Tech Topic: Extended Wear Hearing Aids | March 2014 Hearing Review
By Mark J. Sanford, MS, Tamara Anderson, and Christine Sanford
The InSound Medical Lyric hearing device (now owned by Sonova and sold under the Phonak brand since January 2010) was developed over the past 12 years in Newark, Calif, and was offered commercially for the first time in January 2007.
Lyric is the first hearing device that can be worn continuously in the ear canal 24 hours a day for up to 4 months. This extended wear device was developed on several key concepts:
- Sound quality improves with proximity to the tympanic membrane;
- Some people with hearing impairment resist wearing hearing aids due to stigma associated with hearing loss; and
- People want an invisible and hassle-free solution to their hearing loss.1
- There are many benefits to having a device deep in the ear canal, including2,3:
- An overall increase in gain and output, especially in the high frequencies;
- Reduction in the occlusion effect;
- Ability to use the telephone and other ear level listening devices (headphones, stethoscopes) without feedback;
- Security of fit and retention;
- Reduction of wind noise; and
- Improved localization.
Sergei Kochkin has documented through his MarkeTrak studies that the market penetration of hearing aids is approximately 25%.4 Therefore, even with all the improvements in technology during the past decade—directional microphones, Bluetooth compatibility, multiple programs, etc—the percentage of hearing-impaired people using hearing aids has not changed or, more importantly, increased. The Lyric device has the benefit of being a device placed deeply in the ear canal and eliminates the stigma of wearing a hearing device due to its invisibility and convenience.
The Lyric device received approval by the FDA to be placed by an ear nose throat (ENT) physician in 2002. In May 2008, InSound Medical received approval by the FDA that audiologists and hearing aid dispensers also could size and place the Lyric device with proper training. It also received clearance from the FDA to be worn for up to 120 days continuously by a patient.
Integrating Lyric into a Practice
The Lyric device is very different compared to fitting a traditional hearing aid. The equipment, the evaluation of the ear canal, and skills of the clinician are critical to being successful with the Lyric. In addition, the medical issues that should be considered make the learning curve substantial.
Fitting the Lyric Device
Candidacy. There are three steps to evaluating a patient for the Lyric hearing device. First, the ear canal is evaluated otoscopically to determine if a patient’s ear is an appropriate candidate for the device. Second, an audiogram is performed to determine if the patient’s hearing loss is in the fitting range. Third, the ear canal is then sized by the Lyric fitting procedure, ideally under a high-magnification microscope, to determine if the patient’s ears can accommodate the Lyric device. There are some medical conditions that are contraindications for some patients: transplant recipients, uncontrolled diabetes, radiation to head and neck, and autoimmune compromised patients.
Dispensing Models. There are also different professional dispensing models for this device. A small number of offices have an ENT to size and fit the initial device for the patient, and then the “re-fits” and follow-up care are performed by audiologists and/or hearing instrument specialists. In most offices, the dispensing professional performs the initial size and fitting, and they use the ENT as a safety net should the patient have a medical problem related to the device. Professionals fitting Lyric who use the ENT/otologist as a safety net should have an excellent relationship to manage patients when medical issues arise, which in our experience is less than 2% of the ears wearing Lyric.
An in-depth discussion of the Lyric device, including explanation of the form factor or seals, biocompatibility, mechanical design, proprietary battery, signal processing, benefits of deep canal placement including improved headroom, reduced occlusion effect, reduced feedback, and directionality by Arbogast and Whichard can be found in an April 2009 Hearing Review article.1 It also reviews clinical studies performed by InSound Medical, including improvement in soundfield thresholds, word recognition, and APHAB.
This paper details a study done on the Lyric device, equipment needed to size, fit, and place the Lyric, scheduling issues, medical issues, and business growth by one office fitting Lyric.
