Under the care of private practice audiologists (PPAs), many people regain clarity and connection with the help of hearing aids. That is, until the day comes that hearing aids no longer provide sufficient benefit, leaving patients and their providers at a crossroads. Unfortunately, that crossroads may mean that a patient goes too long without optimal hearing, beginning a path toward silence and social isolation. Our industry is changing, and private practice must evolve as well to continue providing patients with the best possible care. Shifting your approach to incorporate hearing implant technology can benefit both your patients and your practice.
EAS is a potential solution that can help your unhappy or underperforming patient take the next step to better hearing. Combining acoustic amplification in the low frequencies with electric stimulation in the high frequencies, as EAS does, results in significant improvement for hearing in background noise. In a recent EAS clinical trial, 97% of participants experienced benefit with EAS, compared to pre-operative performance with hearing aids.
What do you do when your patient can no longer function on the telephone with “best fit” hearing instruments? What can you do when you notice that your “borderline” poor-performing patient is not keeping annual appointments? What is the best course of action when your patient’s word recognition begins falling below 60% in a best aided condition? What is your response when your patient starts asking you about other solutions, like cochlear implants? Or, when you learn that a nearby colleague is offering cochlear implant-related services?
Patients who are experiencing a decline, not just in hearing thresholds, but also in speech understanding, can take advantage of implantable technology when they reach the limit of what hearing aids can provide. MED-EL’s SYNCHRONY EAS (Electric-Acoustic Stimulation) Hearing Implant System was recently FDA approved and combines the electric stimulation of a cochlear implant with the acoustic amplification of a hearing aid. When patients are no longer able to perceive the benefit hearing aids provide in difficult listening situations, like background noise or large rooms, it may be time to consider electric-acoustic stimulation.

MED-EL’s SYNCHRONY EAS (Electric-Acoustic Stimulation) Hearing Implant System.
A patient who fits EAS candidacy criteria may be an ideal start for a PPA to successfully integrate cochlear implant referrals into their practice. Audiologists who have extensive experience with hearing aids already know and advocate for the benefits of acoustic amplification. Combining acoustic amplification with electric stimulation is a clear next step for a patient with low-frequency residual hearing and severe to profound high-frequency hearing loss who is struggling with their current technology. These are patients who are reliant on their residual hearing and fear losing what is familiar to them; however, the audiologist may have exhausted options like frequency-lowering technology and find that the patient is still experiencing significant difficulty understanding. Patients with this type of hearing loss often are looking for another solution but will need the guidance of someone they trust to fully understand the potential risks and benefits, as well as to reach their maximum potential performance after surgery.
EAS: Test Driving the Latest Innovation in Electrical-Acoustic Stimulation Implants
One of the biggest complaints audiologists receive is that hearing in background noise is difficult. Recent improvements in hearing aid technology have enhanced listening in difficult conditions, but the acoustic amplification provided via hearing aids is sometimes not enough. Patients in this predicament begin considering an implant as the next step in their hearing care, but typically want to stay with their longterm audiologist, if possible. Working with EAS can allow patients to continue care in the same setting, and also allow them to experience electrical-acoustic stimulation. EAS candidates are not the same as traditional cochlear implant candidates with profound hearing loss in both ears and, thus, can especially benefit from a continued relationship with an audiologist who is already familiar with their hearing needs and concerns.
EAS is a potential solution that can help your unhappy or underperforming patient take the next step to better hearing. Combining acoustic amplification in the low frequencies with electric stimulation in the high frequencies, as EAS does, results in significant improvement for hearing in background noise.
