
A tutorial on the practical implementation of verification and validation measures in a dispensing office
Verification and validation are clinical tools to ensure functionality of hearing aids as well as individual patient benefit. However, they are not always employed by clinicians, even though they have been found to be correlated with user satisfaction. Rationale and research into the benefits of verification and validation measures are discussed, in addition to ways to implement them into clinical practice.
Verification techniques are primarily used to determine if the hearing aids meet a particular standard and are performing appropriately. Validation techniques use functional gain, speech perception, questionnaires, or interviewing to determine how much benefit one is receiving from the hearing aids.
Performing only verification measures provides information regarding how much gain your patient is receiving, but little information about whether this amount of gain is actually benefiting your patient. Performing only validation measures provides benefit information, but does not provide any information regarding whether your patient is fit with the appropriate amount of gain.



Tammara Stender, AuD, is a senior audiologist, Rena Appleby, AuD, is an audiologist, and Stephen Hallenbeck, AuD, is a senior audiologist at the GN ReSound Global Audiology Center in Glenview, Ill.
Therefore, the only way to obtain a complete picture of the amount of gain and benefit your patient is receiving is to perform both verification and validation—or V&V—techniques.
What are some reasons clinicians do not verify or validate the hearing aid fitting using real-ear measures, clinical testing, or questionnaires? They include:
- Unclear on test result interpretation or how to convey results to patients, and/or belief that digital hearing aids cannot be verified by real ear;
- Not knowing when to verify or validate;
- Perceptions that the measurement/probe microphone placement may be uncomfortable for patients;
- Changing technology (open fits, digital aids, etc) negates the use of real ear;
- Real-ear or validation measures do not necessarily lead to more sales;
- Cannot bill for specific procedure;
- Lack of confidence in procedures;
- Do not own up-to-date real-ear equipment;
- Feel that, if the patient is happy with the fitting, V&V measures do not matter;
- Time pressures in a busy clinic.
Why V&V Is Essential
Although there are various reasons why clinicians may choose not to verify the hearing aid fitting, there are several very good reasons why it is important. First, less than 12% of targets on the manufacturer’s fitting software screen match what is actually measured in the patient’s ear.1,2
In addition, the fitting software often overestimates the gain in the higher frequencies3 and may not be indicative of the maximum output.4 The target gain settings in the software are simulated values based on the patient’s audiogram, representing the amount of gain the manufacturer would expect someone with an average ear size to obtain. Therefore, an individual patient can be expected to receive more gain than shown in the software if they have a smaller-than-average ear, and less gain if they have a larger-than-average ear.
Further, the target settings may not be adequate for patient benefit, especially regarding speech intelligibility. An online survey showed that 70% of responding audiologists program their patient’s hearing aids using the manufacturer’s “first-fit” settings.5 Since first-fit gain settings may not be giving enough gain for some users, and the first-fit targets may be less than the actual gains in the ear, patients may not be receiving enough amplification for improved speech intelligibility and benefit. Verification and validation measures ensure that the hearing aids are providing the appropriate amounts of amplification, and that the amplification they provide is actually benefiting the patient in daily life.
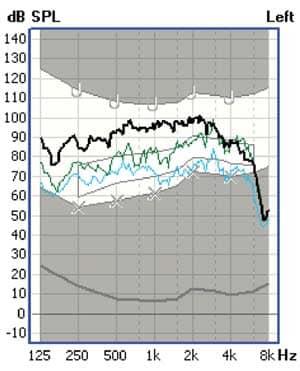
FIGURE 1. Spectral analysis for verification of audibility across soft, moderate, and loud levels. The X’s represent the patient’s hearing thresholds per frequency for the left ear, and the U’s show the UCLs per frequency. The blue line shows the real-ear aided response (REAR) for soft input sounds; the green line shows the REAR for moderate level sounds; the black line indicates the REAR for loud sounds. Note in this example the UCLs are not exceeded at any frequency by the black line (indicative of loud sounds).
