
Tech Topic | January 2015 Hearing Review
A discussion on recent findings regarding the value of CROS/BiCROS systems, as well as a field study that suggests how the use of a Mini Microphone to stream sound from the poorer to the better ear may provide benefit.
It has become common practice in audiology to fit hearing instruments bilaterally when the hearing loss warrants amplification of both ears. This has changed dramatically during the last two decades, with only 25% of the fittings in the United States being bilateral in 19821 to about 84% of the fittings being bilateral today.2
Bilateral hearing aid fitting makes intuitive sense; after all, we have two ears. Binaural hearing effects resulting from input from both ears, such as improvement in horizontal localization, binaural squelch, binaural summation and redundancy, are well documented. Furthermore, these effects apply to hearing- impaired individuals as well, and thus provide evidence for bilateral hearing aid fitting.1,3
However, not all hearing aid users can enjoy these benefits. Hearing aid users who cannot benefit from bilateral hearing aids include those with normal hearing in one ear and an unaidable hearing loss in the other—referred to as unilateral sensorineural hearing loss (USNHL). Asymmetric sensorineural hearing loss (ASNHL) refers to a hearing loss that is aidable in one ear and unaidable in the opposite ear.3 The term single-sided deafness (SSD) can be used inter- changeably for both USNHL and ASNHL.4
Over time, patients with hearing losses such as these learn to employ coping mechanisms, including preferential seating and making adjustments so that the speaker is positioned toward the better ear.5 While use of these techniques is beneficial, sometimes it is not possible to overcome difficult listening environments.
SSD can be addressed with contralateral routing of sound (CROS) and bilateral contralateral routing of sound (BiCROS). By sending the sound arriving at the unaidable ear to the better ear, the head-shadow effect can be reduced; however, listening in noise can still be a challenge. Placing a microphone on the poor ear can introduce noise to the better ear and potentially spoil the signal. Listeners with USNHL reported that they most frequently used their CROS aid in group conversations; however, they found that the quality was best in quiet.6
Listening in noise or groups is particularly problematic for patients with ASNHL because hearing in both ears is compromised. Oeding and Valente3 reported that the degree of hearing loss in the better ear impacted the listeners’ performance during speech-in-noise testing. Patients with better hearing in the aidable ear were found to perform better in both the unaided and aided CROS conditions compared to those in a BiCROS who showed no significant difference between conditions. Subjective results, however, did indicate that participants perceived benefit from the aided condition.
Another study of CROS users7 found that the performance on the Hearing in Noise Test (HINT) was deteriorated when noise was presented to the transmitter ear.
There are few studies published that speak to the efficacy of CROS or BiCROS hearing aids. However, for those that exist, the data is conflicting.4 When comparing speech-in-noise thresholds of two CROS/BiCROS systems with unaided and monaural fitting on the better ear, Williams et al4 showed all of the aided conditions resulted in lower levels, or improved hearing; however, there was no significant difference in performance between the CROS/BiCROS conditions and monaural fitting. It was also reported that adding advanced algorithms, such as directionality, improved the patient satisfaction ratings of the CROS/BiCROS. Perceived benefit with advanced features without objective support is in agreement with the Oeding and Valente3 trial in which noise reduction was added as a feature. The authors of both studies suggest that this may be a result of a placebo effect.
Lack of supporting evidence in the literature, the possibility of making difficult listening situations even worse, and the relatively high cost of CROS products have led clinicians and patients to explore other solutions. Sound transmission through bone conduction via a bone-anchored hearing aid (BAHA), bone conduction aid, or transcranial CROS (TCROS) offer solutions to SSD. Unfortunately, these systems also have drawbacks, making the BiCROS systems the most commonly used method for achieving sound awareness from the unaidable side.4 While successful in providing access to sound from the “deafened” side, it is impossible to completely restore binaural hearing with these methods. However, as mentioned previously, there can be value in the perceived benefit in particular cases.