Otoscopic Equipment
Superior examination of the external auditory canal and tympanic membrane is the first step in fitting the Lyric. In our opinion, this should be accomplished using a microscope, or high-quality magnification loupes with a video otoscope combination. These tools are new for many audiologists and hearing instrument specialists, and they take a period of 2-4 weeks to become comfortable using (when used on a daily basis).
The otoscopic examination is the foundation for placement and successful fitting of Lyric. The bony portion of the ear canal is very sensitive, and visualizing where the medial seal should/will sit in this part of the ear canal is extremely important. Discomfort is the number-one reason patients do not keep the Lyric, and 95% of pain complaints come from this area when fitting Lyric. The discomfort or pain is almost always on the floor of the ear canal or on the lower sides of the canal wall. In some cases, the top of the ear canal by the tympanic membrane can be sore.
The upgrade in otoscopic equipment benefits the entire practice, not only Lyric patients. The microscope (or high magnification loupe) increases the perception of professionalism for the office, and it allows for safer and more precise cerumen management, as well as closer inspection of the ear canal and tympanic membrane of all patients.

Figure 1. The use of a high-quality otoscopic microscope includes high magnification, variable magnification, gold standard for ear canal examination and cerumen removal. Not only does the device improve the quality of care for all patients (including those not interested in Lyric), but it is also useful for demonstrations to patients and family members, and for staff training.
Figure 1 shows the benefit of using a microscope: high magnification, variable magnification, gold standard for ear canal examination, and cerumen removal. The drawbacks of a microscope are it is more expensive, not portable, and has a learning curve of approximately 2-4 weeks. Another nice option with the microscope is having a camera with a monitor that can be seen by the patient, family members, and other staff for training purposes.
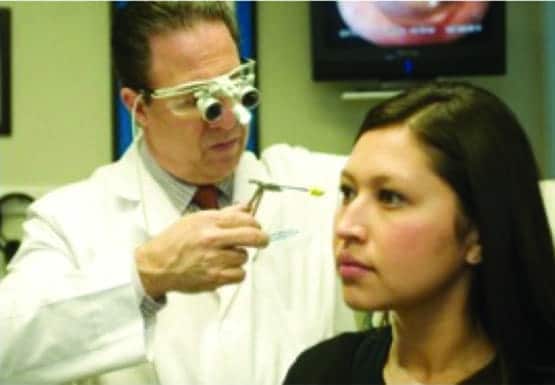
Figure 2. The use of high magnification loupes and a video otoscope combination includes good magnification and portability, and it is relatively inexpensive and easy to learn how to use. Here the clinician is using a magnification loupe to facilitate the sizing procedure.
Figure 2 shows the benefit of using high magnification loupes and a video otoscope combination. The pros of using this combination are: good magnification, portability, ease of learning/use, and less expense (if practice owns a video otoscope). The cons against the combination are: it provides only one level of magnification, you have to use two pieces of equipment, there is some potential for motion sickness in the professional using loupes, and it can end up being more expensive if the practice decides to buy both.
Additional tools that are important are various sizes of curettes for cerumen removal, nasal speculums, ear speculums, alligator forceps, Lampert speculum, and lubrication such as glycerin, MiraCell, Oto-Eze, or vitamin E oil. A suction cabinet is recommended for cerumen removal, including several suction tips of each size (3, 5, and 7 mm). An autoclave is the gold standard for cleaning instruments, though many sterilizing solutions are commercially available.
Ideally, the patients should be seated in a movable hydraulic/electric or salon chair to allow the practitioner to place them into a position that is comfortable for both patient and practitioner.
The equipment described here is a significant investment of $5,000-$15,000, depending on what the office needs and the specific equipment purchased.
Re-fits and Scheduling
The customary hearing aid evaluation for Lyric takes 45-60 minutes if you decide to test, size, fit, and counsel all at the same appointment. Approximately 5-20% of patients who are sized will need to return for fitting 5-10 days later due to sensitive skin that may appear slightly bruised during cerumen removal and/or during the sizing procedure. As a practitioner gains experience and knowledge, the number of patients who need to return for an initial fitting after bruising from initial sizing will decrease to less than 5%.
