Research | January 2019 Hearing Review
Attitudes of audiologists about the CHW model for increasing access to hearing healthcare
Hearing loss is a leading cause of disability in the United States. However, individuals with hearing loss often do not receive appropriate audiologic care due to barriers, such as lack of hearing healthcare professionals, poor public awareness of the impact of hearing loss, limited resources, geographical isolation, and lack of transportation. The purpose of this study was to understand perceptions of audiologists with regards to a novel service delivery model that involves the use of community healthcare workers (CHWs) in audiology. Results of this study reveal key areas of concern and opportunities regarding use of trained laypersons to increase outreach in audiology.
Approximately 37.5 million American adults claim to have difficulty hearing1; however, only 22% of adults who could benefit from hearing aids (HAs) receive them.2 Barriers to hearing healthcare extend beyond cost and include lack of hearing care professionals, poor public awareness, limited resources, geographical barriers, and transportation barriers.
One emerging healthcare model which may alleviate some of these barriers is the use of community health workers (CHWs) in audiology.3,4 A CHW is a trained layperson who shares important similarities, such as language, ethnicity, geographical location, and life experiences, with the patients they serve.5 As a result, the CHW is uniquely aware of societal factors that impact the patient’s health status, their access to healthcare, and their attitudes toward healthcare.
CHWs have been used in other medical fields to provide health education and counseling, help patients navigate the healthcare system, perform screenings, make timely referrals, and provide support for chronic disease self-management.6,7 Therefore, the use of CHWs may help reduce the current gap between those individuals with hearing loss and those accessing services.
Community Health Workers and Audiology
The 2016 report by The National Academies of Science, Engineering, and Medicine (NASEM) titled Hearing Health Care for Adults: Priorities for Improving Access and Affordability8 specifically suggests CHWs as one mechanism to improve access for underserved hearing-impaired populations.
Currently, there are two pilot programs that have trained CHWs to address hearing loss in their communities through an academic-community partnership. The first is the Baltimore HEARS program, which is currently testing their intervention strategy utilizing trained CHWs to deliver an aural rehabilitation (AR) program, including hearing loss education, communication strategies, and the provision of a personal sound amplification product to low-income, minority seniors in Baltimore City.3,9,10 The second program, Oyendo Bien, uses a CHW-health educator model to deliver group AR programs to underserved communities along the US-Mexico border.4,11,12 Initial results of these two pilot programs suggest that application of a CHW model, in conjunction with training from audiologists, may be a novel and viable way to address the hearing healthcare needs of these underserved populations.
While these studies have used an academic-community partnership to train CHWs to provide audiology services, at present, there is no established model for the use of CHWs in the clinical practice of audiology. Therefore, the aim of this study was to conduct a focus group to explore whether clinical audiologists view CHWs as a favorable approach to extending access to hearing healthcare to underserved adults.
Methods
Participants. A total of eight Maryland-licensed audiologists participated (Table 1). Five were private practice owners, two were audiologists in ENT offices, and one was an assistant professor at a university. Their years of experience in a practice ranged from 0-23 years (the assistant professor had not worked in a practice as a clinician, but had been conducting audiology research for 7 years).
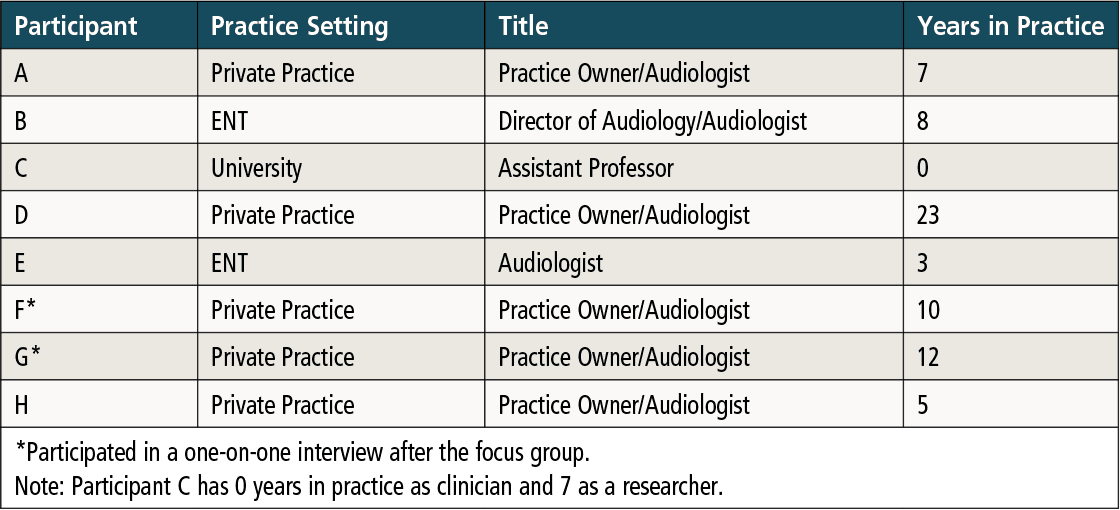
Table 1. Demographic information for focus group participants.
