Tech Topic | November 2020 Hearing Review
By DavId Fabry, PhD, Thomas Burns, PhD, Martin McKinney, PhD, and Achin Bhowmik, PhD
When introduced in 2018, Starkey’s Livio AI was the industry’s first hearing aid with embedded motion sensors and artificial intelligence (AI).1 In addition to the capabilities expected of advanced hearing aids, these devices automatically detect falls and send alert messages to pre-selected contacts.2 In 2020, the Livio Edge AI platform added Edge Mode to continuously monitor and characterize the acoustic environment with onboard machine-learning technology that dynamically applies appropriate levels of gain, noise management, directionality, and other features when necessary. When Edge Mode is employed via a “double tap” or button press, the operating parameters for “all around” listening are expanded, allowing access to alternative settings that optimize comfort and clarity in challenging listening environments. Previous investigations have demonstrated that most patients find Edge Mode easy to use and prefer it over “Normal” hearing aid settings in restaurant noise, when communicating in a car, and in reverberant listening environments.3
During the COVID-19 pandemic, health and government officials are encouraging or even mandating community-wide face mask wearing to reduce potential pre-symptomatic or asymptomatic transmission of the virus to others. This practice, in combination with social distancing (ie, keeping >6 feet apart), has helped decrease spread of the virus, but it has also provided a barrier to clear, empathetic communication, particularly for those with hearing loss.4,5