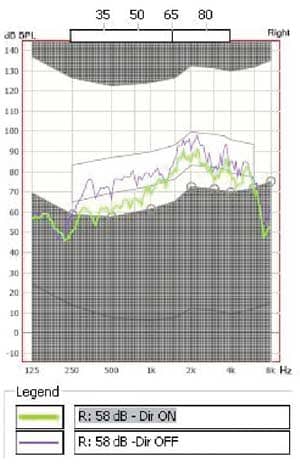
FIGURE 2. Directional real-ear test, conducted with the patient facing 180° from the speaker. The green line indicates the response when directionality is on, and the purple line shows the response when directionality is off. This demonstrates the value of directionality.
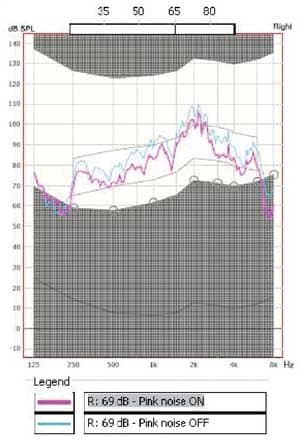
FIGURE 3. Noise reduction real-ear test, conducted with a noise-like signal and the patient facing the speaker. The pink curve reveals the response when noise reduction is set to “Strong,” and the blue curve shows the response when noise reduction is off.
Verification Measures
There are two basic techniques of verification that can be performed: coupler measurements and real-ear measurements.
Coupler measurements can be run prior to the fitting or at any time during the fitting process, to ensure the hearing instruments are functioning properly per the manufacturer’s specifications. They can also be used to simulate real-ear measures with the use of a real-ear to coupler difference (RECD), which is especially helpful in verifying gain and output for small children and infants.
Real-ear or probe-microphone measurements determine the amount of gain the patient receives by measuring the SPL near the eardrum with the hearing aid coupled to the ear. Spectral analysis—sometimes referred to as speech mapping—is a very useful and informative mode of probe microphone measurement that illustrates audibility for a patient for speech sounds ranging from soft to loud. Spectral analysis results are displayed as output—not gain—and graphed on a chart called an SPL-o-gram. In this verification measure, the fitter enters a patient’s hearing thresholds and uncomfortable loudness levels (UCLs) into the real-ear system software. Typically, a speech banana, which is a representation of the long-term average speech spectrum that shows the average intensity of speech as a function of frequency, or prescriptive targets for different input levels, can be displayed on the screen along with the patient’s hearing thresholds. With a probe tube appropriately inserted into the ear canal, selected signals are played through the real-ear equipment speakers at various intensity levels, typically soft (50-55 dBSPL), moderate (65-70 dBSPL), and loud (85-90 dBSPL).
The response is displayed on the screen of the equipment for each of the input levels along with the patient’s hearing thresholds for the ear being tested (converted to SPL in Figure 1). In the SPL-o-gram, audible sounds are above the patient’s hearing thresholds. Thus, it is easy to see at a glance whether sounds at soft levels are audible, as they will be above the patient’s hearing thresholds. In addition, if a speech banana or prescriptive fitting rule targets are selected and displayed on the screen, the display will show how well the targets are being matched for each input level. Finally, by selecting a high-intensity stimulus, the clinician can determine whether the patient’s UCLs will be exceeded by very loud sounds in the real-world environment.
Sound Stimuli Options
There are many types of sound stimuli that can be used in spectral analysis, ranging from puretone-based to speech-based. In puretone-based sound stimuli, a swept puretone is used to measure the hearing aid output at each frequency.
For speech-based sound stimuli, many options are currently available, including live speech provided by the patient or the patient’s significant other, speech-weighted noise, and signals derived from real speech such as the International Speech Test Signal (ISTS).6 The ISTS was designed to contain a wide range of the natural characteristics of speech, including the average speech spectrum and the modulation spectrum, as well as variations in the fundamental frequency and harmonics. In addition, the ISTS combines phonemes from several different languages in order to get a standardized international representation of hearing aid response for speech.
