Final Word | August 2018 Hearing Review
I stayed late in the office a few weeks ago to see a friend of a friend who had a recent problem with hearing in one ear. He described that after a tropical vacation swimming in warm water followed by a long flight home, he noticed an annoying unilateral plugged sensation. He saw a primary care physician who removed some wax with irrigation and sent him home with advice to use cerumenolytic drops.
After a few days with no relief of the symptoms, he asked me for a consultation and advice. Otoscopy revealed that the canal was fully occluded with cerumen behind exostoses that reduced the ear canal opening about 50-60%. I asked about his history, and he confirmed that he had spent quite a bit of time swimming in cold water in his earlier years.
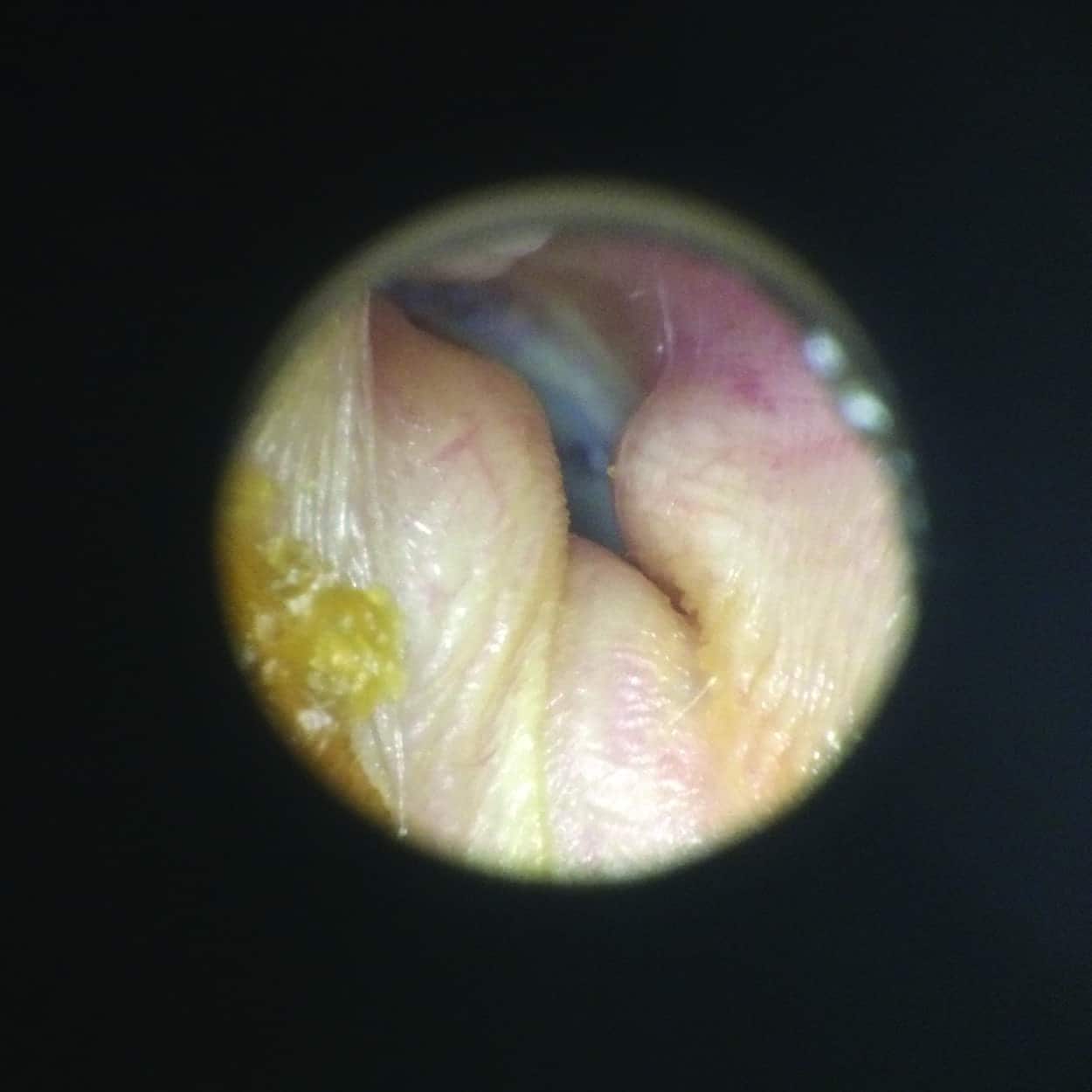
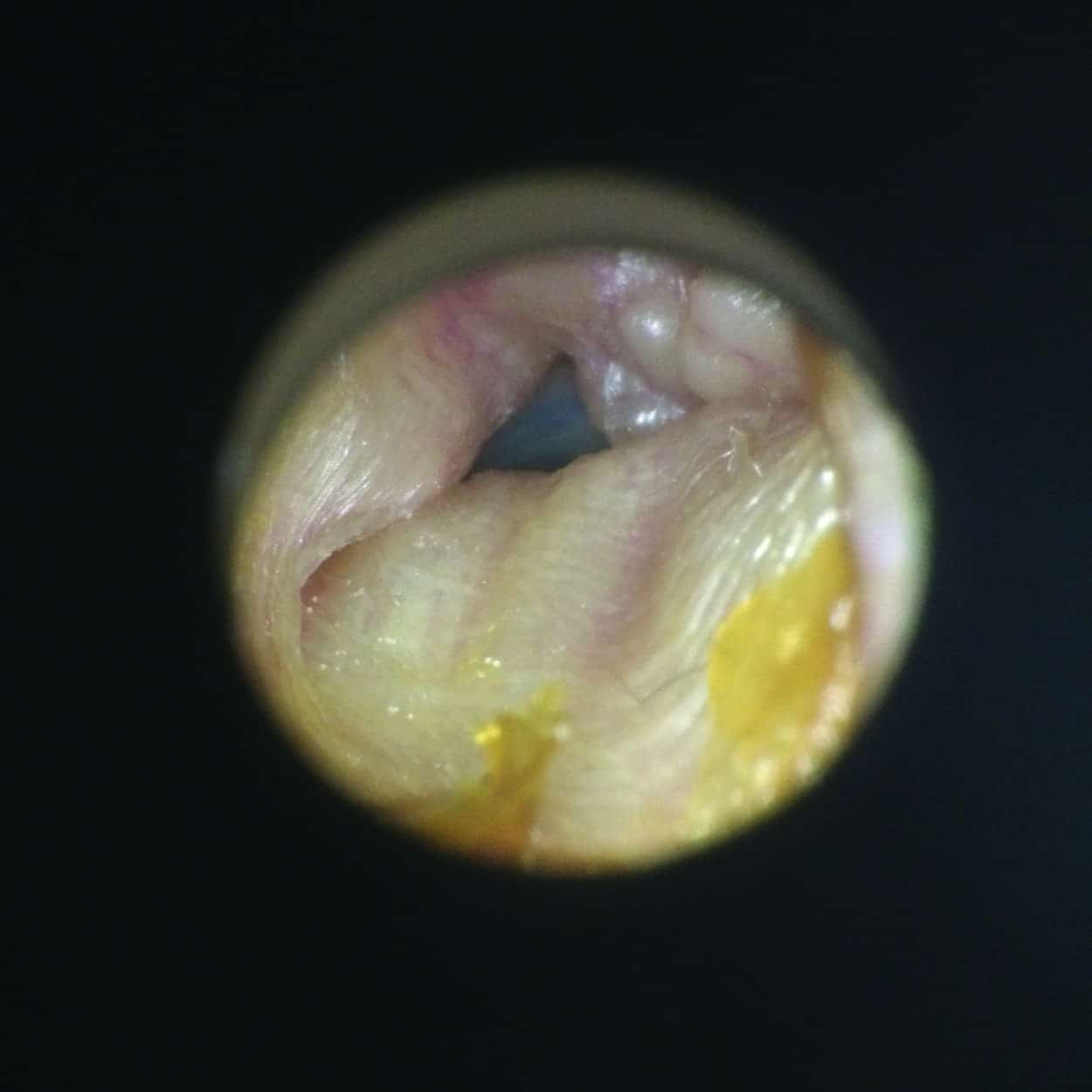
Left and right otoscopy of ear canals with large external auditory canal exostoses. The cartilaginous portions of the ear canals were typical and clear of obstruction up to the bony portion of the canal. The patient has a history of successfully wearing receiver-in-canal (RIC) hearing aids with non-custom silicone tips.
I explained that the exostoses complicated the removal of cerumen because they obstructed the canal enough to make curettage or suction difficult, and possibly uncomfortable for him. I referred him to a local ENT we often work with. He said he would continue with the cerumenolytics and seek the ENT consult if necessary.
Working in a Southern California beach community, we often see cases of external auditory canal exostoses or “surfer’s ear.” I have seen it in an octogenarian who, while at Yale, “spent a bit of time in the water” while perfecting his technique in a rowing shell. I’ve also seen it in countless younger men and women here locally who take advantage of the surf. Often, the bony growths are cosmetic anomalies only visible to someone with an otoscope. Other times, the growths become large enough to nearly occlude the ear canal, resulting in a propensity for wax occlusion or otitis externa because water becomes trapped between the exostoses and the eardrum.
