
Recently, the concept of a “trainable” or “self-adjustable” hearing aid was introduced.1 In brief, the trainable hearing aid presents the user with a set of control buttons that are used to manually adjust selected hearing aid parameters to reach the user’s preferred gain and frequency response. Using the control buttons, the user can adjust the device to his or her own listening preferences outside the clinic in a variety of everyday acoustic environments.
During this process, the hearing aid identifies the acoustic characteristics of the environment and combines this data with manually input information about the user’s preferred gain and frequency response. When sufficient data have been accumulated, the hearing aid begins to make predictions about the user’s preferences in different listening situations based on the environment’s acoustic characteristics, and continues to refine these predictions for as long as additional input from the user is received. The device is considered “fully trained” when the hearing aid is able to accurately predict the user’s listening preferences in different acoustic environments and therefore no longer requires manual adjustments on the part of the user.

|
| Gitte Keidser, PhD, is a senior research scientist, Elizabeth Convery, MS, is a research audiologist, and Harvey Dillon, PhD, is the director of the National Acoustic Laboratories (NAL) in Sydney, Australia. |
Benefits of a trainable hearing aid may include fewer visits to the dispensing professional for fine-tuning, the opportunity to adjust the hearing aid in real-life environments that are difficult to replicate in the clinic, and greater psychological “ownership” of the fine-tuning process, all of which may lead to increased aid acceptance and usage.2 Potential disadvantages to a trainable hearing aid are the time required to train the device to an optimal setting and the additional control(s) with which the user needs to become familiar.
At the National Acoustic Laboratories (NAL), a trainable research device has been developed and evaluated. It was found that the individually trained gain-frequency response was significantly preferred to the response that was prescribed by NAL-NL1 (Zakis JA et al, unpublished data, 2006). We emphasize, however, that the success of a trainable device will depend on how efficient the training algorithm is in relating information about the acoustic environment to the preferred amplification characteristics. Although there are indications that giving consumers more control over their devices may improve satisfaction,3 it is currently unknown how this development in hearing aid technology is viewed by the wider clinical population, and whether hearing-impaired individuals are ready to embrace this development.
In the current survey, adult hearing aid candidates attending a variety of audiology clinics were introduced to the concept of a trainable hearing aid with a written description and a hands-on demonstration, giving them access to controls that allowed them to manipulate the gain-frequency response. Questionnaires were then administered to assess:
- The proportion of clients who thought this step in development was positive and hence qualified as potential users of a trainable hearing aid, and
- The perception of the technology.
Methods
Adult hearing aid candidates from five audiology clinics in the metropolitan Sydney area were approached to participate in the survey, which took 15 to 20 minutes to complete. Participants were drawn from two private clinics, one university-based clinic, and two clinics that provide government-funded services to pensioners and veterans. We approached these clinics on the basis of their geographical location and typical clientele, with the goal of including a diverse cross-section of the hearing-impaired population. A total of 100 interviews across all locations was sought. The interviewees were consecutive clients who understood the request to participate in the survey and who volunteered to do so.
The participants’ primary source of information about the concept of trainability was a printed information sheet that outlined the features of the trainable hearing aid and described how it differed from a conventional hearing aid. A hands-on demonstration of how adjustments may be made to the gain-frequency response during the training period was given to each participant. A continuously looped audio file of a female voice in a background of car noise was presented in the free field, using a laptop computer, an NAL-developed software program called RealWave, and two Active 85 loudspeakers. A handheld keypad, with which two parameters (the slope of the frequency response and the overall volume) could be adjusted using two independent sets of two buttons, was provided to the participants. For each parameter, one button was used to increase the parameter and the other button was used to decrease the parameter.
Wearing their own hearing aids, if applicable, the participants were instructed to adjust the settings to their own listening preferences. Participants were allowed to manipulate the buttons on the keypad for as long as they wished. The hands-on demonstration was included in the survey to give the interviewed clients an idea of the types of adjustments that would be possible when training a hearing aid. It did not, however, demonstrate the training procedure (ie, how, after repeated adjustments of the gain-frequency response by the client in various listening environments, the aid would automatically start to adjust itself to the client’s preferred settings).