The Impact of Face Masks and Social Distancing on Speech Audibility
Figures 1-3 demonstrate the impact on speech audibility when a face mask is worn and physical distancing is used between talkers and listeners. In Figure 1, the green curve represents the sound pressure levels recorded from the ear simulator of a Knowles Electronics Manikin for Acoustic Research (KEMAR) for conversational speech (The Rainbow passage) presented at 65 dB SPL measured at a “typical” conversational distance of 3 feet between the talker and the listener.
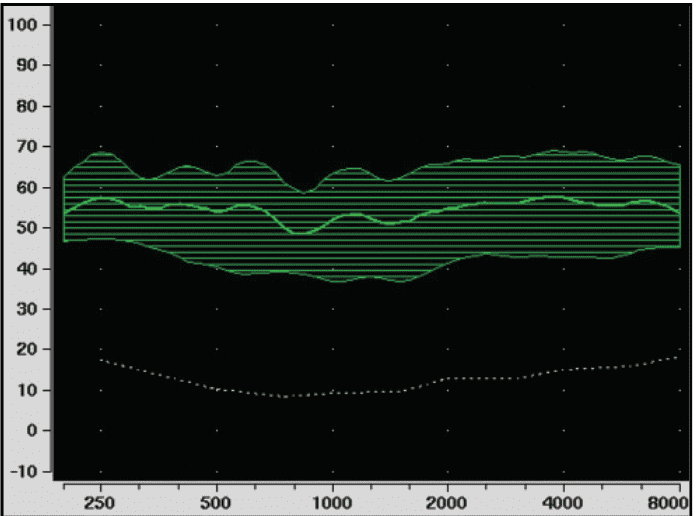
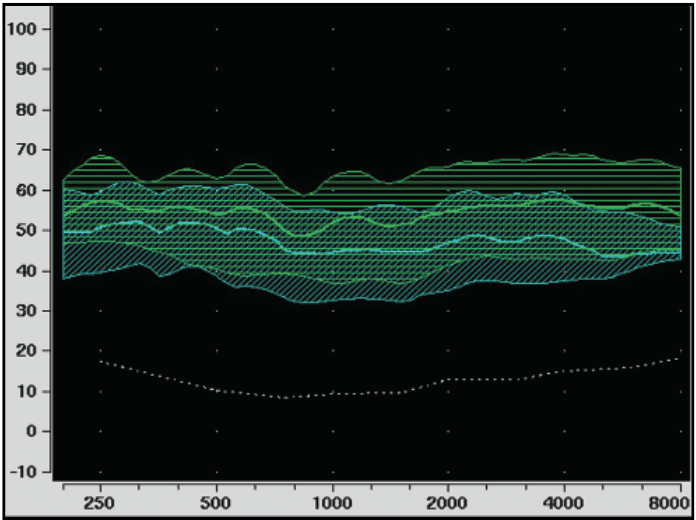
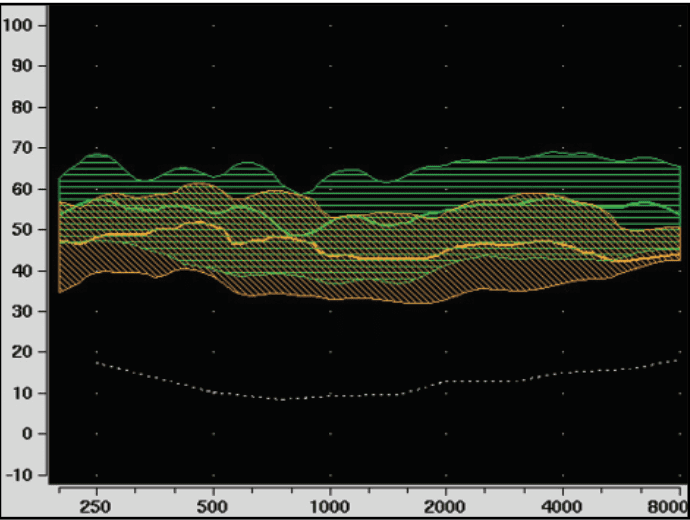
Figure 2 shows the impact of social distancing and is measured with the distance between talker and listener increased to 6 feet. This reduces sound pressure levels by approximately 6 dB.
Figure 3 demonstrates the additional reduction in audibility when a N95 face mask (3M 8210 Plus) is worn along with 6 feet between talker and listener. Clearly, the use of face masks and physical distancing reduces audibility for speech, even for individuals with normal hearing, as the speech sound recorded at the listener’s eardrum is decreased by up to 15 dB relative to the no-mask condition.6
Hearing Loss Complicates the Issue More
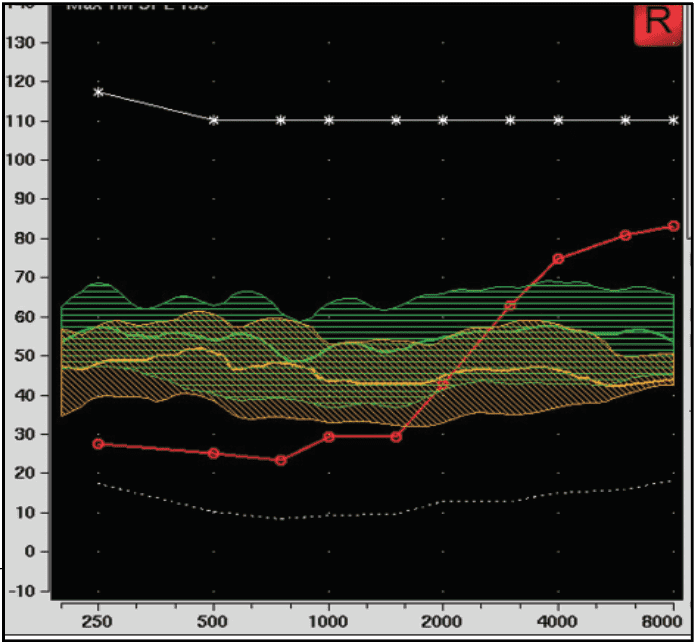
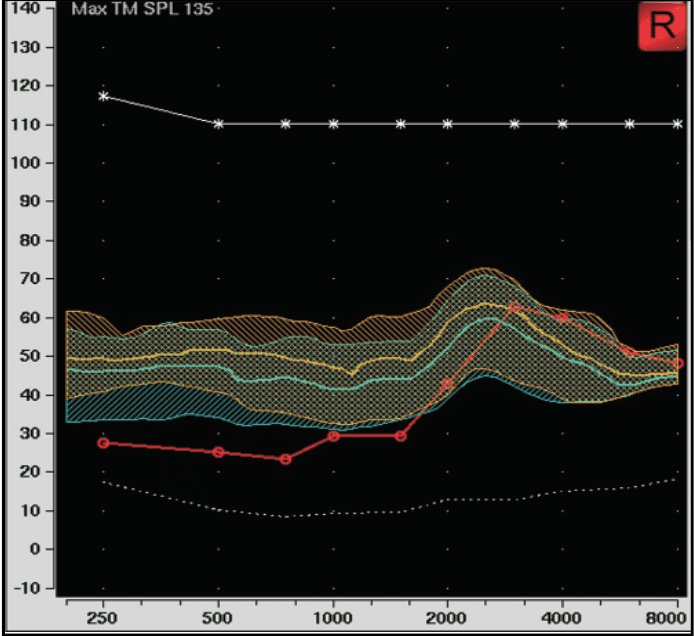
