![Out of the [Head] Shadow: A Systematic Review of CROS/BiCROS Literature](https://hearingreview.com/wp-content/uploads/2021/06/sound_waves_in_ear-1280x640.jpg)
Research | August 2021 Hearing Review
A review and summary of the literature on CROS and BiCROS systems in the past decade
By Elizabeth Stewart, AuD, PhD, and Jane Woodward, MSc
The head-shadow effect—the attenuation of signal amplitude that occurs when sound travels from one side of the head to the other—can create particular challenges for listeners with unaidable hearing loss in one ear. One effective treatment option for these clients is a contralateral routing of signal (CROS) or bilateral contralateral routing of signal (BiCROS) system, depending on the hearing status of the better hearing ear. A systematic review of relevant literature is presented to examine the benefits and limitations of CROS/BiCROS systems and highlight important clinical implications, as well as areas of opportunity for future research.
Individuals who have unaidable unilateral hearing loss (UHL)—that is, hearing loss in one ear that does not benefit from amplification, and normal hearing in the other ear—experience challenges with sound localization, sound awareness on the unaidable side, and hearing in noise and at a distance.1-3 One recent study even found that difficulty following conversations in noise and presence of tinnitus were significantly more likely with UHL compared to bilateral hearing loss.4 UHL is also associated with reduced social interaction, increased loneliness, and poorer psychological well-being.5-8 Children with UHL are more likely to repeat a year at school,9 to need support services,10 and to have an increased risk of speech and language delays.11
One solution for unaidable UHL is a contralateral routing of signal (CROS) system, first introduced by Harford and Barry in 1965.12 A transmitter is worn on the unaidable ear to pick up signals and transmit them to a hearing aid which is worn on the ear with normal hearing. A CROS system can also be configured as a BiCROS (bilateral contralateral routing of signal) for clients who have a hearing loss in their better hearing ear. Having aidable hearing loss in the contralateral ear, rather than normal hearing, adds an additional layer of complexity, as these clients must manage asymmetric hearing loss with only one aidable ear.
CROS and BiCROS systems offer a non-invasive, easy-to-use option for individuals with unaidable hearing loss in one ear with either normal hearing or aidable hearing loss in the other ear, providing benefit to the wearer by overcoming the head shadow effect to improve speech understanding. In order to understand the benefits, limitations, and clinical applications of CROS/BiCROS systems, a systematic search of literature published between 2010 and 2020 was performed. Additional objectives of this literature review included identifying any gaps in the research, as well as optimal methodologies for future research using the latest CROS/BiCROS technology.
The search focused on literature available in English retrieved from PubMed and internal sources. Relevant abstracts were appraised in terms of appropriate device, representative patient group, acceptable report/collation of data, and overall relevance to the research objectives. Full text versions of potentially relevant articles identified during abstract screening were evaluated to determine the adequacy of the study design, outcome measures, statistical analyses, follow-up, and clinical significance of the findings.
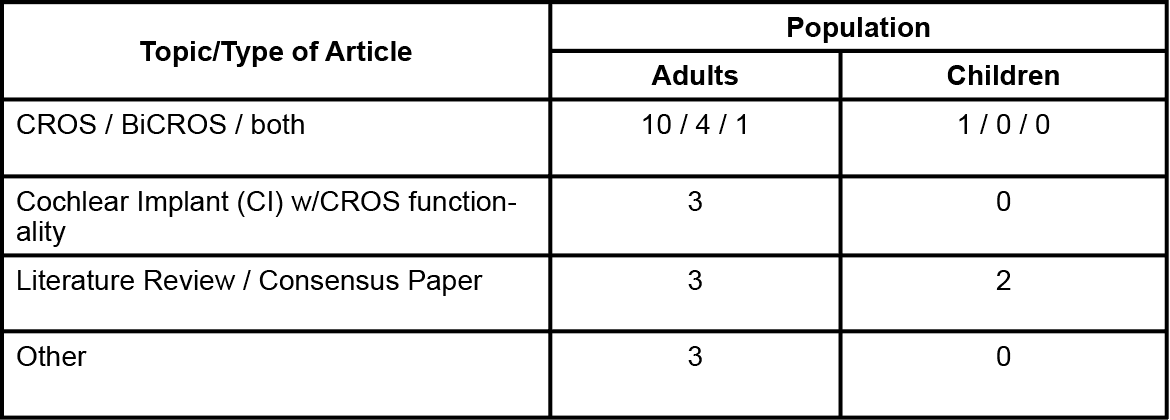
Of the 68 resulting abstracts, 36 were judged to be potentially relevant based on the screening criteria. A total of 27 articles were determined to be relevant to the research objectives, based on full text review. Outcome measures included speech intelligibility (in quiet and in noise), localization, usability, and subjective quality of hearing and/or quality of life. Further details are listed in Table 1.
