For years, the primary goal of using FM amplification systems was to improve the listening and learning skills of children enrolled in classrooms with poor acoustics. Although numerous studies have proven the benefits derived in a classroom setting,1-4 the study and research on the benefits of FM systems when used by adults in everyday environments are lacking.
Advances in hearing instrument technology throughout the past decade have allowed manufacturers to improve the sound quality, as well as reduce the size of hearing instruments. The majority of hearing instrument users want to hear better in noisy situations.5,6 Enhancements in analog and digital hearing instruments—especially with directional microphones—have improved the signal-to-noise ratio (SNR) for many users, which in turn has increased their speech understanding in noise and user satisfaction.7-11 Along with these advances in hearing instruments has come an improvement in FM systems.
There are patients who require and want more benefit than even today’s advanced, directional microphone hearing instruments can provide. FM systems may provide improvement in the SNR of 15-18 dB,12 which is greater than the SNR improvement provided by directional microphone technology (typically 2-8 dB SNR). An FM system can be the answer for these people, especially if they are motivated to make full use of the system.
Candidates for the FM systems in the past often had very poor speech discrimination ability, severe-to-profound hearing loss, and auditory processing deficits. The FM systems can also provide excellent benefit to almost any hearing loss, mild to profound, and can be demonstrated to all patients. This study examined whether adults with mild-to-profound hearing loss would perceive greater benefit with an FM system when compared to the benefit derived from their existing hearing instruments alone.
|
An Example of an FM System for Adults The FM system used in this study was the MicroLink system by Phonak. This system has a receiver that is placed in an audio shoe or “boot,” and the boot is snapped onto the hearing instrument over the battery door (Figure 1). Each manufacturer has its own boot, and the FM receiver (called MLx) is attached with three prongs that snap into the three holes of the boot. A switch on the bottom of the receiver offers control with the options “off,” “FM-only,” and “FM plus hearing aid.”
The receiver is called the “universal receiver” because it can be used by different hearing instruments from different manufacturers. It can also be switched to a different hearing instrument from another manufacturer with a boot for that device. Therefore, if a patient is using “Hearing Aid A” with a MicroLink system, and the patient changes to “Hearing Aid B” from a different manufacturer, the MicroLink system can be used with the new aid. In this study, five different manufacturers’ products were used, demonstrating the versatility of the system. (Author’s Note: Many programmable or digital BTEs produced during the past six years are MicroLink compatible. Analog BTEs are usually compatible if they have direct audio input (DAI) capability.)
The FM system has a transmitter (TX3) that features a sliding switch with four positions: “off,” “omnidirectional,” “directional,” and “super directional.” The TX3 can transmit a signal up to 100 feet away from the receiver. In fact, we had patients who were able to have the signal transmit at even greater distances (up to 300 feet) on a regular basis. The patient adjusts the setting depending on the listening environment. The transmitter must be recharged daily and can function up to 10-12 hours daily. If the transmitter is not recharged every day, it will not function and will have to be charged continuously for 20 hours before any further use. During the initial fitting, we stress the importance of the recharging procedure. The transmitter can be worn around the neck, in a pocket, or set on a table. There is a coated wire antenna approximately 12” long attached to the transmitter. The authors found it beneficial to tape the antenna to the neck loop cord provided with the system. This keeps the antenna from moving around where it is prone to getting caught on clothing or other objects. We have had several patients who returned with the antenna broken or who had the protective tip come off. The TX3 can be plugged into external sources such as television, radio, CD players, etc. Judging from anecdotal reports, this feature has increased our study participants’ enjoyment of TV and music substantially. They have been amazed at how they can walk out of a room and still hear the music or TV program. It has added a lot of flexibility to their lives. Explanation of the system’s function needs to be thorough. The system is fairly easy to use and only one patient could not physically/mentally handle it. With approximately 25% of the patients, the first follow-up appointment was spent re-instructing or reiterating the instructions. This has occurred less as our staff has become more familiar with the system and improved on the counseling relative to the system. We also now repeat the instructions numerous times during the initial fitting session. For the user, there is a small downside regarding battery drain. The batteries in the patient’s hearing instrument will typically last only half as long while using the MicroLink as compared to the life of