An excellent article from 1999, “Prevalence of External Auditory Canal Exostoses in Surfers” by Wong et al1 describes the incidence and pathology of exostoses with cold water exposure as a suspected risk factor. Interestingly, the colder the water, the shorter the average time of exposure required to create the exostoses. Surgery to remove the tumors is possible, but typically only pursued if there is hearing loss or repeated problems with otitis externa.
For those of us with the otoscopes, exostoses are either mildly interesting, or a complication for cerumen management and deep-canal hearing aid fittings.
As shown in the accompanying images, external auditory canal exostoses can dramatically distort the anatomy of the ear canal, obscuring the view of the tympanic membrane, and often complicating the management of ear canal hygiene and limiting the options for hearing aids. The bony tumors are essentially bone covered with skin and the very little cushioning tissue in between makes them very sensitive to touch. Irrigation can be a problem because of the tendency for the residual space behind the exostoses to harbor water and increase the chances of fungal or bacterial infection.
The Final Word? In spite of the complications noted above, most of these individuals can easily be fit with standard or custom products if they are candidates for hearing aids. The bony projections are limited to the bony portion of the ear canal, and there is typically enough anatomy in the cartilaginous portion of the ear canal to accommodate an earmold or custom product, with the exception of deep-fitting hearing aids. Care should be exercised in packing the ear canal to leave enough space for the impression material to model the ear canal, but also to ensure protection to prevent migration of the impression material into the lumen of the residual canal space, which would obviously present a serious complication.
Citation for this article: Van Vliet D.Bad to the bone: Surfer’s ear. Hearing Review. 2018;25(8):34.
References
-
Wong BJF, Cervantes W, Doyle KJ, et al. Prevalence of external auditory canal exostoses in surfers. Arch Otolaryngol Head Neck Surg. 1999;125:969-972.