
By David Smriga, MA
H.R. 3’s current language promotes a bias—intended or not—that mild-to-moderate hearing loss and severe-to-profound hearing loss are two distinct categories, requiring two distinct legislative treatments. Says who?
On April 18, 2017, the FTC held a workshop looking at hearing aids and over-the-counter (OTC) devices.1 Several panel presentations/discussions comprised this workshop. One panel in particular was asked to speak to the costs and benefits of hearing healthcare regulations. The panel included representatives from IHS, AAA, the FTC, and the Consumer Technology Association. At one point, the representative from the Consumer Technology Association stated the following [paraphrased]:
“Look, consumers have a clear choice. They can either choose well designed, well engineered, sophisticated devices designed to help them hear better, or…they can choose hearing aids.”
Clearly, this statement was intended to be both provocative and damning. The speaker wanted his audience to believe a new reality: namely that the hearing aid industry has been poorly serving consumers for decades and that consumers don’t need that industry (or the professional care associated with it) to hear better.
Certainly, the statement was a deliberate affront. But what was more frustrating was that neither AAA or IHS panel members challenged or rebutted his clearly defamatory statement. Left so unchallenged, his statement found a clearer path to becoming a new reality.
On December 12, 2019, the US House of Representatives passed H.R. 3 (the “Elijah Cummings Lower Drug Costs Now Act”) which includes Section 602 entitled, “Providing Coverage for Hearing Care under the Medicare Program.”2 Section 602 of the bill adds two new Medicare hearing benefits: 1) The provision of aural rehabilitation and treatment services by qualified audiologists, and 2) The inclusion of hearing aids for Medicare beneficiaries with severe-to-profound hearing loss. The bill must now go through the Senate, where there is less appetite for negotiating lower drug prices.3
To be clear, H.R. 3 is proposing that all Medicare beneficiaries, regardless of degree of hearing loss, have access to Medicare-covered diagnostic and rehabilitative care as provided by an audiologist. However, only Medicare beneficiaries with a severe-to-profound hearing loss will have access to the proposed hearing aid benefit. And, by some accounts, this represents less than 6% of the total hearing impaired population in the United States.4
So, what “reality” guided federal legislators to limit the hearing aid benefit to those with severe-to-profound hearing loss conditions? Consider the recommendations embodied in the 2015 PCAST (President’s Council of Advisers on Science and Technology) report5 which included the following statement:
“The FDA should designate a distinct category of ‘basic’ hearing aids – non-surgical, air-conduction hearing aids intended to address normal, bilateral, gradual onset, mild-to-moderate age-related hearing loss …, and should approve this class of hearing aids for over-the-counter sale, without the requirement for consultation with a credentialed dispenser…”6
This view of reality suggests that those with mild-to-moderate hearing loss don’t need the kind of hearing aids that those with severe-to-profound hearing loss need. Those with mild-to-moderate hearing losses can fit themselves with OTC products. But, those with severe-to-profound hearing losses need professional consultation and more traditional “hearing aids.”
Could this be the viewpoint that guided the writers of H.R. 3 to limit the “hearing aid” benefit to those with severe-to-profound hearing loss— a viewpoint crafted by a council whose membership included no one from the consuming public or within the hearing health care industry or professions?
We can’t know for sure. But, what we do know is that this notion of drawing a line between mild-to-moderate hearing loss (however defined) and severe-to-profound hearing loss (however defined) as a pivot point in determining the need for a hearing aid benefit (and implicitly the need for associated professional hearing health care) did not come from consumers, nor did it come from the hearing health care community. It came from outside forces. Outside forces clearly interested in crafting a new reality.
In fact, consumer opinion about the importance of professional involvement in hearing health decisions and purchases, regardless of degree of hearing loss, is quite emphatically different.