Two questionnaires were administered. Personal data were collected with the first questionnaire. Participants were asked open-ended and multiple-choice questions about age, gender, level of education, employment status, the length of time they had known about their hearing loss, the length of time they had used amplification, the number of hearing aids typically worn, and the frequency of aid use. Ten-point rating scales were also used to assess hearing aid benefit in quiet and in noise, unaided hearing handicap, residual aided handicap, and attitude toward the use of new technology.
The second questionnaire was an opinion survey about the concept of trainability. All questions were multiple-choice and were designed to assess whether participants liked the trainable aid concept, whether they felt a trainable aid would provide them benefit, how long they would be willing to spend training the device, whether they would prefer to train the hearing aid with a remote control or with an onboard switch or button, the optimal number of switches or buttons on the controller, and whether they would choose a conventional or trainable aid if both options were currently available. Participants were also invited to comment on what they thought would be potential advantages and disadvantages of the trainable aid concept.
|
Parameter |
Median [range] |
|
Gender (1 = male, 2 = female) |
1 [1,2] |
|
Years of age |
77 [23,95] |
|
Education (1 = up to year 10, 2 = high school, 3 = technical college, 4 = university) |
1.5 [1,4] |
|
Employment (1 = student, 2 = apprentice, 3 = unemployed, 4 = employed part-time, 5 = employed full time, 6 = retiree or pensioner) |
6 [3,6] |
|
Years with hearing loss |
15 [0.25, 75] |
|
Number of hearing aids (0 = none, 1 = one, 2 = two) |
2 [0,2] |
|
Years with hearing aids |
7.5 [0.04, 59] |
|
Hours of daily use |
16 [0, 16] |
|
Benefit in quiet (rating from 1 to 10) |
8 [1,10] |
|
Benefit in noise (rating from 1 to 10) |
5 [1,10] |
|
Aided handicap (rating from 1 to 10) |
4 [1,10] |
|
Unaided handicap (rating from 1 to 10) |
8 [1,10] |
|
Attitude toward technology (rating from 1 to 10) |
6 [1,10] |
|
TABLE 1. Median values and range of responses to personal data questionnaire. |
|
Profile of Interviewees
Table 1 shows the median values and range of responses to the personal data questionnaire. It can be seen that the “average” client who agreed to participate in the survey was a retired 77-year-old male who had left the education system before finishing high school. He had known about his hearing loss for the past 15 years, and he had worn amplification bilaterally for 16 hours per day for the past 7.5 years. He obtained more benefit from his hearing aids in quiet than in noise. Overall, his aided handicap was reduced relative to his unaided handicap, and his attitude toward new technology was on the positive side.
Nearly half of the participants had a mild or moderate, gently sloping hearing loss, but a wide variety of hearing loss configurations was represented in the study sample, as shown in Table 2. The degree of loss was calculated by averaging the thresholds at 0.5 kHz, 1 kHz, and 2 kHz (PTA) across both ears. The slope was determined by calculating the difference between the high-frequency loss (average of 2 kHz, 3 kHz, and 4 kHz) and the low-frequency loss (average of 0.25 kHz, 0.5 kHz, and 1 kHz) and averaging the result across both ears. Most participants had a symmetrical sensorineural hearing loss.
|
|
Reverse slope |
Flat |
Gently sloping |
Steeply sloping |
|
Slight and mild |
– |
2 |
21 |
8 |
|
Moderate |
– |
14 |
24 |
1 |
|
Moderately severe |
1 |
9 |
6 |
2 |
|
Severe and profound |
1 |
4 |
5 |
2 |
|
TABLE 2. Distribution of the hearing losses of the interviewed clients by slope and degree of hearing loss. |
||||
Results and Discussion
Potential users. During the time the interviews were conducted, the participation of 247 adult hearing aid candidates who had appointments with the clinic was solicited. Of the 147 clients who were not interviewed, 62 declined participation and 85 were not approached. The reasons for not approaching clients included a known cognitive impairment, known insufficient English skills, incorrect contact details, and contact details withheld by the clinic.