the battery using the aid alone. If a patient’s hearing aid battery lasted on average two weeks prior to the MicroLink, they should then expect only about one week of battery life while using the MicroLink with their aid. We did have one patient notice that this was exacerbated when using the MicroLink on the FM-only setting. There is also a new phone transmitter called the TX4 or Tel-Com (Figure 2). It is a conical space-age-looking device that attaches to the phone. It can also be used as an external sound source for television, radio, CD players, etc. This can serve as more of a permanent system than the TX3, which has to be hooked/unhooked from an external source. Therefore, a patient can have the TX4 plugged into the television, listening to a program with MLx receivers; when the phone rings, the television program is muted automatically by the TX4. The patient then picks up the phone and hears by way of the FM receivers being transmitted by the TX4. When the patient is finished with the phone call, he/she hangs up the phone and the television program comes back on automatically. The TX4 can be used for television, radio, stereo, or CD player, making it flexible for external sound sources. It also allows for binaural hearing on the telephone. Or, if the patient has good dexterity, he/she can have one ear listening to the phone and one to the room conversation, if needed. However, the TX3 and the TX4 cannot be used at the same time. The receiver can only handle information from one transmitter at a time. For example, a patient cannot have the TX3 on when trying to talk on the phone with the TX4. |

Study Method
The study’s 28 participants were all experienced users with behind-the-ear (BTE) hearing instruments. Of the 28 participants in the study, one patient was wearing analog aids, eight wore programmable, and 19 wore digital hearing aids. BTE devices used by the participants included: one Phonak analog power device; four Phonak 332 power AudioZoom; two Phonak 232 AudioZoom; two Phonak E-4s; three Siemens Prismas; three Siemens Signias; five Widex Senso’s; four Resound BZ5s; one Oticon Digifocus; and three Phonak Claros.
Twenty-two of the participants were binaural hearing instrument users and six were monaural hearing instrument users. Twenty participants were wearing devices with directional microphones. The majority of these patients utilized high-end technology devices with optimal SNR capabilities. They were already using exceptional devices that improved their hearing ability, but all were willing to try an FM system if there was the potential of improving their current benefit from the aids.
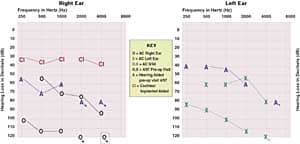
The study participants had the following hearing losses: mild to moderate (two users), mild to severe (four users), mild to profound (three users), moderate to severe (eight users), moderate to profound (three users), moderately severe to profound (four users), severe (one user), and severe to profound (three users). These same participants had the following speech discrimination: 0%-20% (two users), 20%-40% (three users), 40%-60% (four users), 60%-80% (nine users), and 80%-100% (10 users). The average speech discrimination ability of all 28 participants was 74%.
Results
Patients were asked to judge how they were hearing with their existing hearing instruments in nine different listening environments prior to wearing the FM device, including:
- Sound quality of the device
- Listening to a female voice in quiet
- Listening to a male voice in quiet
- Listening to 4-10 people speaking simultaneously
- Listening to music
- Listening to a lecture or sermon
- Listening in a restaurant environment
- Listening at a distance
- Listening in a car
The subjects were to judge their own hearing performance in each of these environments as poor, fair, good, or excellent. After wearing the MicroLink FM system for 3-5 weeks, the subjects were asked again to judge the benefit between hearing with the FM system plus the hearing aid (FM+HA) in the nine listening environments. Each rating was assigned a numerical score: poor=1, fair=2, good=3, and excellent=4.
We felt the above nine environments sufficiently represented situations patients encounter on a regular basis. We analyzed the data by comparing the perceived benefit of the FM system between the following groups:
- Overall benefit of all participants (28 total);
- The subjects who elected to purchase the FM system (20 total);
- The subjects who did not purchase the FM system (8 total).
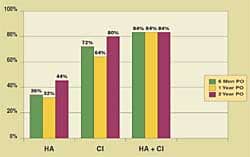
The overall judgments are determined in Figure 3. In every listening environment, the patients judged their hearing to be improved in the hearing aid and FM condition compared to the hearing-aid-only condition.
The largest improvement in subjective benefit came in what patients deemed as the four most difficult listening environments: lecture or seminar, restaurant, at a distance, and in a car. Patients most often complain about hearing in these specific situations and the FM system proved to be a suitable solution for these patients. Remember, 73% of our study participants were already wearing hearing instruments with directional microphone technology, which is aimed at improving listening in these difficult situations. Therefore, the FM system provided even more benefit for these patients in these common, difficult listening environments.
