SPECIAL ISSUE: Unilateral Hearing Loss | Tech Topic | Implants & Bone-anchored Solutions
CROS and BiCROS hearing aids are not the only treatment options for those with unilateral hearing loss. This article reviews other options and potential future avenues for unilateral sensorineural hearing loss and single-sided deafness, as well as for unilateral conductive hearing loss.
Unilateral hearing loss (UHL) is an overly simple description of a broad range of hearing loss configurations, etiologies, sites of lesion, duration, onset, and severity. It is likely that all audiologists have patients with UHL in their caseload, regardless of their work setting. As discussed in this special issue, people with UHL are a group that is generally underserved, and patients with UHL have historically had limited options. Frequently, they often simply choose to “just get by”—that is, they go untreated.1
This article discusses currently available options beyond hearing aid-based contralateral routing of signal (CROS) systems and assistive devices for use in the audiologic management of sensorineural and conductive UHL. Overall, there is low usage of hearing technologies among people with UHL for a variety of reasons. Having a better appreciation for the impact of UHL and the broad range of available options will allow clinicians to better assist patients with personalized and informed decision-making regarding the latest treatments and technologies.
Unilateral Sensorineural Hearing Loss and Single-Sided Deafness
Unilateral profound sensorineural hearing loss (SNHL), also known as single-sided deafness (SSD), is generally characterized as a profound SNHL in one ear, with normal hearing thresholds in the opposite ear. Patients who are diagnosed with unilateral profound SNHL often experience a reduced quality of life, as well as a reduction in speech perception abilities and a reduction in the ability to tell from where sounds originate.2
Existing treatment options for SSD include CROS or BiCROS hearing aids and bone conduction devices (aka bone conduction hearing systems, BCHS). These treatment options work by transferring the signal from the worse hearing side to the better hearing side, and thus do not provide hearing sensation to the worse ear. Although traditional CROS and BiCROS may provide benefit in certain listening situations, such as when the person speaking is near the microphone, they may also provide a detriment to hearing abilities in other listening situations, such as when the person speaking is on the better hearing side, and noise originates on the microphone side.3
