphone condition than when no hearing aid was worn at all! Interestingly, when pinna and concha resonances were partially restored via a special algorithm (Real Ear Sound used with Savia and MicroSavia), measured SRT in noise in these same patients improved to their unaided performance levels.
At any rate, there is an increasing body of empirical evidence to suggest that, at best, speech recognition in noise with omni-directional microphone open-fit devices is equivalent to unaided performance.
Myth Feedback phase-inversion completely eliminates feedback issues with open-fit hearing aids.
In recent years, digital hearing aids with feedback phase inversion have become widely available and are a primary reason behind the resurgence in popularity of open-fit devices. It is a popular misconception, however, that feedback cancellation algorithms eliminate the presence of feedback. Rather, feedback cancellation allows high-frequency gain to be preserved or increased when vent size is increased in an effort to minimize occlusion.9
In all cases, however, there are still theoretical limitations on the high-frequency gain that may be provided for various vent configurations.10 Although additional research is required on this subject, it is probably safe to conclude that a practical limitation resides in the range of 30 dB maximum stable high-frequency gain for unoccluded earmolds used with open-fit devices.
Fact Real-ear measurements (REM) are possible with open-fit devices.
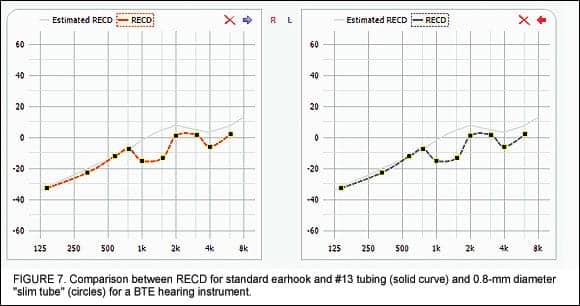
A number of manufacturers have introduced open-fit products that may be adapted from conventional BTE products by removing the conventional earhook and attaching the reduced diameter “slim tube” for reduced occlusion and improved cosmetics. Lybarger11 reminds us that reduced internal tubing diameter affects the acoustic coupling response of the hearing aid. To compensate for this, the real-ear-to-coupler difference (RECD) needs to be adjusted in the hearing aid software to reflect the impact of this change in the resonance properties from the standard (#13) tubing.
An example of this “correction” is illustrated in Figure 7. A more accurate measure of performance, however, is obtained via real-ear measurements with open-fit devices. Conventional use of insertion gain, however, is complicated by the fact that the difference between aided and unaided measurements is corrupted by sound entering through the vent path. As a result, the best way to accurately verify open-ear fittings is through measuring and displaying the real-ear aided response (REAR) on the “SPL-o-gram”.12
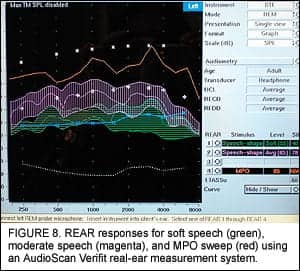
However, a more comprehensive method for verifying open-fit devices has been described by Fabry13 and is briefly summarized here. Using a broadband live or recorded speech (or speech-like) stimulus, REAR is measured for three presentation levels—50 dB SPL, 65 dB SPL, and 85 dB SPL—to ensure that soft speech is soft, moderate speech is comfortable, and loud speech and other sounds approach but do not exceed the loudness discomfort level (LDL). This is illustrated in Figure 8. For open-fit devices, the criterion for “matching” target values should be as follows:
1) Ensure that REAR peaks and minima are audible across as broad a frequency range as possible for average speech levels (65 dB SPL).
2) Match median speech levels to the patient’s unaided thresholds for soft speech levels (50-55 dB SPL). (Exception: If median soft speech levels are above patient’s unaided thresholds, do not reduce gain.)
This method will ensure that compression ratios remain as low as possible, while preserving maximum use of the patient’s residual auditory area. The use of REM verifies that the hearing aids are “acoustically matched” to individual ears, and that they provide audible speech information over as broad a frequency range as possible. Most importantly, however, this approach stresses that REMs are a starting point—not a “gold standard”— and should be used in combination with follow-up tools (eg, datalogging).
Modern hearing aids that use datalogging to monitor volume control adjustments made by the patient after the initial fitting help optimize the initial settings to meet individual patient needs. The bottom line is that real-ear measurements can—and should—be used with open-fit devices to assist with verification of initial instrument settings.
Summary
About 90% of all hearing instruments dispensed today are digital. Compared to their analog predecessors, digital instruments offer improved fitting flexibility, feedback reduction, and multichannel compression strategies to ensure audibility for soft, moderate, and loud sounds. The popularity of open-fit hearing aids has increased dramatically, in large part due to these digital factors in combination with feedback phase-inversion systems that may be used to dynamically cancel hearing aid feedback. In addition, mini- and micro-sized BTE devices offer improved cosmetics while providing minimal occlusion through the use of large acoustic vents. Although there is slightly less of a “wow” factor than with occluded shells or earmolds, open-fit devices equipped with directional microphones provide 20-30% improved speech recognition in noise compared with unaided or omni-directional conditions.
References
1. Hearing Industries Association (HIA). Special survey results on BTEs, directional, and telecoil use. Alexandria, Va: HIA; Feb 22, 2006.
2. Kochkin S. Customer Satisfaction with Single and Multiple Microphone Digital Hearing Aids. The Hearing Review. 2000;7(11):24-29.
3. Ricketts T. Impact of noise source configuration on directional hearing aid benefit and performance. Ear Hear. 2000;21: 194-205.
4. Lybarger S. Earmolds. In: Katz J, ed. Handbook of Clinical Audiology, 3rd edition. Baltimore: Williams and Wilkins; 1985: 885-910.
5. Cord MT, Surr RK, Walden BE, Olson L. Performance of directional microphone hearing aids in everyday life. J Am Acad Audiol. 2002;13:295-307.
6. Plomp R. A signal-to-noise ratio for the speech reception threshold of the hearing impaired. J Speech Hear Res. 1986;29(2):146-154.
7. Fabry DA, Van Tasell DJ. Evaluation of an articulation-index based model for predicting the effects of adaptive frequency response hearing aids. J Speech Hear Res. 1990;33(4):676-89.
8. Kuk F, Keenan D, Ludvigsen C. Efficacy of an open-fitting hearing aid. The Hearing Review. 2005;12(2):26-32.
9. Hellgren J, Lunner T , Arlinger S. Variations in the Feedback of Hearing Aids. J Acoust Soc Am. 1999;106(5): 2821-2833.
10. Greenberg JE, Zurek PM, Brantley M. Evaluation of feedback reduction algorithms for hearing aids. J Acoust Society Am. 2000;108(5):2366-2376.
11. Lybarger S. Earmold venting as an acoustic control factor. In: GA Studebaker, Hochberg I, eds. Acoustic Factors Affecting Hearing Performance. Baltimore: University Park Press; 1980: 197-217.
12. Pascoe D. An approach to hearing aid selection. Hear Instrum. 1978;12-16,36.
13. Fabry DA. Nonlinear Hearing Aids and Verification of Fitting Targets. Trends in Amplif. 2003;7(3):99-115.
14. Kochkin S. MarkeTrak VI: The VA and direct mail sales spark growth in hearing aid market. The Hearing Review. 2001;8(12): 16-24,63-65.
Correspondence can be addressed to HR or David A. Fabry, PhD, Phonak Hearing Systems, 4520 Weaver Parkway, Warrenville, IL 60555; e-mail: [email protected].