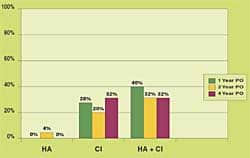
The judged benefit received in the different listening environments becomes even more significant when we compare the group that kept the FM device (Figure 4, page 29) versus the group that did not keep the device (Figure 5, page 29). Those who kept the FM system judged their benefit in the first four listening environments at an average level of 2.5 with their aid(s) alone versus a level of 3.0 with the FM+HA (when judged on the scale of 1-4 mentioned previously). The four most difficult listening situations are where the subjects noticed the most improvement with the FM+HA system when compared to wearing their hearing aids only. Benefit improved from an average of 1.6 (aid alone) to a level of 2.8 with the FM+HA. Therefore, the benefit in the more difficult listening environments was more than twice that of the quieter situations.
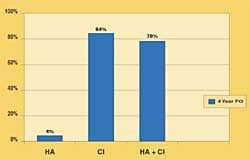
Those who chose not to keep the FM system (Figure 5) still judged their hearing to be improved in all but one listening environment when using it. In the music environment, they judged their hearing the same with their hearing aid alone as with the FM+HA. The group that did not keep the FM system judged the benefit in the first four listening environments at an average level of 2.3 with aid(s) alone versus a level of 2.7 with the FM+HA. In the most difficult listening situations, benefit improved from an average of 1.6 (aid alone) to a level of 2.0 with the FM+HA. Even though these patients did not elect to keep the FM system, they all indicated that their hearing improved with the FM+HA compared to the hearing aid by itself.
Patient Comments
Comments (both good and bad) from our patients about the FM system provide additional insight into the use of FM devices in a private dispensing practice.
Positive comments/scenarios
• One patient who works as a CEO wanted multiple TX3s: one for his secretary, one for his wife who worked in his office, and one for his office manager Unfortunately, this is not currently possible. The receiver can only get input from one transmitter at a time, or it can be done in a “daisy chain,” which is very difficult at best.
• One man had a dead ear on his right side and was aided on his left ear with a new Siemens Signia. His wife had a paralyzed vocal cord that made it very difficult for them to converse with one another, especially when he was driving their car. He was provided with an FM device just before they departed for vacation, which included a 6-hour car ride. He returned the following week with a check in-hand and said, “This is the first time my wife and I have been able to talk in the car for years.”
• A patient had a flat 70-80 dB hearing loss bilaterally with 8% and 12% speech discrimination wearing Phonak 332 AZ. He tried the FM system and returned after 2 weeks. He said: “I went to my club meeting with eight of us around the table and set the TX3 on the table. I was involved in the conversation for the first time since my sudden hearing loss.”
• A patient was wearing Widex Senso instruments for 4 years. He had a moderate-to-severe bilateral loss with 40% and 48% discrimination. He and his wife own an apartment building. The second day wearing the device he was outside raking leaves and his wife was inside the building (with the TX3 in her pocket). She was speaking with a tenant who had a problem with his apartment. She mentioned that needed to go get her husband from the yard. Before she turned to get him, he was already on his way (having heard the conversation take place). His wife was stunned that he could hear her talking at such a distance (Note that all users of the system need to be aware of these capabilities.)
• A patient who uses 332 Power AudioZooms with 8% and 20% discrimination had not been able to use the phone for the past few years. After using the TX4, he has been able to communicate on the phone and he feels that his understanding on the phone is now about 95%.
• A patient with a severe-to-profound unilateral hearing loss with 28% discrimination has been struggling to use the phone. He tried the TX4 and this allowed him to hear well on the phone for the first time in many years.
Negative comments/scenarios:
• One man mentioned he was afraid of losing the TX3 or the receiver. He also worried about leaving the TX3 somewhere like a restaurant and then not remembering where he left it.
• A patient felt that the design was poor because the antenna should be internal or more like a cell phone antenna. She also did not like to have to put the TX3 around her neck—or anyone else’s for that matter.
• There was almost universal agreement on the instructional booklets, with most citing that the booklets were confusing. Because of this, the staff actually found more success if we did not provide the patient with the system’s written instructions. Instead, they were asked to call us or ask us questions at follow up visits.
Cost of the Devices
The MicroLink system is a rather expensive device for the patient to purchase with the suggested retail in the $2,600-$3,600 range depending on monaural and binaural use. Note that this cost does not include the patient’s hearing instruments. However, when a patient comes in with fairly new BTEs and asks the typical question, “So what’s newer and better than what I have?” the MicroLink is an excellent alternative to discuss with the patient.