Procedure. The primary moderator asked questions regarding participants’ experiences working with clients, as well as their experiences with community health and CHWs. A primary and secondary moderator facilitated the 1.5 hour discussion, which was recorded with audio and written notes.
Based on the range of opinions expressed during the focus group, two individuals who had opposing views on the potential use of CHWs in audiology were purposively sampled for follow-up semi-structured interviews. The two participants chosen for the individual interviews had both owned private practices for about 7 years. Separate sets of questions were developed for each interview. These interviews were also audio recorded.
Analysis. The primary investigator (M.F.) performed a close reading of the transcripts and developed a codebook to define terms to code all segments of the transcript. Then two researchers (M.F. and P.K.) independently applied these codes to the transcripts. Following discussion, the final codebook was agreed upon by the research team and a final round of coding was performed independently by the two researchers. This coding strategy was used to categorize the data into patterns which served as the basis for data analysis and discussion.
Results
Seventeen codes were operationally defined and used to analyze the data. Table 2 contains the 10 most commonly occurring codes, with a description and an exemplary quotation for each code. During the individual interview, Participant G, who worked in a rural environment, was enthusiastic regarding use of CHWs in audiology, despite recognizing limitations. In contrast, Participant F, who worked in a more suburban environment, found it difficult to envision any situation where CHWs would provide meaningful contributions to the field.
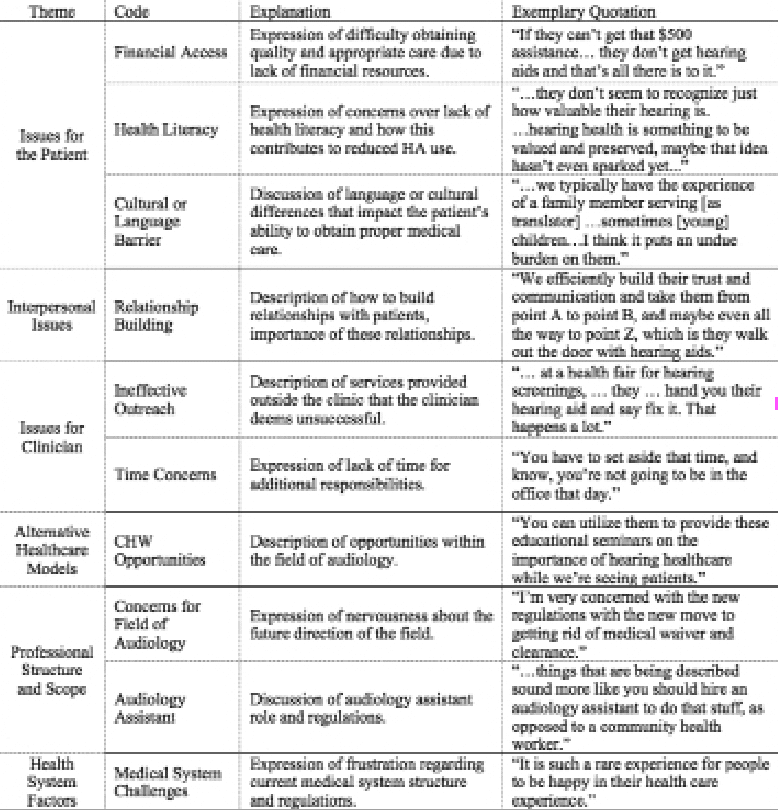
Table 2. Common codes with explanations and quotations used in analysis of the transcripts.