The Lyric device is sold on a subscription basis, so patients will want to be “re-fit” as soon as possible after the device ceases to function. An office will need to allow for “squeeze in” patients who need a Lyric change. A re-fit generally takes only 5-10 minutes, depending on if it is a unilateral or bilateral change. When a pattern of device longevity develops for a patient, they may decide to come in at regular intervals before a device becomes weak and runs out of power.
It is extremely important to see patients who are having pain issues immediately, and make your patients understand that you need to be informed of their ear pain issues. In our view, if an office cannot change their procedures and scheduling to conform to these unique Lyric needs, they should not choose to dispense this device.
Lyric 1 vs Lyric 2 Study
To date, there have been two versions of the Lyric device; the original model, referred to as Lyric 1, released in January 2007, and the current model, Lyric 2, released in 2012.
Lyric 2 builds upon the success of the original Lyric, as the new device is 25% shorter in length than the first device and narrower in width, moving from 6.9 mm x 5.8 mm x 16 mm long to 6.3 mm x 3.6 mm x 12 mm long (Figures 3 and 4). This change in dimensions has allowed Lyric 2 to fit more people anatomically. The latest version also reduces discomfort substantially while maintaining sound quality, ease of insertion and removal, and the invisible appearance of the original Lyric, according to an internal Phonak study in 2011-12.
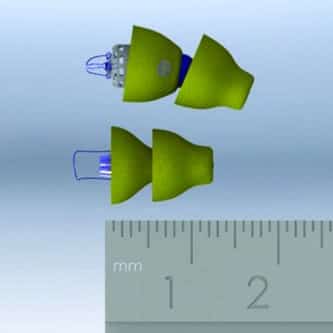
Figure 3. A top view comparison of Lyric 1 (top) and Lyric 2 (bottom).
Our office has been able to fit a much higher number of patients with the new version compared to the original. Our results are showing a fit rate of over 87% with the new version, allowing far more patients to be fit successfully compared to Lyric 1. There is a learning curve with the new version, but it appears to be far less than the original version due to the much higher fit rate.

Figure 4. A side view of Lyric 1 (left) and Lyric 2 (right)
Our study consisted of a retroactive 1-year analysis of Lyric patients in April 2013 in order to compare success rates of patients who tried Lyric 1 with patients who tried Lyric 2. The data collected included patient age and gender, duration of wear for both devices, and reasons for removal. Significant length of wear was set at 30 days, or those who completed the full trial period. For duration of wear for those currently wearing the device, the duration is calculated using the end date of the patients’ current subscriptions. Eleven reasons for removal were determined: cost, discomfort/pain, device failure, long-term break, migration/canal size problem, seeing a practitioner closer to home, deceased, preferred another device/waiting for better technology, removed for medical reasons, and no reason given.
Results
The study comparison of Lyric 1 and Lyric 2 looks at all patients who tried either device since fittings began in 2007. The total fitting numbers for both Lyric devices at the office studied were 979 patients and 1,822 ears. However, the study determined baseline use to participate in the study to be 30 days.
The group of 30-day wearers who tried Lyric 1 was comprised of 711 patients and 1,308 ears. A total of 58% were male and 42% female, and ages ranged from 13 to 104 years (average: 75 years old; median: 76). The data showed that, for the total population, 53.4% were wearing the device. This leaves 46.6% of the population having removed the device for various reasons.

