
Who should receive unilateral fittings, and how should you fit them?
Fitting Tips: Unilateral Hearing Loss | Hearing Review July 2014
Unilateral hearing loss (UHL) is common, and without intervention it can lead to academic, speech-language, and social-emotional difficulties. But there is only limited literature about hearing aid fitting for these patients. Here is a brief review and some considerations when fitting patients with UHL.
It used to be that monaural hearing aid fitting was the standard of practice (Figure 1). About 78.2% of hearing aid fittings were monaural in 1984. In the ensuing years, as the benefits of binaural hearing aid fittings became apparent, the proportion of monaural-to-binaural fittings did a dramatic flip-flop. As of 2008, only 25.7% of total hearing aid fittings were monaural in the United States. For people with bilateral hearing loss, only 10.2% are fitted monaurally.1 Some of these include individuals who have an unaidable ear.
This indicates that the majority of people today who are fit monaurally with hearing aids are those with unilateral hearing loss (UHL). UHL is defined as a loss in one ear of any degree (mild to profound) regardless of the type of hearing loss. Permanent conductive, sensorineural, and mixed losses are all included in the definition. The incidence of UHL is estimated to be 0.8 to 2.7 per 1000 in newborns, 30 to 56 per 1000 in school-aged children, and 7.9% in adults. UHL accounts for half of adults with hearing loss.2,3
Children and UHL
There has been tremendous interest in researching the impact of untreated UHL on children. Research shows sound localization test scores were significantly poorer for the children with UHL than for the children with normal hearing. These localization difficulties increased as the degree of UHL increased. The children with UHL also had significantly poorer speech-recognition scores than their normal-hearing peers. Other researchers have documented poor speech-recognition performance of children with UHL when measured in the presence of background noise.4
Recent research indicates school-aged children with UHL demonstrate worse oral language scores (worse language comprehension, oral expression, and oral composite) compared with siblings and normal-hearing age peers.5 Academically, children with UHL have been found to perform more poorly than their normal-hearing counterparts. In a study of 60 children with UHL, Bess and Tharpe6 found that 35% of the children had repeated at least one grade in school, and an additional 13.3% required resource assistance, such as academic tutoring.
Although the choice to fit infants with moderate or greater degrees of bilateral hearing loss has become standard practice, the decision of whether to fit amplification to children with UHL is less clear. We do not yet know which children are at greatest risk for educational problems nor do we know which interventions are most effective at ameliorating these problems.7
In one report of 46 children ages 6 to 12 years with UHL, only half of the children had ever tried any form of amplification: 13 (28%) had used a FM system; nine (20%) had used a conventional hearing aid; and three (7%) had used Contralateral Routing of Offside Signals (CROS) hearing aids. Only one additional child had tried using a frequency modulation (FM) system and conventional hearing aid over the course of the study, even though the majority of these children had severe-to-profound UHL.8
With the introduction of universal newborn hearing screening, UHL can be diagnosed within the first 3 months of life. It has been shown that fitting of aids soon after identification can minimize language delay; however, there can be a delay of up to 7 months in provision of amplification for children with mild and UHL.
There is also a low compliance in hearing aid use among children with UHL. One important concern for children with UHL is auditory deprivation. Auditory deprivation has been described as more marked if it has an early onset (1-2 years) in individuals with UHL.9
The treatment of UHL can include sound field systems, FM systems, traditional hearing aids, CROS hearing aids, bone-anchored hearing aids (BAHA), and even a cochlear implant depending on the type, configuration, and degree of hearing loss. In this article, we will only discuss the fitting of conventional hearing aid amplification.