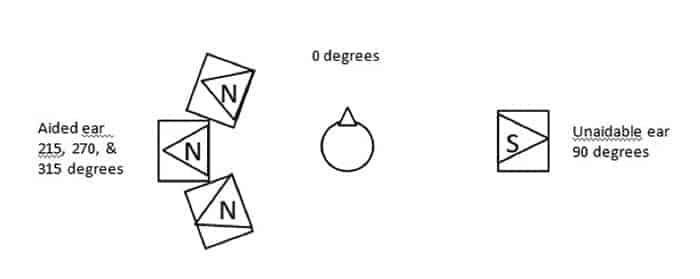
Figure 1. Test set up for OLSA. “N” indicates noise presentation and “S” indicates speech presentation. Each speaker was able to send out its signal without shadow-effects. Signals were presented with delays to produce a diffuse impression.
A trial exploring the use of the ReSound Unite Mini Microphone (hereafter referred to as “Mini Microphone”) for SSD was conducted at Giessen University in Germany in order to investigate possible “off label” uses for the device. A field and lab trial including 10 participants with SSD was completed over a 5-week time period. The purpose of this trial was to: 1) Determine whether adding the Mini Microphone to the unaided side of a monaural fitting improved the audibility of speech in noise, and 2) Investigate perceived benefit while using the Mini Microphone in addition to a hearing instrument on the aidable ear.
Methods
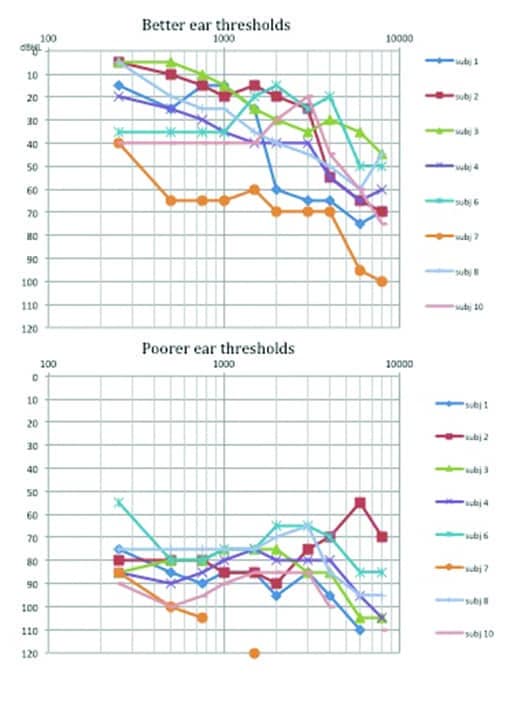
Figure 2a-b. Air conduction thresholds of better (top) and poorer (bottom) ears of test subjects.
Participants were recruited based on hearing thresholds. Criteria for the aidable ear required the hearing loss to be within the recommended fitting range of a ReSound Verso 962 receiver-in-the-ear (RIE) hearing instrument. Therefore, participants exhibited degrees of hearing loss ranging from mild to severe (Figure 2a, top panel). The first week post-fitting was set as an acclimatization period before the 4-week trial began. All fine-tuning of gain settings was established during this time. Participants were divided into two groups. One group would wear the hearing instrument on the aidable ear only, and the other group would use the hearing instrument along with the Mini Microphone to assist in collecting sound from the unaided side.
The Mini Microphone sends the signal wirelessly to the hearing aid, similar to a wireless Bi/CROS system. Two weeks were designated for the hearing-aid-only portion, while the other 2 weeks incorporated the Unite Mini Microphone. Between the second and third visits, the groups switched conditions.
Outcome measures included a comparison of speech-in-noise testing, the Speech, Spatial and Qualities of Hearing Scale Comparative version (SSQ-C) after the completion of both conditions, and a Mini Microphone specific questionnaire (MMQ) after the condition incorporating the use of the Mini Microphone. The subjective measures were selected and designed to elicit each subject’s experiences, expectations, specific use cases, and opinions regarding the hardware after using the Mini Microphone.
A lab trial was conducted during the fourth session for the speech-in-noise testing. The Adaptive Oldenburg Sentence Test (OLSA) was administered twice per participant: once while wearing the hearing instrument only, and again with both the hearing instrument and the Mini Microphone positioned at the unaided side. Participants wore the Mini Microphone clipped to their shoulder or chest pocket. Speech was presented to the unaidable ear while ICRA5-250 noise at 60 dB SPL was simultaneously presented to the aided ear as shown in Figure 1.