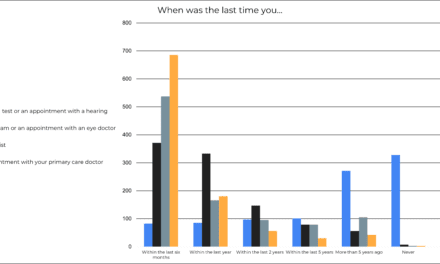
Consider, for example, the results of consumer surveys conducted by the editors at HealthyHearing.com.7 A total of 809 survey participants aged 50 years and older were selected from a nationwide panel of more than 30 million people that was balanced to be representative of the US population. The large sample size resulted in a small (3.45 percent) margin of error. A small margin of error indicates that the survey is likely to be a representative sample of Americans in this age group. The vast majority of respondents reported having normal hearing ability. Of those who reported hearing loss, only 28% wore hearing aids. Therefore, the majority of respondents had little hearing aid experience—the presumed target market for OTC hearing aids. Some examples of the survey responses include the following:
If you needed a hearing test, how important do you think it would be to have a hearing care professional thoroughly evaluate your hearing loss and make recommendations?
- 59.70% – absolutely important
- 33.62% – very important
- 5.19% – of average importance
- 0.62% – of little importance
- 0.87% – not important at all
If you needed hearing aids, how important do you think it would be to have a hearing care professional select, fit and program hearing devices specifically for your needs?
- 60.32% – absolutely important
- 33.50% – very important
- 4.45% – of average importance
- 1.11% – of little importance
- 0.62% – not important at all7
In addition, MarketTrak 9 data8 indicates that 85% of hearing aid users who have hearing aids 4 years old or newer are satisfied with their devices, and 90% of those owners are satisfied with the professional care they received. All while most of these users have a mild-to-moderate hearing loss.4
So, regardless of the degree of hearing loss, or any prior experience with hearing healthcare, it seems evident that the general population of consumers feel professional care and guidance is an important component in effectively treating any degree of hearing loss, and that receiving such care is overwhelmingly satisfying, even for those with mild-to-moderate hearing loss. In addition, considering the co-morbidities now inexorably tied to other-than-normal hearing conditions,9 the most effective treatment would seem to be in the consumer’s best overall health interests.
Unfortunately, H.R. 3’s current language promotes a bias—intended or not—that mild-to-moderate hearing loss and severe-to-profound hearing loss are two distinct categories, requiring two distinct legislative treatments.
Says who?
If not the consumer, and if not those who provide professional hearing healthcare, then these very constituencies must demand an explanation from legislators as to what led them to this distinction. Especially before this distinction becomes actual law.
Because, if an opinion goes unchallenged, it gains a clearer path to becoming a new reality.
Acknowledgement
This article was originally published on the AudNet Hearing Group website and appears here with the permission of the author.
References
1. Strom KE. FTC Workshop Looks at Hearing Aids and OTC Hearing Devices. April 19, 2017. Available at: https://hearingreview.com/inside-hearing/industry-news/ftc-workshop-looks-hearing-aids-otc-hearing-devices
2. 116th US Congress. H.R.3 – Elijah E. Cummings Lower Drug Costs Now Act, Sec 602: Providing Coverage for Hearing Care Under the Medicare Program. September 19, 2019. Available at: https://www.congress.gov/bill/116th-congress/house-bill/3/text#toc-HFC28125AF7654AF7AC6366E440AD29CD
3. Hearing Loss Association of America (HLAA). Breaking News: House Passes Bill for Medicare Coverage of Hearing Aids. December 13, 2019. Available at: https://www.hearingloss.org/house-passes-bill-for-medicare-coverage-of-hearing-aids/
4. Goman AM, Lin FR. Prevalence of hearing loss by severity in the United States. Am J Public Health. 2016 October; 106(10): 1820–1822.
5. PCAST Recommends Creation of “Basic” OTC Hearing Aid Category; Easing of PSAP Regulations. October 23, 2015. Available at: https://hearingreview.com/inside-hearing/industry-news/pcast-report-hearing-loss-raises-concerns
6. President’s Council of Advisors on Science and Technology (PCAST). Aging America & Hearing Loss: Imperative of Improved Hearing Technologies. October 2015. Available at: https://obamawhitehouse.archives.gov/sites/default/files/microsites/ostp/PCAST/pcast_hearing_tech_letterreport_final.pdf
7. Plotnick B, Dybala P. OTC hearing aids—Survey says consumers aren’t sold. April 6, 2017. Available at: https://www.healthyhearing.com/report/52742-Otc-hearing-aids-survey-says-consumers-aren-t-sold
8. Abrams HB, Kihm J. An introduction to MarkeTrak IX: A new baseline for the hearing aid market. Hearing Review.2015;22(6):16-21.