Surgical bone conduction devices may result in higher user satisfaction than CROS hearing aids, yet they too, may demonstrate these same “head shadow” detriments, when noise is present on the side with the microphone/transmitter (ie, the side of the profound SNHL ear).4
Currently, surgical and non-surgical bone conduction options are available to treat SSD. These include:
- The ADHEAR and BONEBRIDGE systems from MED-EL;
- Baha from Cochlear Corp, and
- Ponto from Oticon Medical.
While devices intended to transfer sound to the better hearing ear can improve speech perception and provide awareness of sounds on the deaf side, they do not restore binaural hearing.
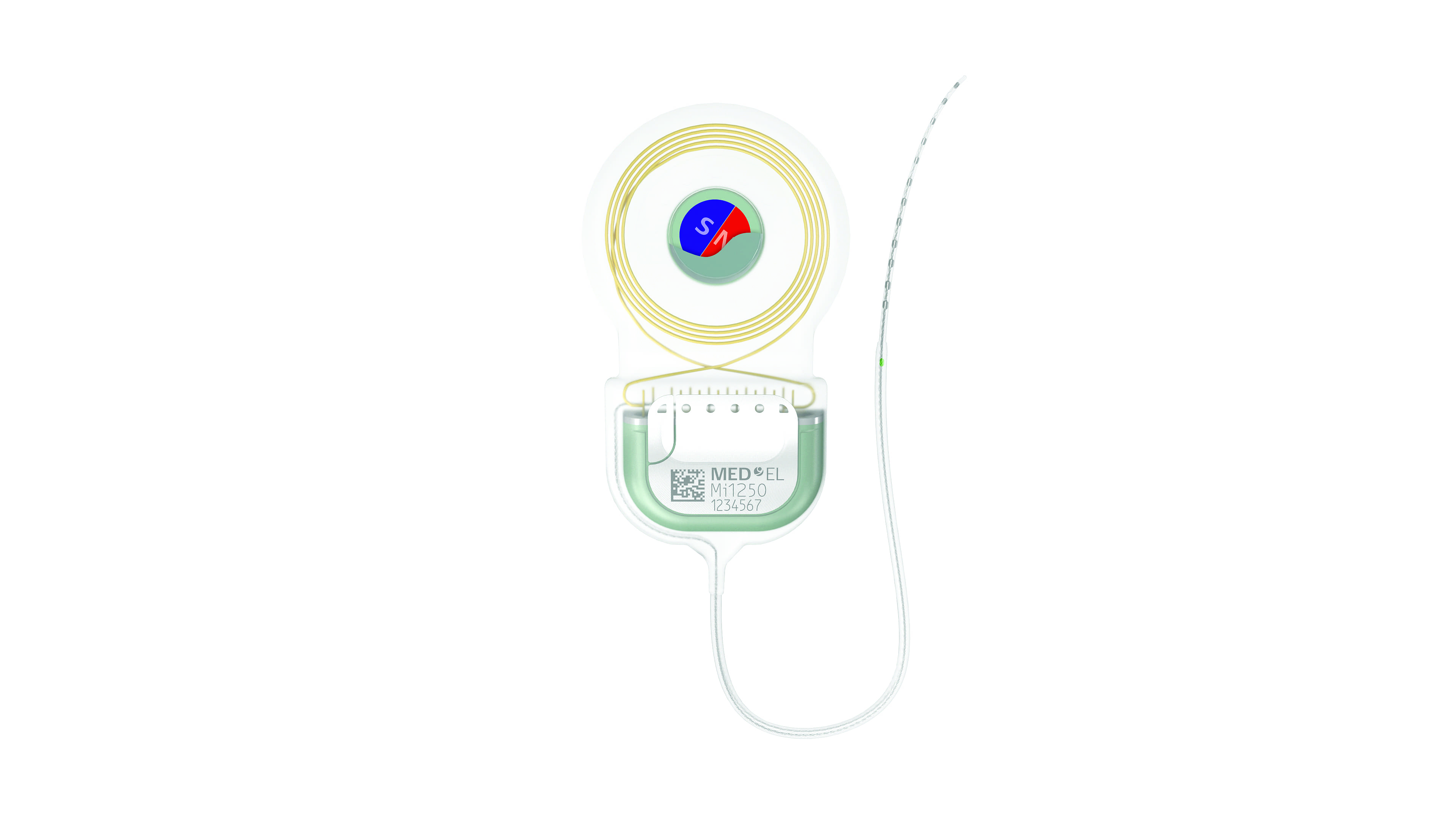
Figure 1. This year, MED-EL Cochlear Implant (CI) Systems, including Synchrony and the recently FDA-approved Synchrony 2 (pictured above), are now indicated for individuals aged 5 years and older with SSD who have profound SNHL in one ear and normal hearing or mild SNHL in the other ear, or individuals aged 5 years and older with AHL who have profound SNHL in one ear and mild to moderately severe SNHL in the other ear, with a difference of at least 15 dB in pure-tone averages between ears.
Although cochlear implants (CIs) have been used to treat bilateral severe-to-profound hearing loss for more than 50 years, CIs for SSD is a relatively new CI application. Specifically, CI research for SSD patients who sought cochlear implantation as a treatment for incapacitating tinnitus5 has been ongoing for more than 10 years. Due to patient reports of multiple benefits after implantation, the impact of CI on speech perception, localization, and quality of life has been re-evaluated and studied extensively in the SSD population. Early reports demonstrated that cochlear implantation for unilateral sensorineural hearing loss can restore some binaural benefits for speech perception and localization.6
In 2019, MED-EL became the first cochlear implant manufacturer to obtain FDA approval for cochlear implantation in SSD patients and for patients with asymmetric SNHL (also abbreviated AHL) ages 5 years and older. Data from the University of North Carolina at Chapel Hill, along with the published body of literature, has demonstrated that cochlear implantation for appropriate patients with SSD is effective in the restoration of binaural hearing.