Figure 5. Reasons for removal for the Lyric 1 versus Lyric 2 populations in this study. Most significant is the improvement between Lyric 1 and Lyric 2. The largest reason for removal in the Lyric 1 population was no reason given with 18.2%, followed by discomfort/pain (11.5%), preferred another device/waiting for better technology (6.5%), deceased (3.3%), cost (2.9%), seeing a practitioner closer to home (1.9%), device failure (1.3%), removed for medical reasons (0.6%), migration/canal size problems (0.4%). There were no patients who took long-term breaks. For Lyric 2, the most-common reason for removal was discomfort/pain with 5.0%, followed by deceased (3.0%), preferred another device/waiting for better technology (2.1%), no reason given (1.9%), cost (0.8%), seeing practitioner closer to home (0.5%), and migration/canal size problems (0.1%)
Figure 5 shows the reasons for device removal for the Lyric 1 population (purple bars). The most-common reason for removal among this population was no reason given with 18.2%, followed by discomfort/pain (11.5%), preferred another device/waiting for better technology (6.5%), deceased (3.3%), cost (2.9%), seeing a practitioner closer to home (1.9%), device failure (1.3%), removed for medical reasons (0.6%), migration/canal size problems (0.4%). There were no patients who took long-term breaks.
Comparatively, looking only at patients who had tried the Lyric 2 for more than 30 days, 445 patients and 800 ears were fit. A total of 57% were male and 43% female, with a range in ages from 13 to 104 years of age (average: 74 years; median: 76). For this group, 86.6% of Lyric 2 patients are currently wearing the device, a large increase from 53.4% in the Lyric 1 group.
Figure 5 also shows the breakdown of removal reasons for the Lyric 2 population (green bars). The most-common reason for removal was discomfort/pain with 5.0%, followed by deceased (3.0%), preferred another device/waiting for better technology (2.1%), no reason given (1.9%), cost (0.8%), seeing practitioner closer to home (0.5%), and migration/canal size problems (0.1%). There were no patients who removed Lyric 2 due to device failure, long-term breaks, or removed for medical reasons.