If a patient is already wearing a MicroLink-compatible hearing instrument, then demonstrating it to the patient is worthwhile. There is now a demonstration TX4 that can easily be set up in an office. We found letting a patient try it for a month with a demonstration unit was the most successful way of showing its benefits.
Potential Future Improvements
There are probably two issues we feel can be improved on with this technology. The first is to create a new antenna that is thicker and shorter (more like a cell phone antenna). Phonak reports that this modification is in the planning stages and will be available sometime in the future. The other is improvement of the instructional booklets given to the patients.
A third wish would be that FM capability becomes available in ITEs—and eventually in half-shells and ITCs, if possible—in the near future. This would improve the hearing ability of our patients in many ways, especially in noisy listening environments, with the telephone, as well as when listening at a distance. We believe that the company with this capability in its product line will certainly have an added, worthwhile advantage to offer patients.
Summary
This study found that adults with mild-to-profound hearing losses can wear an FM system and receive excellent benefit in a variety of listening environments. The improvement found in restaurants, lectures, in a car, and at a distance was found to be the most significant for hearing impaired adult patients. These difficult listening situations are where most people with hearing impairment struggle to hear clearly.
We have found the FM system described here to be a beneficial option for those patients who are not satisfied with their current BTE instrument(s) when faced with challenging listening situations. Twenty of the 28 subjects in this study (71%) elected to purchase the FM system.
The study also shows that FM technology represents a valuable solution when a patient is already utilizing high-end directional technology and is still desiring added hearing benefit in challenging listening situations. FM systems—although traditionally used for children in classrooms—are a useful, available technology that adults can also use to significantly improve their hearing in difficult listening environments.
Acknowledgements
Author’s Note: CSG/Better Hearing Center received no special treatment or benefits from Phonak for writing this article. Each study participant who decided to keep the FM device, paid for it in full. We performed this study because we felt there has not been sufficient data generated relative to FM system benefit for adults in typical listening environments.
We would like to thank David Wessell and Liz Brassine of Phonak for providing the graphics of the MicroLink system in this article and for some clarifications regarding the product.

|
References
1. Crandell C, Smaldino J. Classroom acoustics and amplification. In: M Valente, R Roeser, H Hosford-Dunn, eds. Audiology Volume II: Treatment. New York: Thieme Medical Publishers; 2000.
2. Crandell C, Smaldino J. When hearing aids are not enough: assistive technologies for the hearing impaired. In: R Sandlin, ed. Handbook of Amplification. San Diego: Singular Press; 2000.
3. Crandell C, Smaldino J. Room acoustics and assistive technologies. In: Katz, ed. Handbook of Clinical Audiology. San Diego: Singular Press; 2000.
4. Crandell C, Smaldino J, Flexer C. Soundfield amplification: a theoretical foundation and practical applications. San Diego: Singular Press; 1995.
5. Kochkin S. Customer satisfaction and subjective benefit with high performance hearing aids. Hearing Review. 1996;3(12): 16-26.
6. Stock A, Fichtl E, Heller O. Comparing determinants of hearing instrument satisfaction in Germany and the United States. Suppl to Hearing Review, 1997; 2(suppl):40-46.
7. Agnew J, Block M. HINT thresholds for a dual-microphone BTE. Hearing Review. 1997;26;29-30.
8. Valente M, Fabry DA, Potts LG. Recognition of speech in noise with hearing aids using dual microphones. J Amer Acad Audiol. 1995; 6:440-9.
9. Voss T. Clinical evaluation of multi-microphone hearing instruments. Hearing Review. 1997; 36;45-46, 74.
10. Schuchman G, Valente M, Beck L, Potts L. User satisfaction with an ITE directional hearing instrument. Hearing Review. 1999;6(7):12, 16, 21-22.
11. Valente M, Sweetow R, May A. Using microphone technology to improve speech recognition. Suppl to Hearing Review, 1999; 3(suppl):10-13.
12. Larsen M, Brenner C, Warland A. Multimicrophone instruments, DSP and hearing-in-noise. Hearing Review. 1990;5(7):42-45.
Correspondence can be addressed to HR or Mark J. Sanford, MS, CSG/Better Hearing Center, 31 Panoramic Way, 1st Floor, Walnut Creek, CA 94595; email: [email protected].