This situation is compounded for persons with hearing loss. Figure 4 illustrates the impact on unaided speech audibility for an individual with a gradually sloping high-frequency hearing loss (red curve) for the same conditions as represented in Figure 3. For this individual, critical high-frequency information is reduced when the combination of face masks and social distancing is used. The computed Speech Intelligibility Index (SII) is reduced from 0.65 to 0.52 and predicts a reduction of up to 25% in speech intelligibility. When background noise is added, critical speech information may be rendered nearly inaudible for those with hearing loss.
Hearing Aids Can Help!
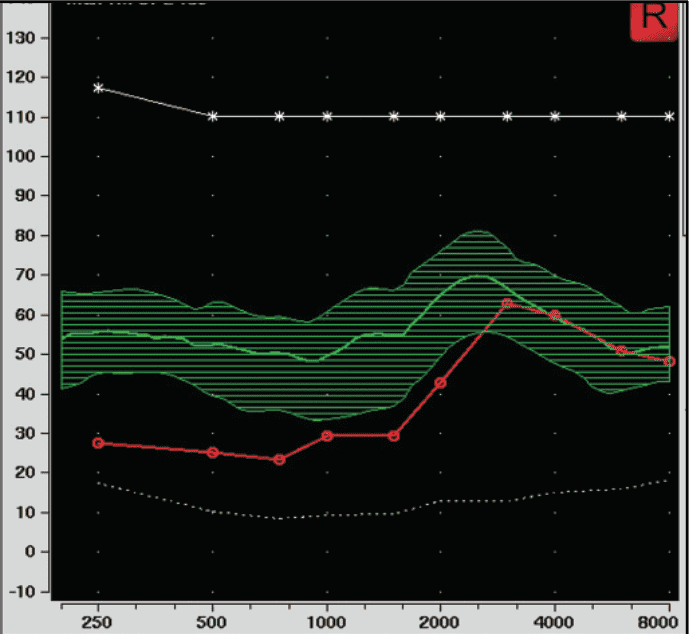
Figures 5-6 demonstrate the impact of social distancing and face mask use on speech audibility for a person with properly-fit hearing aids. Figure 5 illustrates the amplified speech spectrum for a talker-listener distance of 3 feet when no mask is worn. Figure 6, however, shows how the combination of use of an N95 mask and social distancing (6 feet) reduces audibility for the “Normal” memory (teal curve). Therein lies the “face-masking dilemma”: while protecting against the spread of COVID-19, the use of face masks, social distancing, and loss of lipreading cues make communication difficult—even with properly-fitted hearing instruments!
All Masks Are NOT Created Equal!
Eight months into the pandemic, individuals now have an array of face mask choices available to them, including disposable medical face masks, washable cloth masks, and masks with a clear window for lipreading restoration. For many, the solution reflects the best combination of protection, comfort, convenience, and proper fit. Another factor, particularly for those with hearing loss, is increasingly focused on acoustic performance and preservation of visual cues.