Although several options exist for sound stimuli, it may be advantageous to consider those that are most similar to real-world sounds the patient encounters during hearing aid use. For this reason, speech-based stimuli are an excellent choice.
Speech-weighted noise was traditionally used before other options were available, but now has certain limitations with current digital hearing aid technology and algorithms. For example, while testing a patient with speech-weighted noise, it may be necessary to turn off certain algorithms, such as noise reduction, that may reduce the output of the hearing aid due to the low-modulation noise characteristics of the speech-weighted noise.
On the other hand, modulated signals—such as live voice and the ISTS signal—do not experience this complication, and algorithms, such as noise reduction, typically do not need to be disabled to obtain a valid real-ear verification measurement. Additionally, a truer representation of the patient’s real-world hearing aid output may be derived by using live-voice or ISTS signals, since the patient will typically be encountering modulated speech during their everyday use of the hearing aids.
Using Verification for Hearing Aid Feature Analysis
Other aspects of real-ear verification are helpful to ensure that hearing aid features are working properly, and to set realistic expectations about the extent of their impact on sound quality in everyday use.
Verifying directionality of a hearing aid. A simple real-ear test can determine whether directional microphones are functioning properly. In this test, noise reduction should be deactivated. With the patient seated in a chair facing 180° from the speaker of the real-ear equipment, a noise-like signal such as speech noise is presented, first with directionality turned off. Then the noise is presented again with directionality turned on, preferably in a fixed response. It is necessary to wait about 10 seconds for the full directional effect to occur before capturing the curve. If directionality is functioning properly, the curve obtained with directionality turned on will have a smaller amplitude than the curve obtained with directionality off (Figure 2).
Verifying noise reduction in a hearing aid. Another test can determine if the amount of noise reduction programmed into the hearing aid will impact audibility in certain environments. The signal used for this test should be noise-like, not speech-like, so that the hearing aid can identify the signal as a noise signal and activate noise reduction. For this reason, a pink or white noise stimulus is useful. The patient is positioned facing the speaker (at 0°) and the noise is presented at 65 dBSPL, with noise reduction both on and off. Again, it is best to wait a few seconds before capturing the curve for the “noise reduction on” condition to allow the feature to fully reduce the level of the sound. If the response curve with noise reduction activated dips below the patient’s thresholds, it can be assumed that some audibility may be sacrificed when the feature is active at that level. Figure 3 shows the results of this noise reduction test through real-ear measures.
Verification as a counseling tool. In the case of time pressures during patient visits, both of these tests for directionality and noise reduction can be slightly modified to be tested in the coupler before the patient arrives. However, real-ear verification including spectral analysis or speech mapping can also serve as a valuable counseling tool for the patient. The dispensing professional can explain how the hearing aids are making sounds in the real world to be loud enough to hear based on the patient’s hearing thresholds. This type of counseling not only builds the professional relationship between the fitter and the patient, but it also can further educate the patient about the function of his or her hearing aids.
Validation Measures
Validation measures provide invaluable information regarding the benefit patients receive from amplification. Measurement techniques typically involve the use of objective and subjective measurements, with objective measurements providing information obtained within the clinic environment and subjective measures usually providing real-world information.
Three areas of hearing aid outcome, measured through both objective and subjective tests, have been noted to be of particular importance when deriving overall user benefit, as shown in Table 1.7,8
TABLE 1. Validation outcome measures and examples of corresponding objective and subjective tests.
Although these tests and surveys are helpful, the list is not exhaustive. Other surveys, such as the Hearing Handicap Inventory for the Elderly (HHIE),9 can help determine the amount of handicap reduction the patient experiences, by comparing unaided to aided results. Open-ended assessments such as the Client Oriented Scale of Improvement (COSI)10 allow patients to specify the areas of improvement that are most important for their daily lives. Also, non-formal interviewing of the patient at the follow-up visit can highlight areas of improvement that have already occurred and other areas that are still difficult. Thus, the results of validation tests or assessments can be used to apply counseling or rehabilitative techniques to address the problems patients are experiencing.