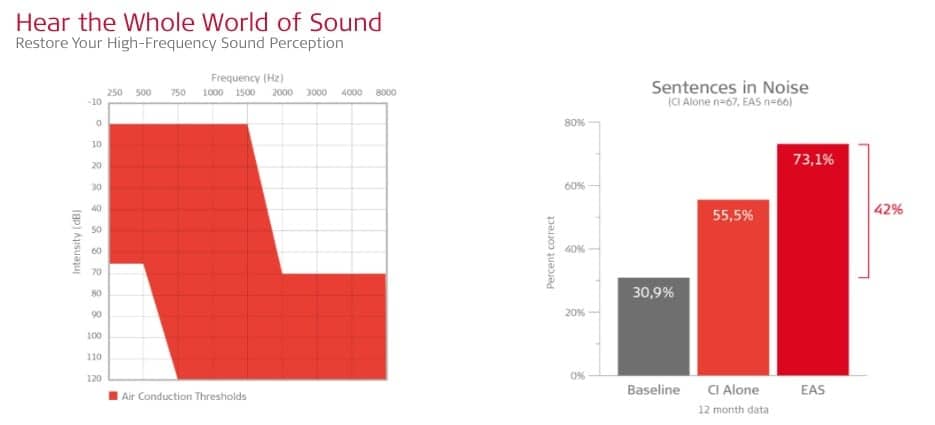
Figure 1. The graph at right shows the results of post-operative sentence testing in background noise, one of the most difficult environments for people with this type of hearing loss. EAS users score an average of 42% higher in speech understanding. In addition, 90% of EAS recipients report increased satisfaction with EAS compared to their hearing aids.
Although the loss of residual low-frequency hearing is an important consideration for patients with partial deafness, a recently-completed clinical trial demonstrated that 97% of EAS patients could still access the acoustic amplification feature of the processor. In fact, 92% of patients reported improved hearing in background noise after receiving EAS, compared with hearing aids before surgery.1 Given the impressive results that patients receive from EAS, a discussion about the risks and benefits of this implantable technology could be the first step to improved outcomes. In the EAS clinical trial, 97% of participants experienced benefit with EAS, compared to pre-operative performance with hearing aids.
Additionally, the benefits of binaural hearing are widely recognized. Many patients may be longterm clients of private practices and may come into the office wearing two hearing aids that are not providing sufficient benefit. When that time comes, careful consideration should be given to continued bimodal hearing. Patients may elect to only have one ear implanted at a time, and will likely benefit from continued use of hearing aid technology in the non-implanted ear. The current audiologist can continue to provide hearing care and ensure that patients are also aware of newer hearing aids and accessories that aim to improve the patient’s lifestyle. An EAS patient is likely to continue wearing a traditional hearing aid on the contralateral ear, so providing the comprehensive service for this patient – EAS and hearing aid in one appointment – can allow for continued care and can set the practice apart. Although many patients may have hearing loss that requires implantable technology in order to reach their best performance, these patients will still require the same consistent counseling and careful device fitting that has always been provided in order to maximize their performance.
Overcoming Potential Pitfalls as You Shift Your Practice to Include Implant Services
While audiologists want to provide the best services for their patients, the path toward becoming a full-service private practice audiologist (PPA) may have some perceived obstacles. Audiologists want to remain a part of the journey with their patients in reconnecting with the world around them. Patients who are frustrated with their hearing aids may eventually seek other options for hearing devices – which could include moving to larger cochlear implant centers. However, cochlear implant awareness in the general population remains low, so these patients may also become non-users and may stop returning to their audiologists for regular follow-ups. This possibility is unfortunate for the patient and the audiologist, both of whom would likely rather continue to build a relationship with someone they have already grown to trust.
Perhaps one of the biggest barriers that PPA owners face is trust that a patient referred to an implant surgeon for a cochlear implant or EAS will not become lost to the CI center. While the reality is this can happen, trust between your practice and the implant center can be developed. When exploring and establishing referral options in the area, have a discussion with the cochlear implant center surgeons and audiologists directly to determine if they are willing to send a referred patient back for mapping and follow-up care. Be prepared for cases where the implant center may say they need to follow the patient once they are implanted and consider that scenario. Open communication between the surgeon and referring audiologist can help ensure that staff at the implant center handles the patient appropriately and agrees to work together to follow the patient.
Reimbursement for services and goods is another critical consideration for a private practice audiologist interested in making the jump to becoming a full-service center. Options exist to support PPAs in obtaining reimbursement for services and goods related to implantable hearing technology. While durable medical goods, such as external components of a cochlear implant processor, are sometimes reimbursed for less than cost, PPAs can consider billing directly to insurance only for services, limiting the financial risk. The parts and accessories can then be submitted to insurance companies by the patient directly or the manufacturer. The idea of submitting for reimbursement for services is consistent with the medical model many PPAs have adopted that ensures hearing tests, other diagnostics, and services associated with hearing devices have a value. While reimbursement can be time-consuming for a PPA with limited administrative resources, manufacturers often have staff available to assist with this process.