Benefits of CROS/BiCROS
The literature reviewed highlighted evidence of:
- Improved speech intelligibility in noise with CROS/BiCROS, when speech is presented to the unaidable side.13-22
- Improved speech intelligibility in quiet with CROS/BiCROS, when speech is presented from the front14,20 and to the unaidable side.13,18
- Improved speech intelligibility in diffuse noise with CROS/BiCROS.19,23
- Improved subjective quality of hearing, such as ease of communication and sound quality.3,15,18,20,22,24,25
- Additional reported advantages of CROS/BiCROS systems, relative to other solutions such as cochlear implants and bone-anchored hearing devices, including usability, non-invasiveness and aesthetics.7,20,26,27
Limitations of CROS/BiCROS
In order to counsel clients appropriately, it is important to also consider any limitations of CROS/BiCROS systems. The main constraints of CROS/BiCROS found in the literature search were:
- Reduced speech understanding in noise when the noise is present on the unaidable side.13-16,19-21,23,24,28,29
- Generally, no improvement in localization performance with CROS/BiCROS.3,5,19-21,25,27 Three studies reported a decrease in localization performance with CROS/BiCROS, compared to unaided.14,16,17 It should be noted, however, that individuals with hearing loss—especially those with an unaidable ear—typically have poorer localization ability than listeners with normal hearing,16 as they are unable to perceive the necessary binaural cues with usable hearing in only one ear. Thus, no evidence of CROS/BiCROS benefit for localization was expected because contralateral routing of signal does not restore input to the unaidable ear.
What Are the Optimal Methodologies When Researching CROS/BiCROS?
The clearest benefit of CROS/BiCROS is the improvement in speech understanding in noise when the speech is on the unaidable side, while the clearest drawback is the decline in speech understanding when the noise is on the unaidable side. However, a scenario in which speech is present only on the better-hearing side and noise is present only on the unaidable side is not a common listening situation in everyday life. Rather, we typically experience diffuse noise in real-world situations. Indeed, it has been suggested that the use of diffuse rather than lateralized noise is beneficial in laboratory studies, as it creates a more realistic sound environment when measuring speech intelligibility in noise.19,29
In addition to behavioral measures of performance on speech-in-noise and localization tasks, Van de Heyning et al30 recommended the use of questionnaires designed to evaluate quality-of-life (QOL) measures, gather information regarding frequency of device use, and assess tinnitus before and after treatment (if applicable). Lastly, Bagatto et al13 advises using standardized frameworks to report characteristics of study participants with unilateral hearing loss (eg, age at diagnosis, degree of hearing loss in the poorer ear, type of intervention), and defining explicitly what constitutes a “successful” outcome when assessing the intervention’s effectiveness.
What Are the Clinical Implications When Fitting CROS/BiCROS?
In addition to some significant research findings, several important considerations when fitting CROS/BiCROS emerged from the studies included in this literature search. For example, when possible, occluding the normal- or better-hearing ear should be avoided in order to preserve monaural cues and minimize disruptions to natural hearing due to changes in ear canal acoustics.7,13 Snapp7 also noted the effectiveness of the devices should be measured objectively using a real-ear probe microphone setup and procedures for CROS/BiCROS hearing aid verification.