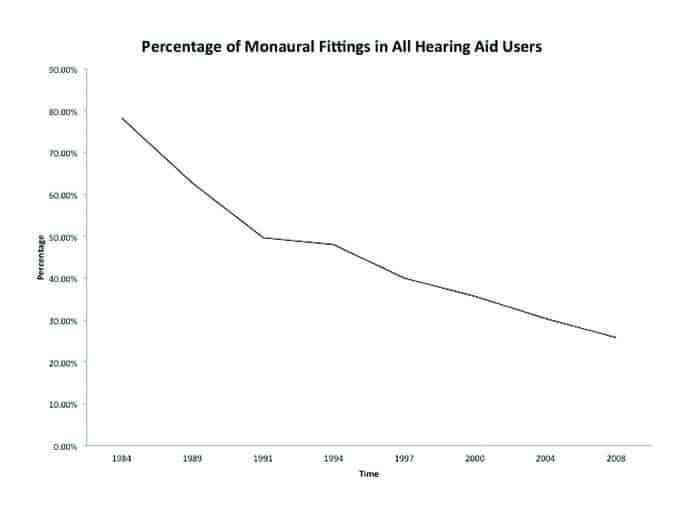
Figure 1. Percentage of monaural fitting in all hearing aid users from 1984 to 2008 (data from MarkeTrak VIII).1 (click to enlarge image)
Benefits of Hearing Aids
The benefits of hearing aids include increased audibility, minimizing of auditory deprivation, as well as ease of listening in both quiet and noisy listening conditions. It can also help binaural processing of sound.
Johnstone and her colleagues10 investigated the sound localization acuity of children with mild-to-severe UHL ages 6 to 14 years who wore a hearing aid in the impaired ear. Their results showed that a hearing aid can provide bilateral localization benefit to some children with UHL. Localization acuity in younger children with UHL was significantly improved, but not in the group of older children; time of intervention is also a main factor affecting the localization benefit. Children who were fit earlier showed bilateral benefit, whereas children who were fit later showed bilateral interference. And, without hearing aid amplification, localization performance in children with UHL rarely equals that of peers.
Fitting of hearing aid amplification is indicated for some people with unilateral hearing losses. The decision to fit a patient with unilateral hearing loss should be made on an individual basis, taking into consideration the person’s or family’s preferences, as well as audiologic, developmental, educational, and communication needs.
Patient use of hearing aids is related to the degree of hearing loss. Those with moderately severe or better UHL are likely to accept the use of a hearing aid, whereas those with a severe or profound UHL may not comply with hearing aid usage at all.
Regarding timing, older children and adults with UHL who are identified as candidates should be fit with amplification as soon as possible. For infants, there is still debate whether they should be fit before or after 18 months of age. On the one hand, it is unknown what degree of UHL may result in auditory deprivation and what is the critical time to provide amplification thereby avoiding these effects. On the other hand, more reliable hearing test results can be obtained from children over 18 months of age.9
Fitting Considerations & Rationale
Should hearing aids be fit differently for patients with UHL than for those with bilateral hearing losses? There is no easy answer to this question.
It should be noted that current prescriptive methods are specifically studied and designed for people with bilateral hearing loss. Although the prescription may provide targets for a monaural versus binaural fitting, it might not specifically address the needs of people with UHL. That is, we do not yet know if people with UHL prefer the gain generated by a prescriptive method designed for monaural fitting of a bilateral hearing loss.7 But we can get some inspiration from fitting experiences with asymmetrical hearing loss.
When doing the initial fitting, be aware that some software will default to a monaural fitting prescription when only one hearing aid is connected if the fitting rule incorporates a binaural correction. NAL-NL2 is an example of a prescription that provides binaural correction for both pediatric and adult patients, while DSL 5.0 only has a binaural correction for adults. For patients with UHL, the opposite ear is a good ear. Thus, any binaural correction should be used even though only one hearing aid is being fit to compensate for binaural summation effects.
As mentioned, the literature on fitting of asymmetric hearing loss can inform how to fit UHL. The goal of fitting asymmetric losses is to provide amplification that results in the perception of a fused auditory image rather than the patient hearing two different sounds from each ear.11
One technique12 to achieve the goal of binaural fusion or balance for fitting an asymmetric hearing loss can easily be applied to fitting UHL. First, find the most comfortable level of the better ear. This will provide a reference to adjust the gain setting of the poorer ear hearing aid. Then, ask the patient about where they perceive your voice to be coming from when you are sitting in front of him or her. Increase or decrease gain accordingly until the patient reports hearing your voice at the front and center of the head. This will guarantee the sound from both ears is balanced. The gain of the poorer ear can be further adjusted according to the patient’s preference.
