The popularity of open-canal fittings has brought new importance to the issue of signal processing delays in hearing aids. This article provides a perspective on acceptable and unacceptable delays in advanced hearing instruments, and looks at processing types and special features that contribute to delays in hearing aid processing.

|

|
| This article was submitted to HR by Rebecca Herbig, AuD, research and training audiologist, and Josef Chalupper, PhD, director of audiology at Siemens Audiologische Technik, Erlangen, Germany. Correspondence can be addressed to or . | |
For people who wear hearing aids, sounds are transmitted into the ear canal via two different paths. In the first path, sound travels around the hearing aid or past the earmold plumbing directly into the ear canal. The more “open” the fitting and the more normal the hearing, the greater the contribution of this pathway. In the second path, the signal passes through the hearing aid, is processed, and is then delivered into the ear canal.
These two paths have inherently different time delays before a given sound is perceived by the hearing aid user. Direct sound heard via the first path has the least delay, and is perceived before the amplified sound, which has to be first processed by the hearing aid circuitry. The delay introduced by the hearing aid has become more of an issue in the past 10 years with the routine use of digital hearing instruments, which have a considerably longer delay than their analog counterparts.
While the delay caused by digital hearing aid amplification is relatively short, and measured only in milliseconds, the sound quality of the speech signal may still be compromised. We know that, when the delay is about 10 milliseconds, the direct sound and the amplified sound interact with each other and cause spectral ripples, which alter the timbre of the sound. Because these spectral ripples are only present when the two sounds are of a similar intensity, they are not present when the amplified sound is significantly louder than the direct sound. When the delay becomes longer, the patient may notice an “echo effect,” and when longer yet (more than 40 ms), the auditory information may fall out of synchronization with the visual information and interfere with speech reading.1
The detrimental effects of hearing aid delay are dependent upon the severity of the hearing loss. As the hearing threshold worsens, the individual is able to hear less of the direct sound transmission and the delay is not as noticeable. Also, as hearing becomes worse, the physical fitting is tighter in the ear canal (eg, less venting). This results in greater attenuation of the direct sound, and thereby reduces the possibility of a noticeable delay. As digital signal processing inevitably introduces delays, and any delay will cause some spectral ripples, the obvious question is: “How much delay is acceptable for all, or at least the majority of, patients?”
Research on Hearing Aid Processing Delays
Over the past 10 years, Stone and colleagues have conducted considerable research about tolerable hearing aid delays.2-5 In general, their findings suggest that disturbance increases monotonically with increasing delay, with delay times as low as 20 to 30 ms rated as disturbing for those with mild-to-moderate hearing losses. For normal-hearing listeners, even speech production is affected when the delay exceeds 30 ms. Another group of researchers working with actual commercial hearing aids, however, found that delays as small as 10 ms affect sound quality.6
A factor that makes hearing aid delays even more of a concern in recent years is the popularity of open-canal (OC) fittings. As the term suggests, OC fittings leave the ear canal much more open than traditional earmolds or custom instruments. As a result, more sound travels directly into the open ear canal and is potentially more audible to the hearing aid user. Moreover, patients who typically wear OC fittings are those with only a mild-to-moderate hearing loss—the same group of users who have the greatest potential to be affected by hearing aid delay.
A recent study7 showed that, in OC fittings for simulated hearing losses that started at 2 and 1 kHz, processing delays may need to be as low as 5 and 6 ms, respectively, to avoid compromises in sound quality. However, these researchers did state that, because the simulations used in the experiment introduced confounding factors, users may actually tolerate longer delays from real hearing instruments than the values they suggested.
Hearing Aid Processing
With digital signal processing, each “feature” of the hearing instrument can add to the total group delay. For example, a hearing aid with more channels, more advanced digital noise reduction, and a more sophisticated feedback reduction system may have more group delay than a hearing aid without these features.
The type of signal processing is also a factor. Hearing instrument manufacturers primarily use two methods for signal processing and frequency analysis. The first is the use of a filterbank, which employs filters to split up the input signal into channels by processing the signal, sample by sample. Other manufacturers use a Fast Fourier Transformation (FFT) scheme that processes a block of samples at once.