Discussion
Six prominent themes emerged from both the focus group discussion and the interviews (Table 2). We have collapsed those themes into broad categories related to the patient, the clinician, and the health system.
Issues for patient. Participants identified several factors that have been discussed in the literature as contributing to difficulty in obtaining quality and appropriate audiologic care. These factors include geographic isolation, lack of financial resources, and low health literacy. In regards to geographic isolation, older adults living in remote areas have reported difficulty obtaining healthcare due to problems with transportation, limited healthcare options, and social isolation.13 In addition, researchers have found that individuals living at or below the federal poverty level are less likely to obtain hearing aids than individuals with higher incomes.14 Lastly, researchers have also found that there is a distinct difference in the language used by audiologists and the health literacy levels of their patients with hearing loss.15 Low health literacy has been linked with poor health outcomes, decreased access to healthcare services, and greater health disparities among racially diverse populations.16,17 Both of the recent pilot studies that used a CHW model have expressly been designed to address these access barriers.3,4
Issues for the clinician. The participants discussed the challenges related to the time and resources necessary to provide outreach services beyond the clinic. While many participants had provided services outside of the clinic, a majority found that these ventures were unsuccessful due to the time and/or monetary commitments involved. These outreach services included performing hearing screenings at health fairs and visiting long-term care facilities for educational seminars for staff and residents. They reported that the outcomes of these services did not justify the expense and effort put forth.
Another aspect of clinical practice that requires time relates to building relationships with clients. The audiologists discussed the importance of building relationships with their clients in order to provide the best possible hearing healthcare—especially for those hearing-impaired individuals who lack the intrinsic motivation necessary to pursue amplification. Saunders and colleagues18 recommended that clinicians try to motivate hearing-impaired individuals to seek help by identifying patient-centered variables that limit help-seeking behaviors. Recently, Ng and Loke19 reported that self-perception of hearing handicap, expectation of potential benefit from amplification, and support from others are non-audiologic determining factors in the successful use of hearing aids. Collectively, these findings suggest that patient motivation and empowering clinician-patient relationships are crucial to successful hearing aid adoption. In other fields, CHWs have served as liaisons with the professionals to support these types of person-centered motivations necessary to seek help and to maintain care routines for chronic conditions.5
Health system factors. Participants expressed a deep level of frustration regarding the complexities of the current US healthcare system and Medicare regulations. Some participants felt that unnecessary Medicare rules and regulations require too much additional time and effort on the part of the clinician. Additionally, participants expressed that they have struggled to adapt to new policies that accompanied the adoption of the Affordable Care Act (ACA). Researchers have also addressed the complexity of the US healthcare system and its inadequate coverage for hearing healthcare services, arguing that more must be done to provide affordable hearing healthcare and expand insurance coverage for hearing aids.8,20
In addition to issues related to insurance, participants spent a substantial amount of time discussing the professional scope and structure of audiology—specifically, the role of audiology assistants. Participants also discussed the emergence of personal sound amplification products (PSAPs) and over-the-counter (OTC) hearing aids. In recent years, reports published by the President’s Council of Advisors on Science and Technology (PCAST)21 and NASEM8 have called for more actions towards increasing availability of hearing technology. Both reports called for US Food and Drug Administration (FDA) regulations for a new class of amplification products that would create more accessible and innovative approaches to meeting the communication needs of hearing-impaired adults. At the time of the focus group, the OTC Hearing Aid Act of 2016 had been recently introduced in the US Congress, and subsequently passed into law in August 2017. This legislation calls for the creation of a category of FDA-regulated OTC hearing aids for adults with mild-to-moderate hearing loss.
Community Health Model
When questioned, none of the participants were familiar with community health or CHWs. When provided with a definition of a CHW and examples of how they have been used in other fields, some participants expressed a better understanding. However, even at the conclusion of the focus group, some participants still had several questions about the roles and responsibilities of CHWs. Following a discussion of CHWs, participants were asked to name potential opportunities and limitations for CHWs in the field of audiology (see Table 3).