Other appropriate assessments—including speech-in-noise testing to quantify head shadow reduction and a needs assessment to identify the patient’s specific listening challenges—should also be completed as part of the clinical evaluation in order to determine potential device benefit.7 Counseling that targets situations in which CROS may not be helpful, such as localization or when noise is present on the CROS side, is also important, according to Bagatto et al.13 In addition, they note the use of a remote microphone system may still be warranted to improve hearing ability in noise.
Are There Any Gaps in the Research?
CROS/BiCROS appears to be relatively understudied. The results of this literature search highlight areas of opportunity for future research using the latest CROS/BiCROS technology. For example, there is some evidence to suggest that CROS solutions can improve quality of hearing, and perhaps consequently, quality of life as well,3,18 but more research is needed. Studies examining listening effort with and without CROS/BiCROS could also reveal important advantages beyond speech understanding.
Conclusions
Investigations of CROS/BiCROS benefits have revealed important improvements in listener performance and experience. The literature search also highlighted some limitations of CROS/BiCROS, relevant for counselling clients. Further reported benefits such as aesthetics, relative non-invasiveness, and ease of use make CROS/BiCROS a compelling solution for individuals with unaidable hearing loss in one ear. The opportunity exists to explore additional benefits of CROS/BiCROS technology, such as listening effort and quality of life, in future investigations.

Citation for this article: Stewart E, Woodward J. Out of the [head] shadow: A systematic review of CROS/BiCROS literature. Hearing Review. 2021;28(8):22-25.
References
- Lieu JEC, Tye-Murray N, Karzon RK, Piccirillo JF. Unilateral hearing loss is associated with worse speech-language scores in children. Pediatrics. 2010;125(6):e1348-e1355.
- McKay S, Gravel JS, Tharpe AM. Amplification considerations for children with minimal or mild bilateral hearing loss and unilateral hearing loss. Trends Amplif. 2008;12(1):43-54.
- Snapp HA, Holt FD, Liu X, Rajguru, SM. Comparison of speech-in-noise and localization benefits in unilateral hearing loss subjects using contralateral routing of signal hearing aids or bone-anchored implants. Otol Neurotol. 2017;38(1): 11-18.
- Pierzycki RH, Edmondson-Jones M, Dawes P, Munro KJ, Moore DR, Kitterick PT. Associations between hearing health and well-being in unilateral hearing impairment. Ear Hear. 2020;42(3):520-530.
- Leterme G, Bernardeschi D, Bensemman A, et al. Contralateral routing of signal hearing aid versus transcutaneous bone conduction in single-sided deafness. Audiol Neurootol. 2015;20(4):251-260.
- Lucas L, Katiri R, Kitterick PT. The psychological and social consequences of single-sided deafness in adulthood. Int J Audiol. 2018;57(1):21-30.
- Snapp H. Nonsurgical management of single-sided deafness: Contralateral routing of signal. J Neurol Surg B Skull Base. 2019;80(2):132-138.
- Wie OB, Pripp AH, Tvete O. Unilateral deafness in adults: Effects on communication and social interaction. Ann Otol Rhinol Laryngol. 2010;119(11):772-781.
- Bess FH, Dodd-Murphy J, Parker RA. Children with minimal sensorineural hearing loss: prevalence, educational performance, and functional status. Ear Hear. 1998;19(5):339-354.
- Oyler RF, Oyler AL, Matkin ND. Unilateral hearing loss: Demographics and educational impact. Lang Speech Hear Serv Sch. 1988;19(2):201-210.
- Lieu JEC, Karzon RK, Ead B, Tye-Murray N. Do audiologic characteristics predict outcomes in children with unilateral hearing loss? Otol Neurotol. 2013;34(9):1703-1710.
- Harford E, Barry J. A rehabilitative approach to the problem of unilateral hearing impairment: The contralateral routing of signals (CROS). J Speech Hear Disord. 1965;30(2):121-138.