Both approaches obey the “Acoustic Uncertainty Principle,” which states that the time-bandwidth product is constant. That is, if spectral resolution is increased, temporal resolution will decrease, and vice versa. Thus, the narrower the channels are (whether filterbank or FFT), the longer the group delay. The fundamental difference between the two approaches is that, with FFT, the bandwidth of the channels is the same across frequency, whereas with filterbanks, bandwidth can vary across frequency.
|
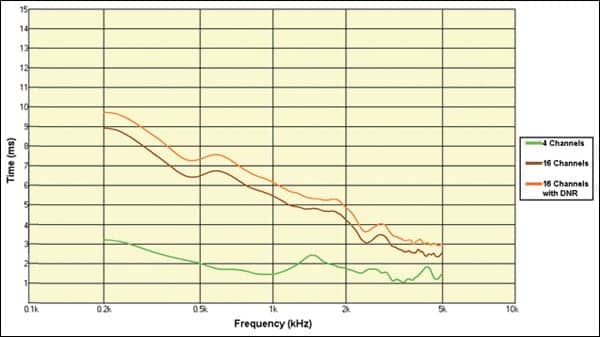
| FIGURE 1. Plotting of the digital processing delay for three conditions in Siemens hearing aids: 4-channel device (green), 16-channel device (brown), and a 16-channel device with an additional digital noise reduction algorithm activated (orange). |
The filterbank approach typically mimics the logarithmic layout of the basilar membrane (“critical bands”) and has finer frequency resolution for lower frequencies than for higher frequencies. The narrower filters required for the lower frequencies cause more delay than those for higher frequencies. Research has shown that, if this frequency-dependent delay is too long, it can cause listeners to hear a consonant at the same time or before a vowel, even though in the original speech signal, the consonant occurred after the vowel.4
In a FFT approach, an entire block of signals is processed at once with uniform analysis bandwidth across frequency. Therefore, unlike the filterbank, the delay caused by Fourier Transformation is uniform across frequencies.
Regardless of which method is used for signal processing, the advent of ever more sophisticated signal processing sometimes also increases hearing aid delay as the signal must travel through an increasing number of processers and algorithms.
Laboratory Measures
Siemens hearing aids employ a filterbank for signal processing. Even with the increasing number of gain channels and advanced signal processing algorithms, the instruments maintain processing delay that is within tolerable limits established by research findings.
The laboratory measure of hearing aid delay can be accomplished by calculating the derivative of the phase response.6 This method is used in some commercially available electroacoustic measurement systems. For the measurements reported below, an ACAM5 system from Acousticon was used. The results of these measures are then typically displayed on a millisecond/frequency chart, as shown in Figure 1.
As mentioned earlier, in a filterbank, delay typically decreases with increasing frequency, and this effect becomes more pronounced as more channels are added. That is, a 16-channel instrument has significantly higher delay than a 4-channel device (especially in the low frequencies), even when both instruments have similar features activated. The bottom green line in Figure 1 is the processing delay for a Siemens 4-channel device. One can see that, for the majority of the frequency range, the delays are at or below 2 ms. In comparison, the delays for the 16-channel instrument (brown line) are acceptable, but the delays are considerably longer—especially for the lower frequencies.
|
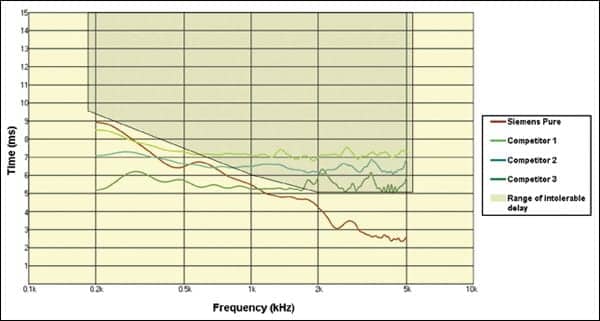
| FIGURE 2. Display of digital processing delay for four different OC hearing instruments. The gray area indicates the range of delay shown to be intolerable according to research.7 |
Finally, as discussed, additional features can also cause further processing delays. In this example, we have added the Siemens SoundSmoothing noise reduction algorithm (Figure 1, orange line). Note that the group delay is now increased by nearly another millisecond across the frequency range.