Hearing Implants – Referral and Mapping
Once a PPA has decided to make the leap and incorporate implantable hearing technology into their practice, taking the time to invest in learning about cochlear implants and mapping is a critical step that can be accomplished through continuing education and working directly with manufacturers. After that level of expertise is achieved, where do the candidates come from and how can they be followed?
In some cases, an existing CI user may move to the area and need a local point of care. Providing this service is an easy way of seeing CI patients and testing the waters in terms of feasibility for expanding to a referral model. Initially, the numbers of these patients will be low, giving the PPA and staff opportunities to learn common pitfalls regarding reimbursement, scheduling, and referrals.
In terms of new EAS or CI candidates, the key can be as simple as asking surgeons how you can work together. If you have patients who don’t meet hearing implant criteria, but might be close, those patients can open the lines of communication. An EAS candidate, in particular, can open the door to discussions with local surgeons and audiologists about the center’s protocol for seeing new patients and determining implant candidacy. You can also have a discussion with the surgeons and audiologists about how the center would like to receive their referrals. Ideally, at that point, a discussion can begin with the center’s audiologists regarding follow-up care and ordering. As with any newly implemented process, there can be questions and misunderstandings along the way, and it’s important to address these with those involved.
It is important that patients are aware they have a choice in follow-up care. By ensuring patients understand that they have a choice, you may even encourage them to explore implantable options that they would have shied away from under the assumption that they would have to start over with new healthcare providers. Patients like what is familiar, and that familiarity, convenience and existing relationship can bring a patient back to your practice – especially if they know that the choice is theirs.
Integrating Comprehensive Hearing Solutions into Your Practice
An implant like EAS can help people with severe hearing loss get comfortable with the concept that their hearing health technology does not need to end with a hearing aid. Specifically, you can suggest moving forward with EAS testing, discuss options with your patient, and then refer if warranted. You can send over results, and possibly even offer to call the surgical CI center to make the appointment for the patient, so that the CI Center office knows the patient has had testing and are referred from your office. These actions can provide a service, as patients are not always able to provide all the relevant information. Consider sending the patient with the CI or EAS testing already completed, as this can keep your practice involved with the patient’s continuum of care.
Providing hearing solutions that increase satisfaction with hearing in background noise and other difficult listening situations not only results in an increased number of happy patients, but can also potentially lead to additional referrals and less time spent reprogramming patients with the same complaints. Manufacturers are a good resource for materials for your office, including candidacy, literature for patients and family members, support groups for CI candidates and recipients, and patient support post implantation.
More than ever before, technology and the latest innovations can help people overcome hearing loss as a barrier to communication. Now may be the time to embrace these changes and expand your services. Ultimately, providing the best and most appropriate care for each and every patient is what works; finding the right technology for the right patient can make a remarkable difference in connecting to the world of sound. The silver lining is that this can also pay dividends in expanded markets for PPAs willing to take their practice to the next level.
Reference
1. IDE G040002 Final Report “Electric-Acoustic Systems Clinical Trial.” The Electric Acoustic Stimulation (EAS) System clinical trial was a multi-center, FDA-controlled study in the US, including the Department of Otolaryngology/Head and Neck Surgery, University of North Carolina School of Medicine, which implanted more patients than other centers. Allison Racey, AuD, MED-EL, had oversight of the EAS System clinical trial overall, while audiologists Margaret Dillon, AuD, Assistant Professor, Director, Cochlear Implant Clinical Research; and Meredith Anderson, AuD, Research Instructor, were co-investigators of the clinical trial at UNC. The EAS System was FDA-approved in September 2016 for candidates age 18 years and older who have normal to moderate sensorineural hearing loss in the low frequencies, sloping to a severe-to-profound hearing loss in the high frequencies (with single-word speech understanding scores at less than 60% in both ears pre-operatively).

Allison Racey, AuD
Allison Racey, AuD, is Manager of Clinical Research, MED-EL, where she oversaw the EAS clinical trial in the United States.

Melissa Riess, AuD
Melissa Riess, AuD, is the founder of Hearing Associates of Central Florida. She has expertise in the fitting of digital hearing aids, FM devices and cochlear implants.