Hearing Aid Features
Whether hearing aids should be fit differently for those with UHL also extends beyond the gain-frequency response prescription to features of the hearing aids.
Volume control. The most obvious place to begin this discussion is with on-board controls. While a program button to access multiple listening programs may be of little relevance for patients with UHL, a volume control is a must. This is because it won’t be known how the poor ear with amplification will interact with the good ear in real-world situations. The patient should have the opportunity to make volume adjustments to match the good ear.11 For young children, the volume control may need to be deactivated for safety concerns.
WDRC. Wide Dynamic Range Compression (WDRC) is always the preferred choice for UHL. WDRC will automatically adjust the gain of the hearing aid based on the input sound level to ensure natural perception of loudness. Soft sounds will be soft but audible, and loud sounds are perceived as loud but not uncomfortable.7 There is evidence that audibility is improved and speech recognition is either maintained or improved with WDRC as compared with linear amplification.13
Directional mics. Directional microphones can be fitted according to the patient’s communication needs for adults with UHL. For children, the use of directional microphone may be beneficial in some listening situations, such as when the target signal is located in front of the listener; however, decreased performance with directional response has been noted when the target signal was located to the side or behind the listener. The use of directional microphones should be based on the child’s ability to orient toward the target signal.14
Children’s limited experience with receptive speech and the importance of overhearing will limit the use of directional microphones. When a directional microphone is used, it is recommended to keep it in the automatic mode. There is some evidence that directional microphones in the automatic mode will switch appropriately between a directional and omnidirectional response for the given environment approximately 90% of the time. Even if the microphone is in the “wrong” mode 10% of the use time, it is still likely that the child will experience significant overall benefit.7
Wireless accessories. People with UHL also may benefit from hearing aids with digital wireless capabilities. Such hearing aids can receive an audio signal from a remote location to improve signal-to-noise ratio (SNR) and can be of particular benefit when listening in noisy environments. An example of a wireless accessory that could be used for this purpose is a companion microphone that can be held or worn by a conversational partner or speaker-of-interest. The speaker’s voice will be picked up by the microphone and transmitted wirelessly to the hearing aid.
One important consideration when using wireless accessories is that the fitting should be considered open regardless of how the impaired ear is fit. This is because the good ear is not occluded. The time of arrival of the streamed wireless signal to the impaired ear should not be delayed too much relative to the good ear receiving the signal acoustically to avoid disturbing perceptual effects. It has been demonstrated that speech intelligibility benefits will be affected if the transmission delay is greater than 40 ms and the coupling is vented.15 Considering this, the proprietary 2.4 GHz digital wireless technology used by ReSound is advantageous for UHL since the delay associated with streaming is short and there is no relay device needed.16
Noise reduction and frequency lowering algorithms. For noise reduction, the same guidance applies as for binaural fittings. Noise reduction has not been found to improve or degrade speech understanding in adults or school-aged children, but it can improve comfort and ease-of-listening in realistic listening situations. For younger children, further research is needed and it is therefore not generally recommended.14

Figure 2. Binaural correction using NAL-NL2 fitting rule. The dashed lines show the gain targets without the binaural correction; the red lines show the gain settings with the binaural correction; gains are decreased to compensate for binaural summation. (click to enlarge image)
Frequency lowering (frequency compression, frequency translation, or frequency transposition) algorithms are another common feature in hearing aids today. Any type of frequency lowering will cause some amount of sound distortion. Since the good ear will receive undistorted normal sound, the frequency lowered sound may interfere with binaural processing. Therefore, frequency lowering is not suitable for UHL fittings.
Minimizing distortion. For patients with UHL, the good ear serves as the reference for the sound, so it is important to keep distortion at a minimum. Compression output limiting provides superior sound quality as compared to hearing aids that limit maximum output through peak clipping.17 It is better that a hearing aid with compression output limiting is selected in order to get better sound quality to match the good ear.
Verification
No matter which prescription method is used, the target is only a starting point. The good ear will always do most of the work. The role of aided ear is to provide more useful information to help understand speech and for binaural processing. When the poor ear has a severe hearing loss, the aided sound can reach the brain, but it may not be helpful. A fitting with less gain than prescribed can be appropriate in such cases.11
Conclusion
UHL is common, and without intervention it can lead to academic, speech-language, and social-emotional difficulties. But there is only limited literature about hearing aid fitting for patients with UHL; some of the ideas have to borrow from asymmetry hearing loss fitting. Further research is needed in this area.