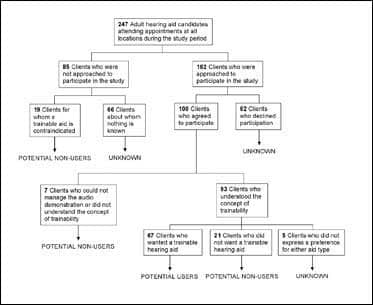
Defining a potential user of a trainable device as a person who appeared to understand the trainable concept and who could manage the audio demonstration, and who expressed a desire to try a trainable aid over conventional amplification, the 100 interviewed and 147 noninterviewed clients were grouped into three categories: potential user, potential nonuser, and unknown. The flow diagram in Figure 1 shows the distribution of interviewed and noninterviewed clients in the three categories. The categorization of interviewed clients was based on their responses to the survey and particularly their responses to the question, “If you could choose between a conventional hearing aid and a trainable hearing aid today, which one would you choose?” Noninterviewed clients who had profound hearing loss and primarily used sign language, as well as those with a known cognitive impairment, were assigned to the potential nonuser category, because both characteristics were assumed to be contraindications to a trainable hearing aid. The remaining noninterviewed clients for whom no data were available to suggest whether or not they were potential users of a trainable aid were categorized as unknown.
|
| FIGURE 1. Flow diagram showing the categorization of adult hearing aid candidates into potential trainable hearing aid users, non-users, and unknown. |
In all, 67 clients were classified as potential users of a trainable hearing aid, 47 as nonusers, and 133 as unknown. Among clients positively identified as either potential users or nonusers (114 in all), 59% were classified as potential users of a trainable hearing aid. The five interviewed clients who had no preference for either style of hearing aid technology had not had experience with hearing aids at the time of the interview, and consequently found it difficult to indicate a preference either way.
The relatively high percentage of potential trainable aid users among only the interviewed clients (67%) reflects a general positive appraisal of the idea of training a hearing aid in diverse listening environments, and many spontaneous comments by clients confirmed this. However, it should be pointed out that the interviewed clients were given relatively little time to consider the implications of and commitment to training a hearing aid, as the participants’ feedback was solicited immediately after their initial introduction to the concept of trainability. It is likely that, if the clients had been allowed more time to think about the potential cost, self-discipline, and time investment required to train a hearing aid, a number of the interviewed clients may have selected a different option. Consequently, the percentage of potential trainable aid users identified here should be interpreted with some caution, and may be considered more an upper limit, rather than an absolute value.
A further explanation for the positive response to the trainable aid concept, which led to the identification of a relatively high proportion of potential trainable aid users, may be traced to the motivation of the interviewed clients. It is generally believed that motivation has a strong influence on whether or not an individual decides to try a hearing aid.4,5 One can argue that, since the sample used in this study was drawn from a population of hearing-impaired individuals who had already entered the hearing health care system, the sample is mostly reflective of highly motivated hearing aid candidates.
It is also possible that the audio demonstration may have affected the participants’ opinions about trainability. For the audio track that was used in the demonstration (speech in car noise), it was possible for most clients to find a gain-frequency response that reduced the background noise while maintaining clarity of the speech, thus providing the client with a positive experience. Although all participants were told that the demonstration was not tuned to their individual hearing loss, it was apparent that some participants based their opinions of the trainable aid on their success in finding a setting that was suitable for them. There is no way of knowing to what extent the demonstration influenced the participants’ opinions about trainability and hence, their response to the question that led to the classification of participants as potential users or nonusers of a trainable aid. We hope, of course, that the audio experience was evaluated together with the written introduction to the trainable aid concept and the following discussion with the experimenter about the concept.
|
Parameter |
ß |
p-level |
Tolerance |
|
Attitude to technology |
-0.47 |
0.008 |
0.90 |
|
Education |
-0.21 |
0.25 |
0.87 |
|
Gender |
0.27 |
0.14 |
0.85 |
|
Symmetry |
-0.67 |
0.0006 |
0.72 |
|
PTA |
0.50 |
0.01 |
0.71 |
|
Age |
0.48 |
0.01 |
0.78 |
|
Aided Handicap |
-0.29 |
0.11 |
0.88 |
|
Slope |
-0.26 |
0.20 |
0.73 |
|
TABLE 3. The eight parameters that correctly predicted potential trainable aid usage in 82% of participants. ß (standardized weight): the relative independent contribution of the parameter; p-level: significance level; and tolerance: the proportion of variance that is unique to the respective parameter with all other variables included in the model. The higher the tolerance value, the less redundant the parameter. |
|||
Profile of potential trainable aid users. A profile of a potential trainable aid user was sought among the personal and audiometric parameters collected for the interviewed clients, of whom 67 were classified as users and 28 as nonusers. A discriminant analysis produced a significant model (p < 0.00001) that included eight parameters, suggesting that a potential user of a trainable hearing aid tends to be a younger, better educated male with milder, more sloping, less symmetrical hearing loss; a high degree of self-perceived aided handicap; and a positive attitude regarding technology. The model correctly classified 61 of the 67 potential users for the trainable hearing aid and 17 of the 28 potential non-users, or 82% of all participants. According to the standardized regression coefficients (ß), the significance level (p), and the tolerance value (1 – R2), symmetry of hearing loss, PTA, age, and attitude toward technology contributed to the greatest degree (Table 3). A discriminant analysis including only these four parameters as independent variables produced a significant model comprising all four parameters that correctly identified 79% of participants (ie, almost the same number of participants as the eight-parameter model). The four-parameter model is considered more valid and less likely to be a chance result than the eight-parameter model.