The notable drastic decrease in the “no reason given” category can be attributed to a change in technology used by InSound Medical to record information on patients. The transition from the use of the original HandFit system to the Phonak Authorized Lyric Provider System (ALPS) has made recording the reason for removal more clear and easier to access from the online Lyric database.
How Lyric Changes a Practice
Demographics. More than half (55%) of patients who have come into our practice for Lyric are new to hearing devices, which suggests that Lyric is tapping into the 75% of people who have hearing loss but do not want/use hearing devices. Three-quarters (75%) of patients who try Lyric are new to this practice, so the device provides a significant opportunity for growth of a business. These numbers are based on over 5 years and fitting nearly 1,000 patients.
Candidacy/learning curve. The learning curve for the Lyric is substantial, and a practitioner should be conservative in the beginning in choosing good candidates with healthy skin, good canal size, and within the fitting range. Practitioners can increase their success rate with Lyric as they gain experience. Our fitting rate with Lyric has been significantly higher than InSound Medical and Phonak average Lyric practitioners due to the length of time and number of patients we have fit both successfully and unsuccessfully during 5+ years.
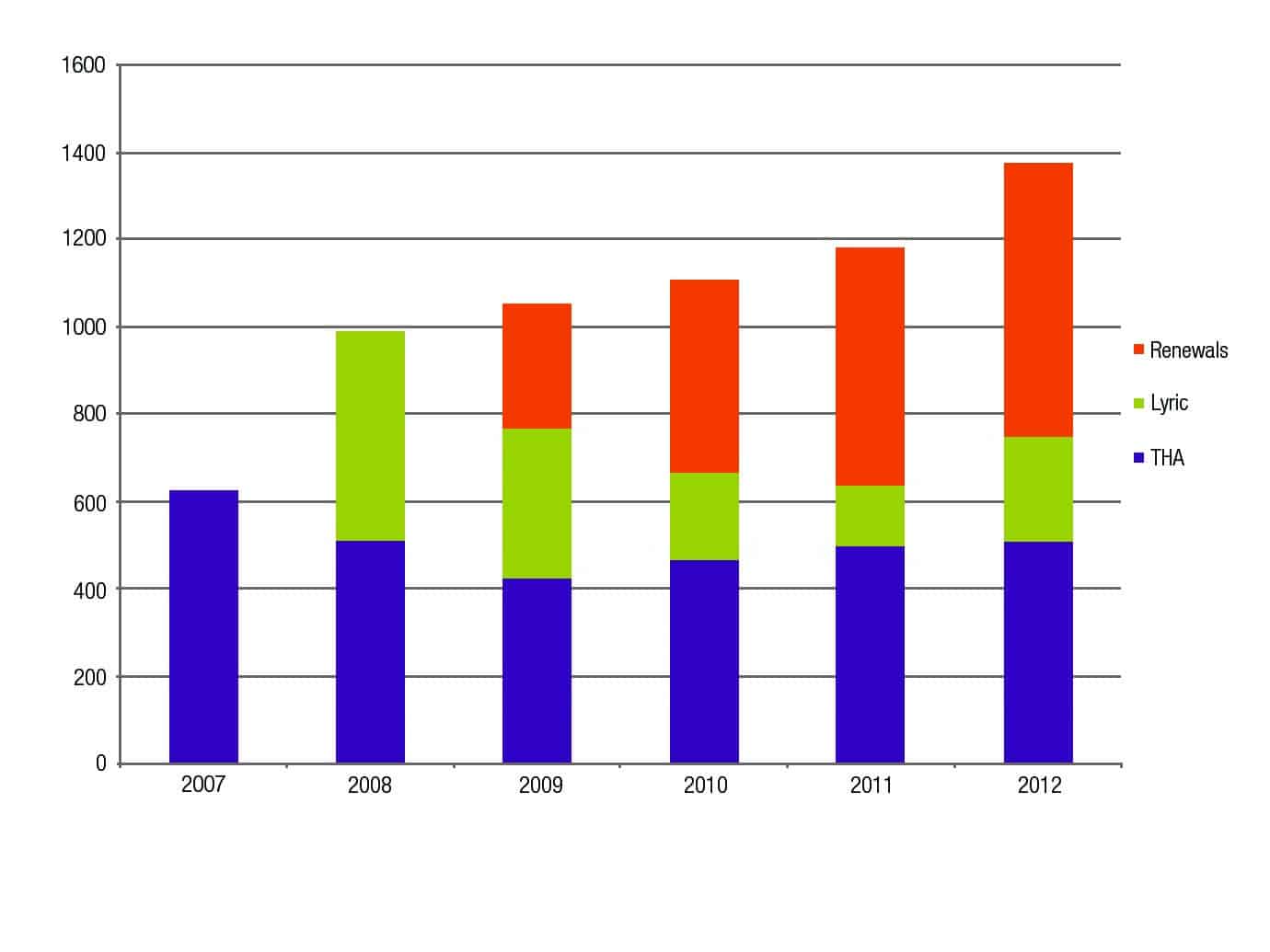
Figure 6. 2007-2012 hearing aid sales by units in this practice, showing sales of Lyric renewals (from subscriptions of current Lyric customers), new Lyric devices, and traditional hearing aids (THA).
Understanding recurring revenue and its short-term and long-term implications. Figure 6 demonstrates the units sold of traditional hearing aids versus the Lyric hearing aid and how subscription renewal increased that number to surpass the sale of traditional aids. These increases are due to the power of the Lyric to pull in new patients who want to try Lyric and the annual renewals of patients using Lyric.