UNC Chapel Hill completed a clinical trial examining the results of cochlear implantation on 20 subjects with SSD. All subjects were implanted with a MED-EL cochlear implant with a standard electrode array. The study sought to determine the effect of CI on speech perception ability, as well as localization and quality of life. The investigators found that word recognition ability with the cochlear implant alone improved significantly compared to pre-operative measures and that these results were similar to those obtained by traditional cochlear implant recipients.7 The cochlear implant also provided benefits in speech perception in noise when a masker was presented either to the front or to the better hearing ear. When the masker was presented to the worse ear, no detriment in speech perception was detected. Localization skills were also improved post-implantation. Subjective benefit of the device on quality of life (QOL) was also measured in this clinical trial via the Abbreviated Profile of Hearing Aid Benefit (APHAB) and the Speech, Spatial, and Qualities (SSQ) of Hearing Scale.2 Cochlear implant recipients with SSD demonstrated improvements in QOL as early as one month after device activation. These outcome measures revealed patients perceived a benefit from the cochlear implant on speech perception in noise, spatial hearing, and listening effort. As such, cochlear implantation with MED-EL Systems is now an FDA approved treatment for SSD.
The results from the clinical trial conducted at UNC have been corroborated by a large body of published literature from around the world. A study from the House Clinic in Los Angeles demonstrated similar benefits in speech perception and localization on 10 subjects who were also implanted with a MED-EL cochlear implant.8 Further, the subjects in the House study indicated significant improvements in QOL 6 months after device activation.
A small number of studies have been completed that include children with SSD or asymmetric hearing loss. Two studies published in recent years indicated that children may also obtained benefit from cochlear implantation in the presence of unilateral profound SNHL.9,10
Together, this data demonstrates that cochlear implantation can provide better spatial awareness and improved speech perception for patients with SSD. Cochlear implantation can also enhance QOL for many of these same people. The risks of cochlear implantation for SSD are the same as the risks for CI in the traditional population, and the potential benefits a person may obtain from CI generally outweigh the risks.
Unilateral Conductive Hearing Loss
Conductive hearing loss (CHL) may result from a variety of issues, including: otitis media with effusion, impacted cerumen, cholesteatoma, multiple ossicular issues, tympanic membrane perforations, congenital aural atresia, otosclerosis, trauma to the temporal bone, and more. Patients with unilateral conductive hearing loss may be candidates for bone conduction devices, and the audiologist and otolaryngologist generally work collaboratively to diagnose the patient and to determine their specific treatment options.
de Wolf and colleagues11 demonstrated that when an air-bone gap greater than 30-35 dB is present, patients generally perform better with a bone conduction system than a traditional air conduction hearing aid. Of note, in cases where there is an actively draining ear, or the patient is susceptible to otitis externa, or in the presence of aural atresia, a bone conduction system is most often the preferred and chosen option.11,12
Aural atresia, a congenital condition that is most often unilateral, is characterized by an absent or stenotic external auditory canal. Aural atresia is typically accompanied by microtia (ie, underdeveloped pinna), may involve the middle ear and ossicles, and may occur in association with other craniofacial conditions and syndromes. Estimates of incidence range from about 1 in 10,000 to 20,000 live births.13,14 Aural atresia occurs more commonly in boys and is more often right-sided than left-sided. Children with unilateral aural atresia tend to present with a moderate or moderate-severe conductive hearing loss.15
Kesser et al16 evaluated the impact of unilateral aural atresia on academic performance, and found that, in terms of amplification, only 1 in 8 students were using a hearing aid or bone conduction system. There are several issues which appear to drive this relatively low use rate. Unfortunately, even in 2019, parents of babies with UHL are often incorrectly told that many children do quite well with only one normal-hearing ear. Many studies have indicated that children with one normally hearing ear and one profound SNHL ear will not be able to tell where sounds originate (they often cannot tell who is speaking or where the sound is coming from), they tend to repeat grades more frequently than children with two normally hearing ears, and tend to have a higher rate of speech, language, and auditory processing delays, as well as lower vocabularies and social problems (see the article by Anne Marie Tharpe, PhD in this special issue of Hearing Review). While we don’t have the same level of information about the academic success and hearing difficulties of children specifically with unilateral conductive hearing loss, the surveys collected by Kesser et al showed that 65% of the children needed additional school resources, 45% needed speech therapy, 32.5% required an FM system, and 47.5% had an Individualized Education Plan (IEP).