In order to avoid the spectral ripples, which occur when direct sound and amplified sound are of similar intensity levels, an algorithm was developed in which channels with less than 3 dB of prescribed gain are completely turned off. This of course relates directly to OC fittings, as these patients typically have normal hearing through 1000 or even 1500 Hz. This OC fitting approach is also consistent with the recent findings of Keidser et al8 who reported that, with an open ear canal, the lower frequencies are perceived as slightly louder (~4 dB).
| HR Podcasts #24 Parents vs Kids: Perceptions of Hearing Loss Among Immediate Family Members, with Thomas Powers, PhD. Aired 6/11/09. #25 & #26 “Top-10” Expert Insight Questions, Pts 1 & 2, with Michael Nilsson, PhD. Aired 7/23/09 (Pt 1) and 7/30/09 (Part 2). #27 Changing Dynamics in Dispensing and EarQ, with Ed Keller. Aired 8/13/09. #28 Improving BTE and Mini-BTE Fittings with Mechanical Adjustments to the Earmold and Plumbing, with Brian Taylor, AuD. Aired 10/8/09. #29 Using the Color Speech Range Audiogram, with Dennis Hampton, PhD. Aired 10/22/09. #30 A User-Programmable and Adjustable Hearing Aid, with David Yu. Aired 11/19/09. #31 The Challenge of Aging: Hearing Care for Older Adults Conference 2009, with Louise Hickson, PhD 12/10/09 |
In their study on the effects of OC devices, Stone and colleagues7 reported that, for mild hearing loss starting at 2 and 1 kHz, the hearing instrument should have delays no longer than 5 and 6 ms, respectively. To assess compliance with this recommendation, we evaluated four commercially available OC devices from different manufacturers, using the laboratory test procedures described earlier. The results are shown in Figure 2. The brown line on the chart represents the Siemens Pure. Note that, for the key frequencies in an OC fitting (>1000 Hz), the instrument clearly falls at or below the suggested delays. However, two of the other three devices have delays that are at, or exceed, recommended values.
One should keep in mind the researchers’ caveat that users may actually tolerate longer delays from real hearing instruments (ie, above the 5 to 6 ms values their study suggested).7 However, the extent that a delay is “noticeable” does differ somewhat among individual patients, and is related to degree of hearing loss, cognitive status, and other factors. Therefore, it is also possible that, for isolated cases, an even shorter delay than shown in Figure 2 for the Siemens Pure might be required to achieve optimum sound quality. In such instances, we recommend disabling some of the adaptive signal processing features, which add to hearing aid delay. Switching to a device with fewer channels, and therefore fewer filters, would also be a reasonable solution.
Summary
All hearing aids have processing delays, and these delays have the potential to interfere with amplified sound quality of speech. The popularity of OC fittings has increased the focus on this issue, as delays must be the shortest when the ear canal is open. Tolerable delay values are well established, and this issue is thoroughly studied when hearing aid processing is designed and new algorithms are implemented. As we have reported here, Siemens products are designed so that effective signal processing is maximized, while all delays still fall at or below research-recommended values.
References
- Dillon H. Hearing Aids. New York City: Thieme; 2001.
- Stone MA, Moore BCJ. Tolerable hearing aid delays. I. Estimation of limits imposed by the auditory path alone using simulated hearing losses. Ear Hear. 1999;20:182.
- Stone MA, Moore BCJ. Tolerable hearing aid delays. II. Estimation of limits imposed during speech production. Ear Hear. 2002;23:325-338.
- Stone MA, Moore BCJ. Tolerable hearing aid delays. III. Effects on speech production and perception of across-frequency variation in delay. Ear Hear. 2003;24:175-183.
- Stone MA, Moore BCJ. Tolerable hearing-aid delays: IV. Effects on subjective disturbance during speech production by hearing-impaired subjects. Ear Hear. 2005;26:225-235.
- Dillon H, Keidser G, O’Brian A, Silberstein H. Sound quality comparisons of advanced hearing aids. Hear Jour. 2003;56:30-40.
- Stone MA, Moore BC, Meisenbacher K, Derleth R. Tolerable hearing aid delays. V. Estimation of limits for open canal fittings. Ear Hear. 2008;29:601-617.
- Keidser G, Carter L, Chalupper J, Dillon H. Effect of low-frequency gain and venting effects on the benefit derived from directionality and noise reduction in hearing aids. Int J Audiol. 2007;46(10):554-68.
Citation for this article:
Heurig R, Chalupper J. Acceptable Processing Delay in Digital Hearing Aids. Hearing Review. 2010;17(1):28-31.

.gif)