It would not be time or cost-effective for dispensing professionals to institute all of these verification and validation procedures into their hearing aid fittings and follow-up visits. However, not performing any of these measures can be more costly in terms of numerous follow-up visits and returns of hearing aids due to dissatisfied users. Often, it is helpful for the clinician to show patients the amount of benefit they are receiving, especially if they have not yet acclimated to the devices in everyday use. Validating hearing aid benefit may also be necessary for third-party payment.11
Many studies point to the comprehensive benefits of employing verification and validation measures in hearing aid dispensing. Kochkin noted that improved satisfaction arises from the use of outcome measurement, as well as counseling.12 Valente et al13 noted that instituting clinical verification and validation techniques helped grow their practice, reduced the return rate, and provided satisfaction not only among hearing aid users but among clinicians, as they felt proud of their level of care for their patients.
Thus, the benefits of verification and validation extend not only to hearing aid users but also to the clinicians who serve them.
References
- Aarts NL, Caffee CS. Manufacturer predicted and measured REAR values in adult hearing aid fitting: accuracy and clinical usefulness. Int J Audiol. 2005;44(5):293-301.
- Aarts NL, Caffee CS. The accuracy and clinical usefulness of manufacturer-predicted REAR values in adult hearing aid fittings. Hearing Review. 2005;12(12):16-22.
- Hawkins DB, Cook JA. Hearing aid software predictive gain values: how accurate are they? Hear Jour. 2003;56(7):26,28,32.
- Mueller HG, Bentler RA, Wu YH. Prescribing maximum hearing aid output: differences among manufacturers found. Hear Jour. 2008;16(3):30-36.
- Lindley G. Current hearing aid fitting protocols: results from an online survey. Audiology Today. 2006;18(3):19-22.
- Holube I, Fredelake S, Vlaming M, Kollmeier B. Development and analysis of an International Speech Test Signal (ISTS). Int J Audiol. 2010;49(2);891-903.
- Humes LE. Modeling and predicting hearing-aid outcome. Trends Amplif. 2003;7(2):41-75.
- Humes LE. Hearing-aid outcome measures in older adults. In: Palmer CA, Seewald RC, eds. Hearing Care for Adults. Stafa, Switzerland: Phonak AG; 2007:265-276.
- Weinstein BE, Spitzer JB, Ventry IM. Test-retest reliability of the Hearing Handicap Inventory for the Elderly. Ear Hear. 1986;5:295-299.
- Dillon H, James A, Ginis J. The Client Oriented Scale of Improvement (COSI) and its relationship to several other measures of benefit and satisfaction provided by hearing aids. J Am Acad Audiol. 1997;8(2):27-43.
- Humes LE, Amos NE. Are your hearing aid fittings “on target”? ASHA Leader. September 1, 2009.
- Strom KE. HR interviews Sergei Kochkin, PhD. Hearing Review. 2005;12(11):24-32,82.
- Valente M, Potts LG, Valente M. Signal testing approaches; clinical procedures to improve user satisfaction with hearing aids. In: Tobin H, ed. Practical Hearing Aid Selection and Fitting. Baltimore: Department of Veterans Affairs; 1995:Chapter 6.
- Cox RM, Alexander GC, Gilmore CA. Development of the Connected Speech Test (CST). Ear Hear. 1987;8(5 Suppl):119S-126S.
- Walden BE, Demorest ME, Hepler EL. Self-report approach to assessing benefit derived from amplification. J Speech Hear Res. 1984;27:49-56.
- Cox R, Alexander G. Measuring satisfaction with amplification in daily life: the SADL. Ear Hear. 1999;20:306-320.
- Cox RM, Alexander GC. The abbreviated profile of hearing aid benefit. Ear Hear. 1995;16:176-86.
- Cox RM, Stephens D, Kramer SE. Translations of the International Outcome Inventory for Hearing Aids (IOI-HA). Int J Audiol. 2002;41:3-26. The IOH-HA is also available at: www.memphis.edu/ausp/harl/ioi-ha.htm.
Correspondence can be addressed to HR or Tammara Stender, AuD, at .