9. Deal JA, Reed NS, Kravetz AD. Incident hearing loss and comorbidity: A longitudinal administrative claims study. JAMA Otolaryngol Head Neck Surg. 2019;145(1):36-43.

About the author: David J. Smriga, MA, is Vice-President of Corporate Communications for AUDNET Hearing Group, a national organization of hearing health care entrepreneurs focused on supporting small business excellence in the hearing care industry.
Correspondence can be addressed to HR or David Smriga at: [email protected].



Karl is absolutely right. Our industry and professional associations have submitted a great deal of information and content to various government bodies regarding their position on the key issues articulated in the “OTC Hearing Aid Act”, and the FDA’s subsequent pending regulations regarding these products. My reference to the incident at the FTC workshop that was included in the article was not included to imply that industry and professional groups are not speaking out in general. It was to highlight that, in that particular incident, a deliberately misleading characterization was left unchallenged. And, as a result, that misleading characterization gained a foothold of legitimacy with ANY constituencies hearing it, including important constituencies outside of the government.
Thus, if the characterization embodied in H.R. 3 that mild-to-moderate hearing loss and severe-to-profound hearing loss are two distinct categories requiring two distinct legislative treatments also goes unchallenged, it too can gain a foothold of legitimacy.
As Karl points out, science confirms that such a distinction is a red herring. And, I am pointing out that neither the consuming public or the hearing health care community ever asked for such a distinction. Indeed, those consumers speaking out at the FDA hearings clearly stated that they weren’t looking for eliminating their audiologist as the path to lower cost hearing aids, but were actually looking for a Medicare benefit to help defray the cost of hearing aids. And now, H.R. 3 suggests a Medicare benefit that enforces that distinction. So, regardless of the efforts of industry and professional groups, as Karl also points out, the government is still not listening.
So, before this proposed benefit becomes actual law, both the consuming public and the professional community need to remind legislators that they are not looking for a cheap hearing aid, they are looking for professionally provided products at a more affordable cost via a Medicare benefit that reaches all degrees of hearing loss.
If government cost is the issue, then the government should propose either a Medicare allowance toward the purchase of hearing aids for all degrees of treatable hearing loss, or a regulatory requirement that any insurance company seeking to be a Medicare advantage company must provide its subscribers with a meaningful (defined by the government) hearing aid benefit available for all degrees of treatable hearing loss. To restrict the benefit to severe-to-profound hearing losses further reinforces the false reality that mild and moderate hearing losses do not require professional care for the best outcomes.
Yes, this is another call-to-action to educate the government despite the efforts of lobbyists to direct them otherwise. And yes, professional associations will likely rise once again to this challenge. But, the consuming public and individual hearing health care professionals must raise their voices as well. Because, if an opinion goes unchallenged, it gains a clearer path to becoming a new reality.
As always, I enjoyed Dave’s perspectives. In particular, I agree with the premise that–in what appears to be several facets–the FDA and legislators seem to be disregarding hearing science, and/or they endorse several positions that have little or no scientific merit to back up their positions. However, I don’t think Dave’s intent was to imply that no one is speaking out for the hearing healthcare field; it’s just that too few are listening. While it may be true that no one responded to the provocations of the CES representative who was purposefully insulting (ie, sometimes it’s best just to ignore a deliberate jerk), there have been MANY publications, testimonies, submissions, and position statements from the Hearing Industries Association, professional organizations, and researchers addressing the topic of hearing loss severity and consumers’ difficulty in self-diagnosing hearing loss and the value of professional care. In fact, a lot of good scientific evidence on this issue exists, going back to George Gates’ Framingham longitudinal studies of the 1980s, or perhaps longer. Reams of evidence have been presented at the original accessibility/affordability meeting, as well as the PCAST, NASEM, and FDA and FTC workshop meetings, culminating in a consensus statement from AAA, ADA, IHS, and ASHA, as well as a comprehensive position paper from HIA (HR published an abridged version of this in May 2017). So, I think the overall point is: let’s make sure we consider the science when formulating the regulations!