A hearing aid may be a good option for some of the patients with UHL. Fitting of a hearing aid should be individually based and using your own expertise, taking consideration of patient age, degree of hearing loss, speech development, communication needs, and other morbidities, etc. The relevance of other treatment options than conventional hearing aids, such as FM, CROS, BAHA, and a cochlear implant, also should be considered and communicated to the patient.
Correspondene can be addressed to Dr Cui at: [email protected]
References
1. Kochkin S. MarkeTrak VIII: 25-year trends in the hearing health market. Hearing Review. 2009; 16(11):12-31.
2. Ross DS. Mild and unilateral hearing loss in children. Access Audiology. 2006;5(2)1-8.
3. Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences. Arch Intern Med. 2008; 168(14):1522-1530.
4. Tharpe AM. Unilateral and mild bilateral hearing loss in children: past and current perspectives. Trends Amplif. 2008;12(1):7-15.
5. Lieu JEC, Tye-Murray N. Karzon RK, Piccirillo JF. Unilateral hearing loss is associated with worse speech-language scores in children: a case-control study. Pediatrics. 2010;125(6):e1348-e1355.
6. Bess FH, Tharpe AM. Case history data on unilaterally hearing impaired children. Ear Hear. 1986;7:14-19.
7. McKay S, Gravel JS, Tharpe AM. Amplification considerations for children with minimal or mild bilateral hearing loss and unilateral hearing loss. Trends Amplif. 2008;12(1):43-54.
8. Lieu JEC, Tye-Murray N, Fu Q. Longitudinal study of children with unilateral hearing loss. Laryngoscope. 2012;122:2088-2095.
9. McKay S. Issues related to amplification for children with mild or unilateral hearing loss. National Workshop on Mild and Unilateral Hearing Loss: Workshop Proceedings. Breckenridge, Colo: Centers for Disease Control and Prevention; 2005.
10. Johnstone PM, Nabelek AK, Robertson VS. Sound localization acuity in children with unilateral hearing loss who wear a hearing aid in the impaired ear. J Am Acad Audiol. 2010;21:522-534.
11. Schum DJ. Asymmetrical sensorineural hearing loss: Fitting strategies. AudiologyOnline. Available at: http://www.audiologyonline.com/articles/asymmetrical-sensorineural-hearing-loss-fitting-12222
12. McSpaden JB, Brethower L. Achieving binaural fusion in asymmetric hearing losses. Hearing Review. 2007;14(5)[May]:40-41. Available at: https://hearingreview.com/2007/05/achieving-binaural-fusion-in-asymmetric-losses
13. McCreery RW, Venediktov RA, Jaumeiko JC, Leech HM. An evidence-based systematic review of amplitude compression in hearing aids for school-age children with hearing loss. Am J Audiol. 2012; 21:269–294.
14. McCreery RW, Venediktov RA, Jaumeiko JC, Leech HM. Am J Audiol. 2012;21:269-294. An evidence-based systematic review of directional microphones and digital noise reduction hearing aids in school-age children with hearing loss. Am J Audiol. 2012;21(2)[Dec]:295-312.
15. Whitmer WM, Brennan-Jones CG, Akeroyd MA. The speech intelligibility benefit of a unilateral wireless system. Int J Audiol. 2011;20:905–911.
16. Groth J, Anthonsen F. Fewer wires, less complexity, and more connections: The new challenge for wireless hearing instruments. Hearing Review. 2010;17(6):28-36.
17. American Academy of Audiology. American Academy of Audiology Clinical Practice Guidelines: Pediatric Amplification. June 2013. Available at: http://audiology.org/resources/documentlibrary/Documents/PediatricAmplificationGuidelines.pdf
Original citation for this article: Cui T. Monaural hearing aid fitting considerations for Patients with unilateral hearing loss: Who should receive unilateral fittings, and how should you fit them? Hearing Review. 2014;21(7):32-34.