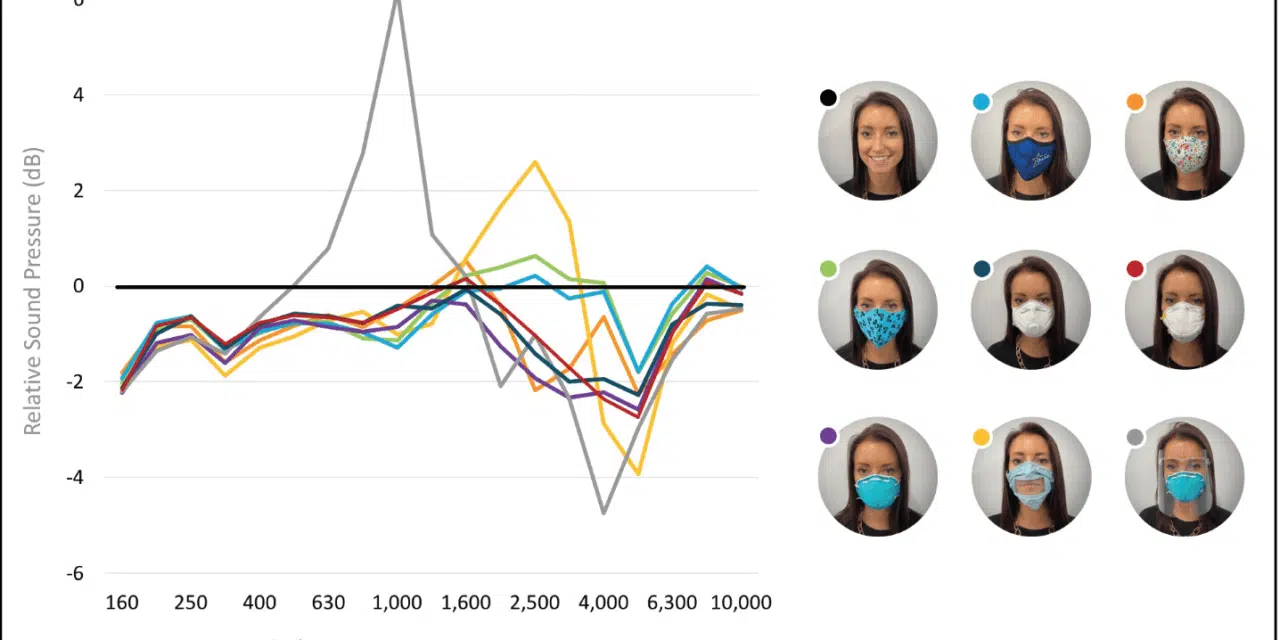
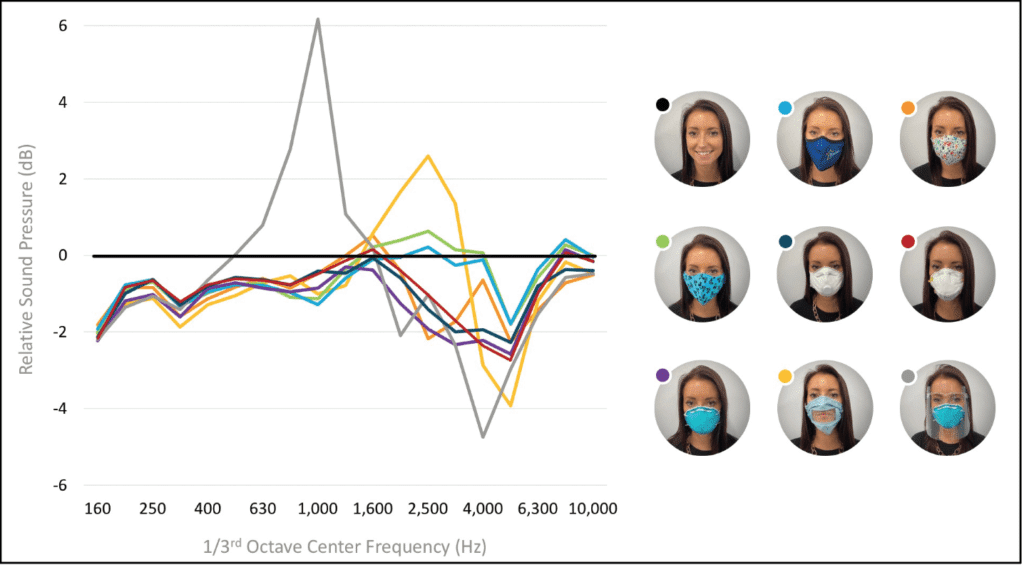
To assess differences in sound attenuation across face masks, acoustic measurements were made on many of the latest commercially available styles. Figure 7 illustrates the differences for a range of mask types. The data are normalized relative to when no mask is worn, which is depicted by “zero” line on the x-axis. While all of the masks reduce important high-frequency sound information, there is significant variation across fabric, medical, and paper masks, especially those equipped with a plastic “window.” One unexpected finding was that face masks and face shields that used clear plastic had an enhancement of several dB in the low/mid frequencies along with a reduction in the high frequencies.7,8 These data illustrate the challenge of using a predetermined compensation scheme, with fixed high-frequency gain adjustment, to adapt for the impact of social distancing and face mask use.