Results
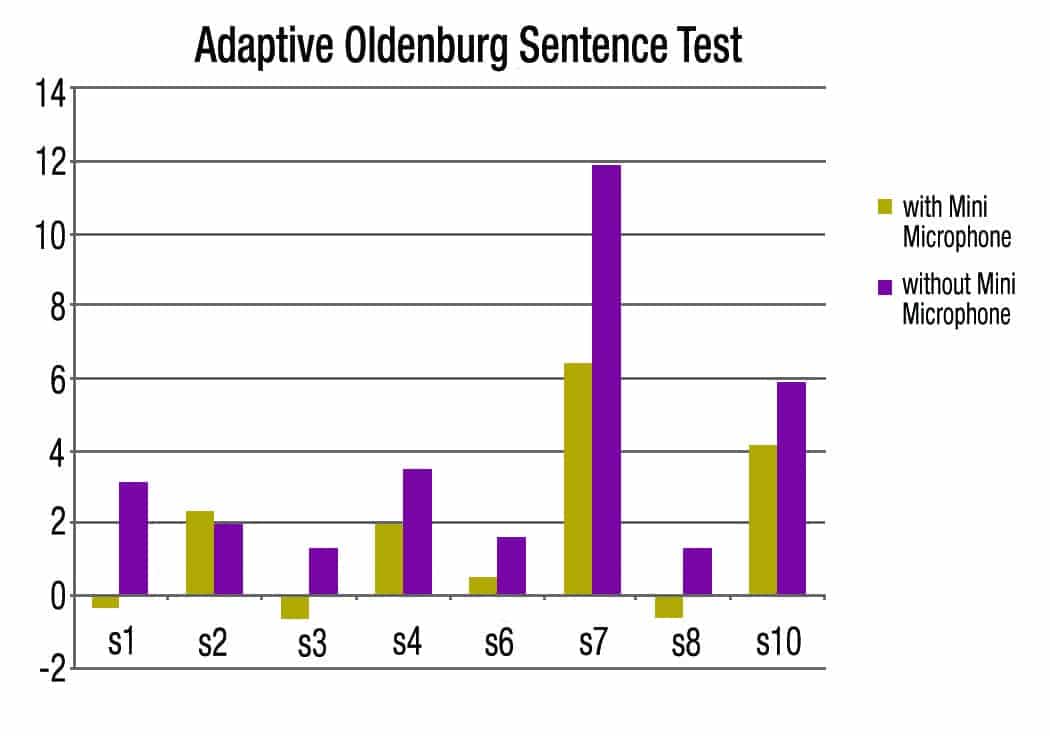
Figure 3. OLSA scores per subject with and without the Mini Microphone, with seconds on the x-axis and dBSNR on the y-axis.
Eight test subjects with SSD completed the trial. Better ear hearing thresholds for the 8 subjects were within the fitting range of the Verso 962 RIE fit with an “S” receiver, with the exception of Subject 7 who was fit with a high-power receiver. Own hearing aid usage varied among subjects. Three participants only aided the better ear, 3 aided the poorer, and 2 wore devices on both ears consistently.
Seven of the 8 subjects demonstrated an improvement in speech-in-noise test scores when wearing the Mini Microphone. Mean scores for hearing-instrument-only and instrument-with-Microphone conditions were 3.8 dB and 1.7 dB SNR, respectively. A lower SNR result on the OLSA test indicates better performance.
The Mini Microphone is packaged with a lanyard and a built-in clip, and subjects were encouraged to try different placements to find the optimal position for each particular listening situation. Subjective data was collected via the SSQ-C and the MMQ. On the MMQ, 5 of the 8 subjects reported they most frequently used the Mini Microphone clipped at the unaided side because they felt they achieve the most benefit with this placement. Three participants primarily used the lanyard, resulting in a placement in the middle of the chest. Six of 8 subjects reported general benefit. It was noted that both of the participants who did not claim benefit wore the Mini Microphone all hours but with the lanyard and placement at the middle of the chest.