Whereas age would seem to be a likely predictor, potential users of a trainable aid were not exclusively young; the mean age of the candidates was 71 years, as compared to 78.5 years for potential nonusers. Level of education also appears to be a sensible predictor, if it is assumed that individuals with higher levels of education naturally constitute a more curious and experimenting population. Given that a majority of the interviewed clients were above 60 years of age, it is also believable that gender and attitude toward new technology contributed significantly to the discrimination between potential users and nonusers. Our prediction is, however, that such parameters will cease to be significant in the future, as increasing numbers of females with careers enter the aging population and technology becomes more common in the lives of the elderly.
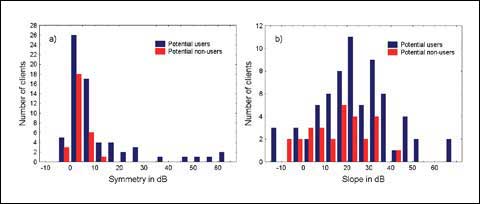
The two audiometric predictors of users of a trainable aid should be interpreted with care. Participants with highly asymmetrical hearing loss (difference in PTA of 30 dB or more between ears) or who had a steeply sloping high-frequency hearing loss (slope > 40 dB) made up small subgroups of our study sample (six and nine participants, respectively). All but one participant in the two subgroups fell into the potential user category, which caused the “symmetry” and “slope” parameters to show statistical significance.
However, if we look at the group of potential users of a trainable aid as a whole, we see that there are actually more participants with symmetrical hearing loss (difference in PTA of 20 dB or less between ears) and flat hearing loss (slope < 20 dB) who identified as potential users of a trainable aid (56 and 27, respectively) than there were participants with asymmetrical hearing loss and steeply sloping loss (Figure 2). So although the data suggest that clients with asymmetrical hearing loss or steeply sloping high-frequency hearing loss are very likely to be potential trainable hearing aid users, there is certainly no reason to believe that clients with symmetrical hearing loss or a flatter audiometric configuration could not benefit from such a device. Finally, we would like to point out that a different model may have emerged if the personal and audiometric data from the 19 noninterviewed nonusers had been included.
|
| FIGURE 2. Distribution of interviewed potential users and nonusers of a trainable hearing aid across a) symmetry of hearing loss, and b) slope of hearing loss. The larger the audiometric parameter, the less symmetrical and more sloping the hearing loss. |
Perception of trainability. Of the 100 interviewed clients, 93 completed the trainable aid opinion survey, because the interview had been discontinued at this point for seven participants who did not demonstrate a reasonable understanding of the trainable aid concept, or who could not manage the hands-on demonstration.
The pie charts in Figure 3 show the distribution of these participants’ responses to the survey questions. First, it can be seen that an overwhelming proportion of the interviewed clients who completed the questionnaire (91%) reported that they liked the idea of a trainable hearing aid (Figure 3a). However, when asked subsequently about the degree of personal benefit the participant would expect to receive from trainability, the percentage of interviewed clients who responded positively dropped to 66% (Figure 3b). So, not all participants expected the invention to provide a better solution to their hearing problems.
Second, with respect to training the device, three-quarters of participants (76%) reported that a few weeks or less would be a reasonable time commitment (Figure 3c). The preference for control of alterations to the amplification characteristics was almost equally distributed: 54% of participants expressed a preference for using a remote control, while 46% preferred the option of buttons or switches on the hearing aid itself (Figure 3d). An overwhelming 90% felt that a trainable hearing aid should have two controls, as introduced in the hands-on demonstration, while 9% preferred a greater number of controls (Figure 3e). This information suggests that the design has to be simple and that training must be completed relatively quickly.