Restoring Speech Audibility
User-activated Edge Mode in Livio Edge AI hearing aids optimizes speech audibility and sound quality in all listening environments by assessing the levels of speech and noise present using an onboard AI model trained with machine-learning technology, and then dynamically applying gain, output, noise management, directional microphones, and other features to optimize sound for each person in each environment. In effect, Edge Mode is “agnostic” to which mask is worn, talker-listener social distancing, or presence of background noise; the technology optimizes speech audibility in every listening situation.
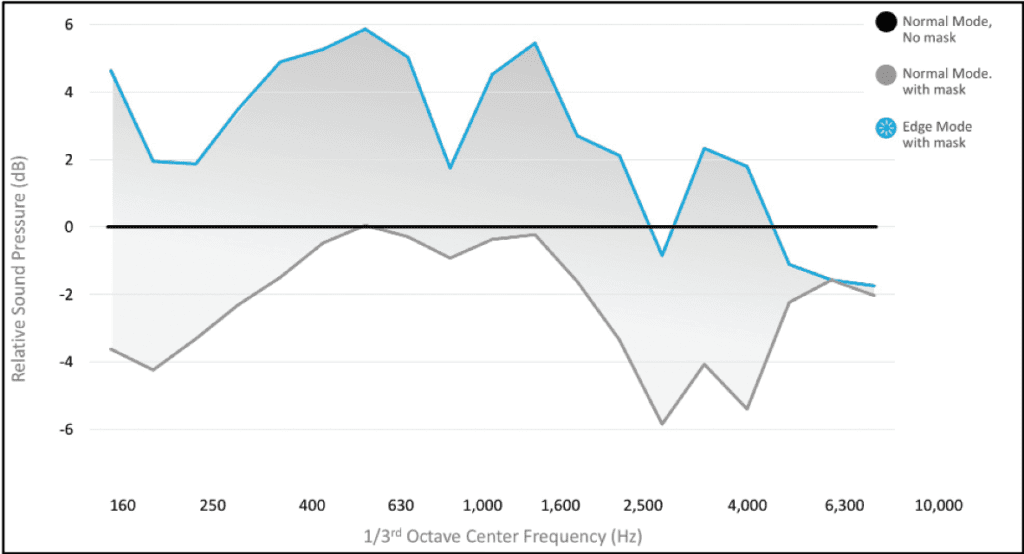
Figure 8 illustrates the relative difference in speech audibility with 6-foot social distancing and +5 dB signal-to-noise ratio (SNR) for conditions when the talker is not wearing a mask, in the “Normal” program and when “Edge” mode has been activated. In this example, speech levels are greater than when no mask is used, which helps provide additional benefits to offset the loss of visual cues gained by lipreading when a mask is worn.