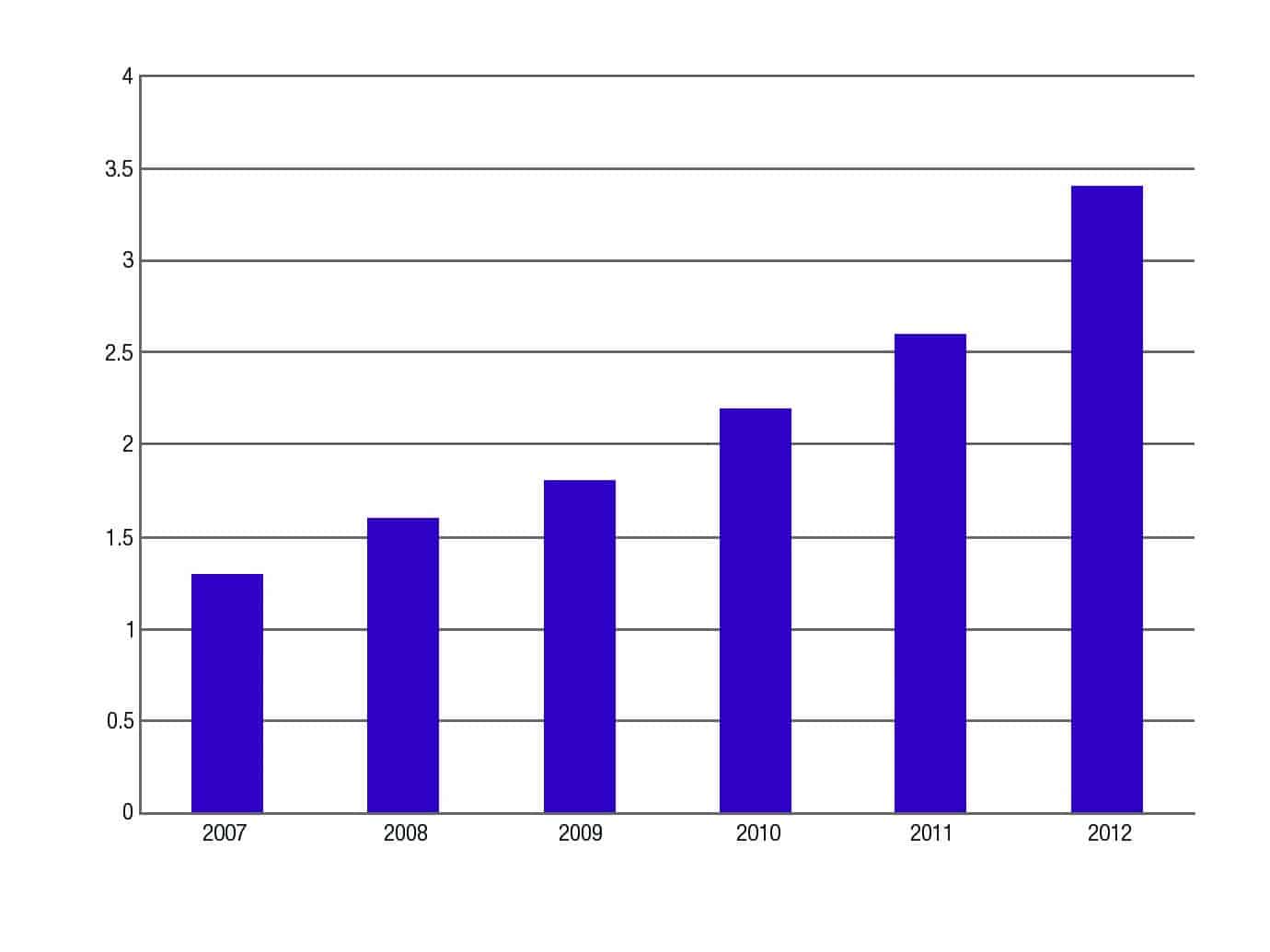
Figure 7. Practice revenues, in millions of dollars
Figure 7 shows the gross revenue increase of the practice since the introduction of Lyric, from $1.3 million in 2007 to $3.4 million in 2012. The business will grow substantially in gross revenue initially; however, because the practice will make less net profit per Lyric than a traditional device, the owner needs to understand the benefit of the recurring revenue.
Subscription model. Lyric is sold on a subscription model, meaning the cost the patient pays covers all services for a year. The subscription is usually for 1 year, and patients can buy extended years, especially if they have an insurance benefit that covers more than the cost of 1 year. There are a few patients whose devices last 120 days, but this cannot be determined in the beginning for a patient trying the Lyric. The patient’s ear adapts to Lyric over time and a fairly consistent interval of service life develops. Most patients will come in at regular time intervals to have their Lyric(s) changed for a new device(s).