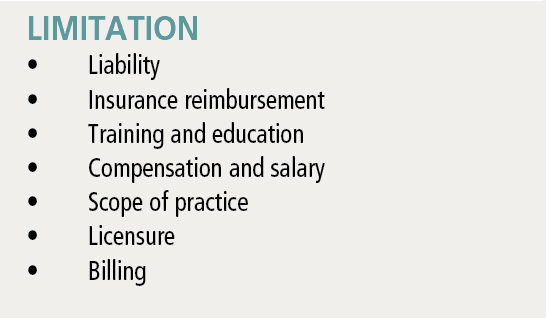
Table 3. Summary of opportunities and limitations for CHWs raised during focus group.
The opportunities discussed are reflected in the two CHW-delivered AR programs that have been reported in the literature.3,4 Participant G had several anecdotes regarding times she had relied on socially or technologically savvy patients to serve as peer mentors for other patients in her practice. Participant G had great enthusiasm for building this approach into her practice as a CHW model of care.
Many of the limitations of CHWs raised during the focus group have also been addressed in the literature. For example, insurance reimbursement is currently limited for services provided by CHWs. However, the ACA recently expanded the ability of the Centers for Disease Control and Prevention (CDC) to provide grants for community-based outreach. Additionally, the Centers for Medicare and Medicaid Services (CMS) have introduced a rule that would allow CHWs to receive reimbursement for services as long as these services are recommended by a licensed professional.22 Individual states have also expanded reimbursement for services provided by CHWs through Medicaid.
Limitations of this Study
There are several limitations associated with this study. The first limitation is that the study employed a small sample of audiologists from one geographic area, limiting the generalizability of these results. Second, participants may have been hesitant to openly voice opinions or express disagreement in the group. Finally, despite multiple recruiting efforts, participants were drawn almost exclusively from alumni of Towson University’s AuD program and thus were from a similar educational background. This may have biased their responses and reactions during the sessions.
Conclusions
The aim of this study was to determine whether use of CHWs is a favorable approach to extending access to hearing healthcare from the perspective of audiologists. Using a focus group and semi-structured interviews, we examined factors that may contribute to the success of a CHW model in hearing healthcare. There was a continuum of opinions regarding this issue, as well as clear divisions between those with a positive perspective of this model and those with a negative perspective.
Future Directions
This was an exploratory study that investigated a topic that is still in the early stages of testing and implementation. Therefore, it is necessary to expand upon this study and obtain information from a larger, more diverse population of clinical audiologists, possibly through a qualitative survey approach. Future studies should examine whether the nature of audiologists’ work settings lead to different opinions regarding use of CHWs in audiology. Specifically, urban vs rural work settings should be examined to determine whether these differences change audiologists’ perspectives on the utility of CHWs.
The results of this preliminary study suggest that it is imperative to work with clinical audiologists and provide education about CHWs and community health so that this model is seen as an assetrather than a threat to the field. Concerns raised during the focus group and interviews should be considered in order to develop a model that is appealing, implementable, scalable, and sustainable.
As this CHW healthcare model continues to expand, new rulings and research may provide additional clarity for providers regarding cost and reimbursement for using CHWs in their practices. Allowing CHWs to be involved in providing some services to the hearing-impaired population may improve the audiologist’s ability to efficiently treat more patients by saving time and money.
Acknowledgements
Nick Reed, Jon Suen, and Frank Lin are gratefully acknowledged for their guidance and contributions to this project.
Correspondence can be addressed to Dr Mamo at: [email protected]



About the Authors: Sara K. Mamo, AuD, PhD, is an assistant professor at the University of Massachusetts Amherst; Meredith R. Frank, AuD, is an audiologist at Clarke Schools for Hearing and Speech in Northampton, Mass; and Peggy Korczak, PhD, is a Professor of Audiology at Towson University in Towson, Md.
Citation for this article: Mamo SK, Frank MR, Korczak P. Exploring Community Health Worker (CHW) models for delivering audiology services. Hearing Review. 2019;26(1)[Jan]:12-17.
References
-
Blackwell DL, Lucas JW, Clarke TC; Centers for Disease Control. Summary health statistics for US adults: National health interview survey, 2012. https://www.cdc.gov/nchs/data/series/sr_10/sr10_260.pdf. Published February 2014.
-
Margolis RH, Morgan DE. Automated pure-tone audiometry: An analysis of capacity, need, and benefit. Am J Audiol.2008;17(2):109-113.