Further, when faced with the daily challenge and cosmetic impact of wearing a bone conduction system on a softband, parents tend to delay decision-making until it is apparent that their child needs the support of a hearing device. As the child matures, decisions regarding whether to pursue ear reconstruction may impact the age at which a bone conduction implant (BCI) is pursued. Some parents may elect to seek the BCI after reconstructive processes are complete, while others are simply reticent to commit their child to the lifelong care and maintenance of a percutaneous abutment.
Until very recently, the only alternative to a BCI for children beyond their toddler years has been a softband solution. Unfortunately, softband solutions often have accompanying negative cosmetic implications and physical discomfort, which may result in inconsistent compliance and therefore inconsistent access to sound. For decades, bone conduction systems have been associated with pressure against the head or a percutaneous abutment offering direct bone conduction stimulation, while posing a lifelong risk of infection around the abutment site.

Figure 2. The ADHEAR System is indicated for people with conductive hearing loss, and is designed as a solution for people who cannot or do not want to undergo surgery or for people suffering from conductive hearing loss of uncertain duration. The system consists of an adhesive adapter that resembles what some might describe as a high-tech “sticker” containing a place for the audio processor to click onto.
In the past year, the United States saw the introduction of two pioneering technologies which fundamentally reshaped the entire process of delivering bone conducted sound. ADHEAR by MED-EL is a non-surgical, pressure-free, adhesive-based bone conduction system offering enhanced comfort and cosmetics with performance equivalent to standard softband systems (Figure 2).17-19 ADHEAR is FDA cleared for unilateral and bilateral conductive hearing loss and SSD. In addition to daily wear for those with a permanent conductive hearing loss, ADHEAR expands the possible use cases of a non-surgical bone conduction system to those with a defined transient CHL or CHL of chronic yet uncertain duration. The cosmetics of the ADHEAR system makes it acceptable to individuals of all ages and stages.

Figure 3. The Bonebridge System is cleared for use in conductive and mixed hearing losses as well as single-sided deafness for candidates age 12 and older. Bonebridge is the first bone-conduction implant that combines the benefits of intact skin with direct-drive stimulation of the bone.
The BONEBRIDGE System by MED-EL is an active transcutaneous bone conduction implant system delivering direct-drive bone conduction while keeping the skin intact (Figure 3). The recipient wears a slim audio processor coupled to the head by a gentle magnetic attraction (as has been done with cochlear implants for many decades). The system has been available in other countries since 2012. As such, considerable research related to safety, surgical, and audiologic outcomes is available in the peer-reviewed literature. The FDA clearance for the BONEBRIDGE in the United States is for individuals 12 years and older.
Conclusion
Innovations such as new technologies and expanded indications for existing technology can help address UHL and SSD and offer advances in comfort, cosmetics, and efficacy. Hearing care professionals play a key role in ensuring that potential candidates are aware of their options. While people with UHL and SSD have historically faced limited or less-than-ideal options, recent advances help ensure that patients with UHL and SSD enjoy a fuller range of sound. Hearing care professionals should feel confident counseling patients regarding the variety of options to help them better hear. Further, considering these new options and technologies, providers are encouraged to proactively reach out to UHL and SSD patients to review contemporary options and to help guide them to new and improved alternatives.
References
-
Van de Heyning P, Távora-Vieira D, Mertens G, et al. Towards a unified testing framework for single-sided deafness: A consensus paper. Audiol Neurotol. 2016;21:391-398.
-
Dillon MT, Buss E, Rooth MA, et al. Effect of cochlear implantation on quality of life in adults with unilateral hearing loss. Audiol Neurotol. 2017;22:259-71.
-
Niparko JK, Cox KM, Lustig LR. Comparison of the Bone Anchored Hearing Aid implantable hearing device with contralateral routing of offside signal amplification in the rehabilitation of unilateral deafness. Otol Neurotol. 2003;24:73-8.
-
Arndt S, Laszig R, Aschendorff A, et al. Cochlear implant treatment of patients with single-sided deafness or asymmetric hearing loss. HNO. 2017;65 (Suppl 2):S98-S108.
-
Van de Heyning P, Vermeire K, Diebl M, et al. Incapacitating unilateral tinnitus in single-sided deafness treated by cochlear implantation. Ann Otol Rhinol Laryngol 2008;117(9):645-52.
-
Vermeire K, Van de Heyning P. Binaural hearing after cochlear implantation in subjects with unilateral sensorineural deafness and tinnitus. Audiol Neurotol. 2009;14(3):163-71.