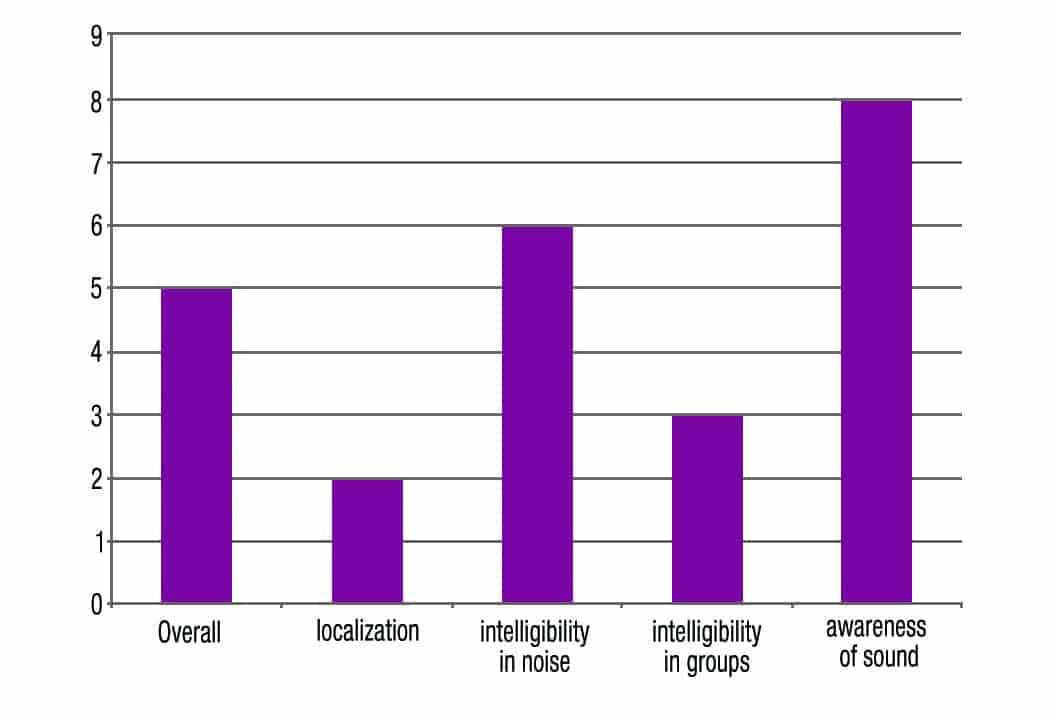
Figure 4. Number of participants reporting benefit on the Mini Microphone Questionnaire.
As shown in Figure 4, most subjects found that the Mini Microphone provided more awareness of environmental sounds. Six responded there was improvement while listening to speech in noise. Three reported benefit in groups and two with localization.
The SSQ-C questions are grouped by categories of speech intelligibility, spatial hearing, and quality of hearing. Participants are asked to rate their experience with the Mini Microphone on a scale of “5 to 5” compared to their experiences without. Positive ratings indicate benefit from the Mini Microphone, and negative ratings reflect greater benefit with the hearing instrument only. Ratings of “0” indicate no difference between the two conditions.

Figure 5. The sum of all ratings in the SSQ C, by category. Subjects were asked to rate their experience with the Mini Microphone on a scale of 5 to -5, with positive ratings indicating greater benefit from the Mini Microphone, and negative ratings indicating greater benefit from the hearing instrument only condition. A rating of “0” indicated no difference.
Figure 5 shows the sum of points per category. When combining the positive and negative ratings, it is clear that there was an overall positive outcome of using the Mini Microphone.
Another way to examine the data is to simply count the number of positive, negative, and indifferent responses per category. When this is done, it becomes apparent that most often there is no difference between conditions in the field (Figure 6). At the same time, there were many more situations where using the Mini Microphone was rated as being better than the hearing instrument alone.