|
| FIGURE 3. Response distributions for seven opinion survey questions, which were designed to assess: a) whether participants liked the trainable aid concept; b) whether participants felt a trainable aid would benefit them; c) how long participants would be willing to spend training the device; d) whether participants would prefer to train the hearing aid with a remote control or with an onboard switch or button, and e) the preferred optimal number of controls. |
The trainable aid opinion survey concluded with two open-ended questions that targeted potential advantages and disadvantages of the trainable concept. Participants cited as advantages the ease of adjusting their own hearing aid settings rather than attempting to explain their preferences to an audiologist, the ability to tailor the hearing aids to their own listening situations without repeated visits to an audiology clinic, and the flexibility of being able to control the quality of the tone. Disadvantages reported included the potential high cost of the device, the possibility of an increase in size and/or weight of the hearing aid, and the concern that many users would not have sufficient knowledge to optimize their own settings without the guidance of an audiologist.
From the responses to the survey, it is apparent that—although many clients liked the idea of training their own devices and praised the expected advantages—the clients opted for less flexibility (few controls) and a short training period. Whereas Dreschler et al (unpublished data, 2006) found some indication that more parameters—and hence greater flexibility in terms of adjusting the gain-frequency response—do not necessarily lead to a different or better outcome than a two-parameter approach, there are data suggesting that longer training periods will lead to a more satisfactory outcome (Zakis JA et al, unpublished data, 2006). However, the time it would take the trained response to converge to the preferred response would depend on the specific algorithm used to train the device (Zakis JA, unpublished data, 2005).
From the results of the opinion questionnaire, it would also appear that, to make the trainable hearing aid accessible to as many clients as possible, a choice between a remote control and onboard switches or buttons must be available, because clients reported strong preferences for the option they selected during the interview.
Conclusion
A survey of a typical clinical population revealed that 59% of adult hearing aid users are interested in training their own hearing aids. Four parameters in particular, when combined, were found to discriminate between those who were interested in a trainable aid and those who were not. Among clients who participated in the survey, the parameters correctly identified 79% of the interviewees (at a higher than chance level). According to this model, those who were interested in a trainable aid are younger, show a strong interest in technology, and have a milder and less symmetrical hearing loss.
The model requires further verification and should not be interpreted as excluding clients with other audiometric profiles, or implying automatic candidacy for those with the right profile. For a large uptake of the trainable hearing aid, it would seem that the device must be fully trained within a few weeks using a few simple controls. Clients should be provided with a choice of method for accessing the user controls.

|
| “Twenty Trends Influencing the Hearing Care Field.” December 2005 HR. |
Acknowledgments
This study was supported by the Co-operative Research Centre for Cochlear Implant and Hearing Aid Innovation of Australia. A preliminary version of this paper was presented at the American Academy of Audiology Convention in Washington, DC, in March 2005.
The authors thank the managers of the five Sydney audiology clinics who allowed us access to their clients and facilities: Allen-Fisher Acoustics, AudioClinic Chatswood, Macquarie University Audiology Clinic, and the Sydney and Parramatta branches of Australian Hearing. We are especially grateful to the clients of these clinics who generously gave of their time to participate in this study. In addition, we would like to thank Dan Zhou and Scott Brewer of NAL for coding the audio demonstration software that was used in this study.
References
- Dillon H, Zakis J, McDermott H, Keidser G, Dreschler W, Convery E. The trainable hearing aid: What will it do for clients and clinicians? Hear Jour. 2006;59(4):30-36.
- Zakis JA. A Trainable Hearing Aid [PhD dissertation]. Melbourne, Australia: University of Melbourne; 2003.
- Kochkin S. MarkeTrak IV: Isolating the impact of the volume control on customer satisfaction. Hearing Review. 2003;10(1):26-35.
- Hickson L, Hamilton L, Orange SP. Factors associated with hearing aid use. Austr J Audiol. 1986;8(2):37-41.
- Gatehouse S. Glasgow Hearing Aid Benefit Profile: derivation and validation of a client-centered outcome measure for hearing aid services. J Amer Acad Audiol. 1999;10(2):80-103.
Correspondence can be addressed to HR or Gitte Keidser, National Acoustic Laboratories, 126 Greville St, Chatswood, NSW 2067, Australia; e-mail: .