-
Buss E, Dillon MT, Rooth MA, et al. Effects of cochlear implantation on binaural hearing in adults with unilateral hearing loss. Trends in Hearing. 2018;22:1-15.
-
Galvin JJ, Fu QJ, Wilkinson EP, et al. Benefits of cochlear implantation for single-sided deafness: Data from the House Clinic-University of Southern California-University of California, Los Angeles Clinical Trial. Ear Hear. 2019;40(4):766-81.
-
Arndt S, Prosse S, Laszig R, et al. Cochlear implantation in children with single-sided deafness: Does aetiology and duration of deafness matter? Audiol Neurotol. 2015;20 (suppl 1):21-30.
-
Tavora-Vieira D, Rajan GP. Cochlear implantation in children with congenital and noncongenital unilateral deafness: A case series. Otol Neurotol. 2015;36:235-9.
-
de Wolf M, Hendrix S, Cremers C, et al. Better performance with bone-anchored hearing aid than acoustic devices in patients with severe air-bone gap. Laryngoscope. 2011;121: 613-616.
-
Mylanus E, van der Pouw K, Snik A, et al. Intraindividual comparison of the bone-anchored hearing aid and air-conduction hearing aids. Arch Otolaryngol Head Neck Surg. 1998;124: Mar, 271-276.
-
Son HJ. Congenital Aural Atresia (Grand Rounds Presentation, UTMB Dept of Otolaryngology). October 17, 2007. Available at: https://pdfs.semanticscholar.org/d301/4823679e0e94d7ae1f000d3d36706249188f.pdf
-
Centers for Disease Control and Prevention (CDC), National Center for Health Statistics. Birth and Natality. 2017. Available at: http://www.cdc.gov/nchs/fastats/births.htm
-
Centers for Disease Control and Prevention (CDC). Facts about anotia/microtia. November 1, 2018. Available at: https://www.cdc.gov/ncbddd/birthdefects/anotia-microtia.html
-
Kesser BW, Krook K, Gray LC. Impact of unilateral conductive hearing loss due to aural atresia on academic performance in children. Laryngoscope. 2013;123(9):2270–5.
-
Neumann K, Thomas JP, Voelter C, Dazert S. A new adhesive bone conduction hearing system effectively treats conductive hearing loss in children. Int J Ped Otorhinolaryngol. 2019;122:117-125.
-
Gawliczek T, Munzinger F, Anschuetz L, et al. Unilateral and bilateral audiological benefit with an adhesively attached, noninvasive bone conduction hearing system. Otol Neurotol. 2018 Sep;39(8):1025-1030.
-
O’Donnell AT. Non-surgical advances in treatment for conductive hearing loss. Hearing Review. 2018;25(9):36-38.

, is Acoustic Systems Manager, and Allison Racey, AuD, is Manager of Regulated Research at MED-EL Corp, Durham, NC.
CORRESPONDENCE can be addressed to Dr O’Donnell at: [email protected]
Citation for this article: O’Donnell A, Racey A. Managing people with sensorineural and conductive unilateral hearing loss and single-sided deafness. Hearing Review. 2019;26(10)[Oct]:24-26.
Other articles in the October 2019 Hearing Review special edition on unilateral hearing loss:
- Introduction to Special Edition: Unilateral Hearing Loss: Underappreciated, Undertreated, By Karl Strom
- Contralateral Routing of Signal: A Status Report 2019, By Douglas L. Beck, AuD, and Virginia Ramachandran, AuD, PhD
- Unilateral Hearing Loss in Children: Current Perspectives, By Anne Marie Tharpe, PhD
- A New Dual-Streaming CROS/BiCROS Solution, By Susanna Løve Callaway, AuD, and Pernille Aaby Gade
- Managing People with Sensorineural and Conductive Unilateral Hearing Loss and Single-Sided Deafness, By Amanda O’Donnell, AuD, and Allison Racey, AuD
Also see:
- The Impact of Unilateral Hearing Loss on Adult Life, By James Galloway, MSc; Vicky Zhang, PhD; Vivienne Marnane; Sanna Hou, MClinAud; Greg Stewart, and Fabrice Bardy, PhD