Renewal rates. Renewal revenue is a totally new concept in the hearing industry, and one that along with the patient benefits of Lyric makes it advantageous for a practice to consider offering. Since the Lyric is sold on a subscription model in which a patient pays for 1 year at a time, a practice needs to know what their renewal rate will be. Our office has averaged 78% renewal rate for the second year and 83% for the third year and subsequent years. Patients who do not renew have either started going to a provider closer to where they live (due to our office being one of the first to offer Lyric, many patients drove several hours each way initially) or moved, died, or opted for a traditional device. Once most patients experience Lyric, they do not want to change to a traditional device.
Success rate. The clinician’s success rate with Lyric will improve as they obtain more experience examining the ear canal, sizing and fitting the Lyric, programming the device, and handling sizing, migration, feedback, and other issues that occur with the device. Therefore, the training and knowledge learned initially is critical to long-term success with the product. The decision to introduce Lyric into a practice should not be taken lightly.
Happy patients. The Lyric produces very happy patients. Our office manager who has been employed with us for 24 years said one day after 6 months of our office fitting Lyrics that she was frustrated because she could not remember the names of Lyric patients as easily as she did traditional device patents. She finally figured out that it was because they were so happy and they did not complain like traditional device patients about their hearing aids.
There is an interesting irony with patients who wear the Lyric: they have an invisible device, but they tell everyone about it. They say to their friends to look in their ears that they have this great new device. The hearing aid industry has been trying to be cosmetically oriented for years to reduce the stigma of wearing an aid, and now there is a device that is basically so invisible that our patients want everyone to know they are wearing a device.
Additional benefits. The Lyric differentiates an office from local and even national competitors. In many ways, the Lyric sells itself and should be introduced to all patients, especially those who will not use a traditional device. The patients who do wear Lyric provide incredible word of mouth about the device, creating a higher referral rate for the practice.
Lyric changes the office’s perception of hearing as patients are extremely satisfied, happy, and want to wear a hearing device. This is compared to many traditional device users who tend to have more negative feelings toward their devices.
We believe the relationship between the patient and practitioner also changes. The practitioner is much more involved with the patient when sizing and fitting the Lyric compared to a traditional device. This intimacy makes the patient more loyal and “tied” to the office than with a traditional hearing device that the patient can think they can get from any dispensing office.
Summary
The Lyric hearing device is a great option for hearing-impaired patients, and we believe that it is tapping into people with hearing loss who normally would not wear a traditional device. It has been fit on thousands of patients successfully who have the appropriate anatomy and hearing loss for the Lyric, and the latest version of the device has proven to fit a high percentage of ears.
However, the authors caution that dispensing professionals should understand that the learning curve with the Lyric is significant and it requires the proper training. In addition, it is imperative to have an excellent relationship with an ENT physician in the rare cases when medical examination is required. Peer-to-peer training will help in success rates initially and in the long-term with Lyric. Finally, because of its subscription model, the practice owner needs to be aware of initial renewals and the resulting implications for the business’s key performance indicators.
Acknowledgements
The data collected and views presented here are solely those of CSG Better Hearing Center which received no funding for this study. Mark Sanford has been paid by Phonak as a speaker about Lyric and conducts teaching immersions on Lyric in offices internationally.
Mark Sanford, MS, has been an audiologist for 27 years and owns 5 offices in the San Francisco Bay area. Tamara Anderson practiced as an ENT for 16 years in Russia before moving to United States, and she owned a dispensing office in North Carolina before moving to California and joining CSG Better Hearing for the past 5 years. Christine Sanford is a graduate of George Washington University, works in the art world, and does freelance writing.
Original citation for this article: Sanford MJ, Anderson T, Sanford C. The extended-wear hearing device: Observations on patient experiences and its integration into a practice. Hearing Review. 2014;21(3): 26-31.