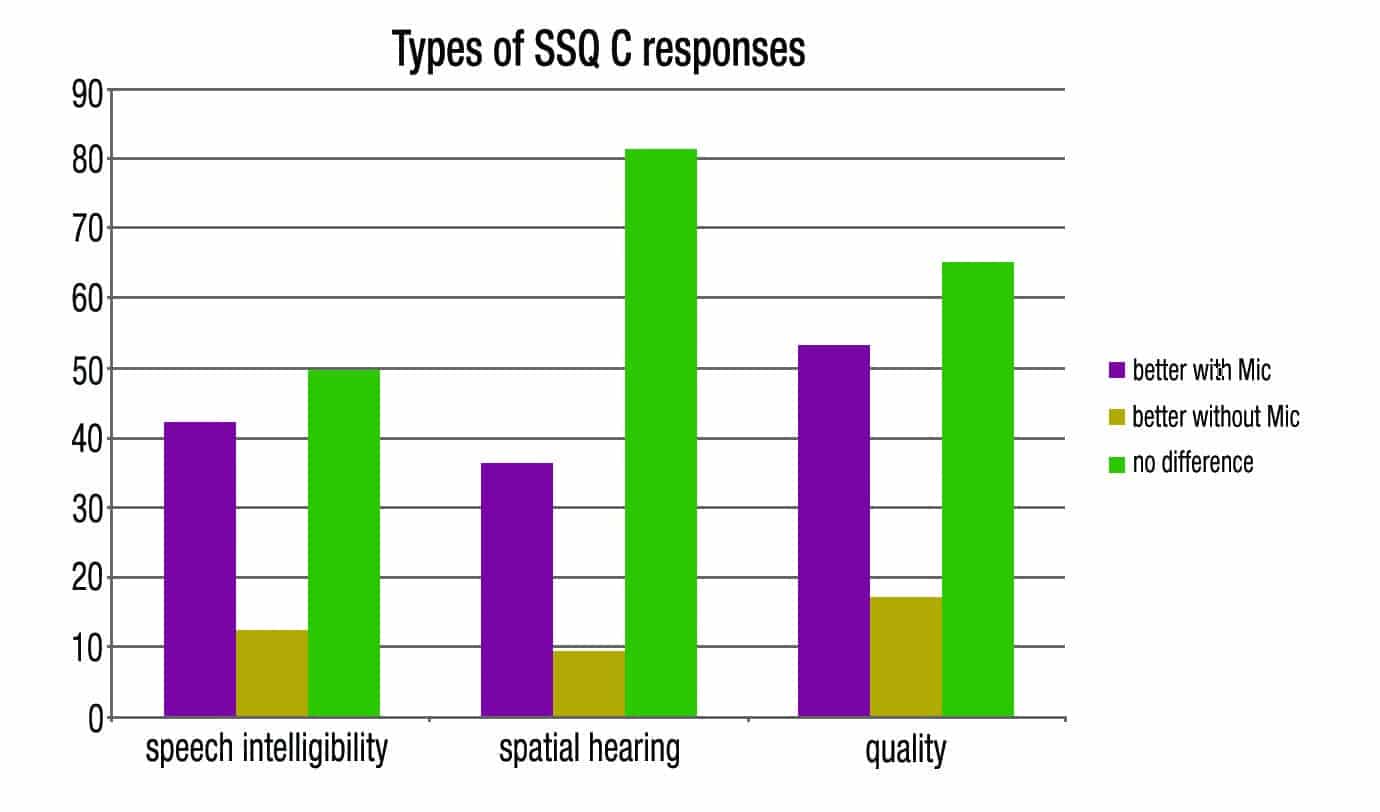
Figure 6. The quantity of types of responses on the SSQ C, per category.
Use Time
Subjects were instructed to use the Mini Microphone as they saw fit during the field trial. Wear time for the hearing instrument and the Mini Microphone was recorded by the participants. The mean use time of the hearing aids was 8.3 hours per day, including 5.6 hours of Mini Microphone use. While most used the hearing instrument more hours than the Mini Microphone, 3 participants used the hearing aids and Mini Microphone an equal number of hours per day. Two of these subjects were the only ones to report no benefit in noise on the questionnaire. Conversely, all subjects who used the Mini Mic part time, or as needed, felt that using the Mini Mic resulted in better speech understanding in noise and greater overall benefit.
Discussion
While it is not possible to draw sweeping conclusions with a small number of participants, it is of interest to consider individuals and why some reported benefit or a preference for using the Mini Microphone while others did not. Subjects 4 and 8 reported that using the Mini Microphone was beneficial, but subject 4 indicated greater benefit on both subjective and objective measures. Both subjects own hearing instruments for their right and left ears. However, Subject 4 typically does not wear the device on the poorer ear, and felt that the trial devices provided an improvement. Conversely, Subject 8 wears both instruments on a more regular basis, compared to Subject 4 who only aided the better ear.