-
Nieman CL, Marrone N, Mamo SK, et al. The Baltimore HEARS pilot study: An affordable, accessible, community-delivered hearing care intervention. Gerontologist. 2017;57(6):1173-1186.
-
Marrone N, Ingram M, Somoza M, et al. Interventional audiology to address hearing health care disparities: Oyendo bien pilot study. Semin Hear.2017;38(02):198-211.
-
Kim K, Choi JS, Choi E, et al. Effects of community-based health worker interventions to improve chronic disease management and care among vulnerable populations: A systematic review. Am J Public Health. 2016;106(4):e3-e28.
-
McCord GC, Liu A, Singh P. Development of community health workers across sub-Saharan Africa: Financial considerations and operational assumptions. Bull World Health Org. 2012;91:244-253B.
-
Verhagen I, Steunenberg B, de Wit NJ, Ros WJG . Community health worker interventions to improve access to health care services for older adults from ethnic minorities: A systematic review. BMC Health Serv Res. 2014;14:497.
-
The National Academies of Sciences, Engineering, and Medicine. Hearing health care for adults: Priorities for improving access and affordability. http://nationalacademies.org/hmd/reports/2016/Hearing-Health-Care-for-Adults.aspx. Published June 2, 2016.
-
Suen J, Lin F, Nieman CL, et al. Developing a community health worker training curriculum for hearing care. Poster presented at: The 44th Annual Scientific and Technology Conference of the American Auditory Society; March 2-4, 2017; Scottsdale, AZ.
-
Suen J, Han H-R, Nieman C, et al. Baltimore HEARS pilot: A community health worker hearing care intervention. Poster presented at: The 45th Annual Scientific and Technology Conference of the American Auditory Society; March 1-3, 2018; Scottsdale, AZ.
-
Ingram M, Marrone N, Sanchez DT, et al. Addressing hearing health care disparities among older adults in a US-Mexico border community. Front Public Health. 2016;4(169).
-
Sanchez D, Adamovich S, Ingram M, et al. The potential in preparing community health workers to address hearing loss. J Am Acad Audiol. 2017;28(6):562-574.
-
Goins RT, Williams KA, Carter MW, Spencer SM, Solovieva T. Perceived barriers to health care access among rural older adults: A qualitative study. J Rural Health. 2005;21(3):206-213.
-
Bainbridge KE, Ramachandran V. Hearing aid use among older US adults: The national health and nutrition examination survey, 2005-2006 and 2009-2010. Ear Hear. 2014;35(3):289-294.
-
Nair EL, Cienkowski KM. The impact of health literacy on patient understanding of counseling and education materials. Int J Audiol. 2010;49(2):71-75.
-
Bennett IM, Chen J, Soroui JS, White S. The contribution of health literacy to disparities in self-rated health status and preventive health behaviors in older adults. Ann Fam Med. 2009;7(3):204-211.
-
Smith SG, O’Conor R, Curtis LM, et al. Low health literacy predicts decline in physical function among older adults: Findings from the LitCog cohort study. J Epidemiol Community Health. 2015;69(5):474-480.
-
Saunders GH, Chisholm TH, Wallhagen MI. Older adults and hearing help-seeking behaviors. Am J Audiol.2012;21(2):331-337.
-
Ng JH-Y, Loke AY. Determinants of hearing-aid adoption and use among the elderly: A systematic review. Int J Audiol. 2015;54(5):291-300.
-
McNeal MH. Say what? The Affordable Care Act, Medicare, and hearing aids. Harvard J Legis.2016;53:621-670.
-
President’s Council of Advisors on Science and Technology (PCAST). Aging America & hearing loss: Imperative of improved hearing technologies. https://obamawhitehouse.archives.gov/sites/default/files/microsites/ostp/PCAST/PCAST%20hearing%20letter%20report.pdf. Published October 2015.
-
Centers for Medicare & Medicaid Services (CMS). Medicaid and children’s health insurance programs: Essential health benefits in alternative benefit plans, eligibility notices, fair hearing and appeal processes, and premiums and cost sharing; exchanges: Eligibility and enrollment. July 15, 2013. https://www.federalregister.gov/documents/2013/07/15/2013-16271/medicaid-and-childrens-health-insurance-programs-essential-health-benefits-in-alternative-benefit