- Bagatto M, DesGeorges J, King A, et al. Consensus practice parameter: Audiological assessment and management of unilateral hearing loss in children. Int J Audiol. 2019;58(12):805-815.
- Choi JE, Ma SM, Park H, Cho Y-S, Hong SH, Moon IJ. A comparison between wireless CROS/BiCROS and soft-band BAHA for patients with unilateral hearing loss. PLoS One. 2019;14(2):e0212503.
- Fogels J, Jonsson R, Sadeghi A, Flynn M, Flynn T. Single-sided deafness-Outcomes of three interventions for profound unilateral sensorineural hearing loss: A randomized clinical trial. Otol Neurotol. 2020;41(6), 736-744.
- Kuk F, Seper E, Lau C, Crose B, Korhonen P. Effects of training on the use of a manual microphone shutoff on a BiCROS device. J Am Acad Audiol. 2015;26(5), 478-493.
- Kurz A, Rak K, Hagen R, Ehrmann-Muller D. Evaluating the decision for cochlear implantation in individuals with single-sided deafness (SSD): Implementing the SSD Consensus Protocol into clinical routine. Otol Neurotol. 2020;41(6):727-735.
- Mosnier I, Lahlou G, Flament J, et al. Benefits of a contralateral routing of signal device for unilateral Naida CI cochlear implant recipients. Eur Arch Otorhinolaryngol. 2019;276(8):2205-2213.
- Picou EM, Davis H, Lewis D, Tharpe AM. Contralateral routing of signal systems can improve speech recognition and comprehension in dynamic classrooms. J Speech Lang Hear Res. 2020;63(7):2468-2482.
- Ryu N-G, Moon IJ, Byun H, et al. Clinical effectiveness of wireless CROS (contralateral routing of offside signals) hearing aids. Eur Arch Otorhinolaryngol. 2015;272(9):2213-2219.
- Snapp HA, Hoffer ME, Liu X, Rajguru SM. Effectiveness in rehabilitation of current wireless CROS technology in experienced bone-anchored implant users. Otol Neurotol. 2017;38(10):1397-1404.
- Williams VA, McArdle RA, Chisolm TH. Subjective and objective outcomes from new BiCROS technology in a veteran sample. J Am Acad Audiol. 2012;23(10):789-806.
- Dwyer RT, Kessler D, Butera IM, Gifford RH. Contralateral routing of signal yields significant speech in noise benefit for unilateral cochlear implant recipients. J Am Acad Audiol. 2019;30(3):235-242.
- Oeding K, Valente M. Sentence recognition in noise and perceived benefit of noise reduction on the receiver and transmitter sides of a BICROS hearing aid. JAm Acad Audiol. 2013;24(10):980-991.
- Peters JPM, Smit AL, Stegeman I, Grolman W. Review: Bone conduction devices and contralateral routing of sound systems in single-sided deafness. Laryngoscope. 2015;125(1):218-226.
- Arndt S, Laszig R, Aschendorff A, Hassepass F, Beck R, Wesarg T. Cochlear implant treatment of patients with single-sided deafness or asymmetric hearing loss. HNO. 2017;65[Suppl 2]:98-108.
- Dornhoffer JR, Dornhoffer JL. Pediatric unilateral sensorineural hearing loss: Implications and management. Curr Opin Otolaryngol Head Neck Surg. 2016;24(6):522-528.
- Snapp HA, Hoffer ME, Spahr A, Rajguru S. Application of wireless contralateral routing of signal technology in unilateral cochlear implant users with bilateral profound hearing loss. J Am Acad Audiol. 2019;30(7):579-589.
- Taal CH, van Barneveld DCPBM, Soede W, Briaire JJ, Frijns JHM. Benefit of contralateral routing of signals for unilateral cochlear implant users. J Acoust Soc Am. 2016;140(1):393.
- Van de Heyning P, Tavora-Vieira D, Mertens G, et al. Towards a unified testing framework for single-sided deafness studies: A consensus paper. Audiol Neurootol. 2016;21(6), 391-398.