Experience and satisfaction with their own devices may have impacted their individual judgments of using the Mini Microphone. Subject 8 typically wore two instruments. Removing one may have caused a condition that was not preferred overall.
During the trial period, these subjects wore the hearing instrument throughout the day, but differed in their use of the Mini Microphone. Subject 4 reported improvement in specific situations, such as when the speaker was toward the poorer ear and in small group conversations. This subject also reported lowering the volume on the Mini Microphone in “party situations” because the music was too loud. This same person wore the hearing instrument 8 hours per day, while the average use of the Mini Microphone was only 2 hours. This indicates that the Mini Microphone was only used when there was a perceived need and not worn throughout the entire day.
Subject 8 reported benefit in quiet environments like watching television but was not pleased with the Mini Microphone in noise. This person wore both the hearing instrument and the Mini Microphone simultaneously throughout the day. Simply wearing the Mini Microphone in all listening environments, without manipulating the volume control, was likely the cause for the poorer ratings.
Subject 4 consistently reported improvement on the SSQ with the Mini Microphone when compared to with and without own device, while Subject 8 did not. Both subjects realized benefit during OLSA testing, but in the case of Subject 8, this was not validated in the field trial.
AccordingtoValente,5 introducing sound from the poorer side may not always be beneficial, and the wearer should have control over the device by either a volume control or an on/off switch. He recommended that CROS amplification be used judiciously and should not be worn if it is merely adding noise. Based on this recommendation, it could be anticipated that noise reduction on the transmitter ear would be a helpful feature. Oeding and Valente3 investigated the implementation of a noise-reduction algorithm on the transmitter ear, and reported that the feature did not increase speech perception. It was suggested that a noise detector that would turn off the microphone on the transmitter ear could be of benefit. This implies that a “full-time” CROS solution may not always be desirable.
The Mini Microphone does offer the flexibility of a volume control, but also offers some versatility beyond the capability of a CROS system. It does not have to be worn by the listener but can be worn by the speaker instead. This may be particularly valuable in a lecture scenario, when conversing with one individual in a noisy environment like a restaurant, or even in the car if the unaided ear is toward the conversation partner. The voice of the speaker is then sent directly to the individual wearing the hearing instrument. The Mini Microphone also offers an input jack. Items such as music players and cell phones can be directly connected to the Mini Microphone, which wirelessly streams the signal to the hearing aid and thus adds utility for the wearer in more situations.
Summary
Data regarding amplification solutions for SSD is scarce, and the data that does exist suggests benefit using CROS systems in particular cases. It is not uncommon for objective and subjective data to conflict. Patient factors, such as thresholds of the better ear, current use of amplification, and willingness to work with a solution, can all impact the success of a CROS fitting.
It does appear that using a transmitter on the unaidable side is beneficial, but not in all environments. If the transmitter is equipped with a volume control and an on/off switch, at minimum,it is more likely to yield end-user benefit.
The ReSound Unite Mini Microphone can be a viable less-expensive option for those with SSD, allowing access to sound on the unaidable side. It conveniently includes a volume control and audio input options, in addition to its ability to be used as a remote microphone.
The small study presented here found that use of this device to stream environmental sound from the poorer-hearing ear side to a hearing aid on the better ear does provide better hearing in noise in a controlled setting, and that it generated positive responses from the majority of participants during the field trial compared to wearing only a hearing aid on the better ear.
 Erica D. Koehler, AuD, and Mallory Maine, AuD, are research audiologists at GN ReSound Global Audiology in Glenview, Ill. Alexandra D. Pastoors-Gebhart, and Jürgen Kiessling, PhD, are associated with the Department of Audiology at Justus-Liebig-University Giessen, in Giessen, Germany.
Erica D. Koehler, AuD, and Mallory Maine, AuD, are research audiologists at GN ReSound Global Audiology in Glenview, Ill. Alexandra D. Pastoors-Gebhart, and Jürgen Kiessling, PhD, are associated with the Department of Audiology at Justus-Liebig-University Giessen, in Giessen, Germany.
Correspondence may be sent to Dr Koehler at: [email protected]
Citation for this article: Koehler ED, Maine M, Pastoors-Gebhart AD, Kiessling J. Another win for wireless accessories: Hearing aid and remote microphone combination for SSD. Hearing Review. 2015;22(1):26-29.