Mask Mode for Livio AI
Starkey has also introduced a “Mask Mode” solution that provides gain offsets, based on the measurements from the large variety of face mask types (see Figure 7). For Livio AI 1200-2000 products, hearing aid users may select a “custom” program that increases gain by 4 dB for frequencies 2.0-3.9 kHz and 6 dB from 4.0-9.4 kHz relative to the prescribed Normal program. In addition, fixed directional microphones are activated to emphasize speech sounds in front of the hearing aid user. While not customized for the specific face mask, social distance or background noise conditions, Mask Mode is designed to improve communication by hearing aid users when encountering communication challenges posed by the COVID-19 pandemic.9
User Preference for Edge Mode for Masks and Mask Mode
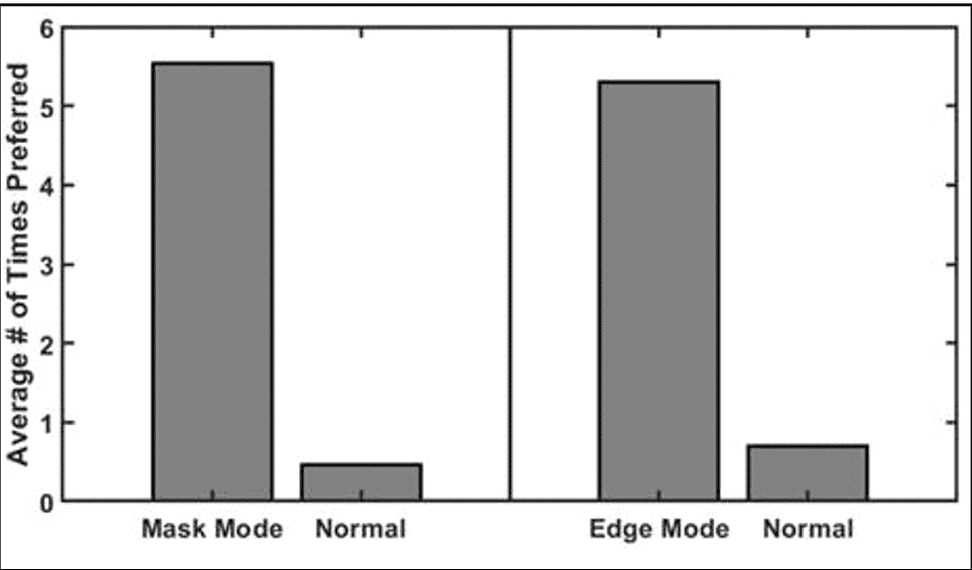
A total of 13 hearing aid users ranging in age from 56 to 84 years, with an average mild sloping to moderately severe high-frequency hearing loss, listened to recordings (The Rainbow passage) in background noise with a +5 dB SNR. Initially, preferred listening level was established for the prescribed (Normal) program when no face mask was worn. Subsequently, no volume adjustments were allowed, and blinded paired-comparison preference judgments for speech clarity and intelligibility were made between the 1) Normal program and Edge Mode for Masks, and 2) Normal program and Mask Mode for conditions when the talker wore an N95 medical face mask. Each subject made 6 preference judgements per condition. Results are shown in Figure 9. These data were analyzed using two Wilcoxon signed-rank tests (one for Mask Mode vs. Normal and one for Edge mode vs. Normal). They indicate that both Mask Mode and Edge Mode were preferred relative to the Normal program when the talker was using a medical-grade N95 face mask.
Summary
The challenges presented by social distancing and face masks make communication more difficult. Fixed offsets are offered in “Mask Mode” which is selected by the hearing aid user to improve communication when face masks are worn. Edge Mode for Masks, by comparison, uses a native AI model trained with machine learning technology to instantaneously optimize speech audibility to offset communication challenges presented by face masks, social distancing, and background noise. With AI at their fingertips, patients can simply “tap” to hear—whenever and wherever they want to hear better—without the need to access manual volume controls or smartphone applications. In laboratory tests, both of these solutions (Edge Mode for Masks and Mask Mode) were significantly preferred by hearing aid users over the “Normal” prescription targets when the talker was using a medical-grade N95 face mask. For face masks that deviate from the “average” mask characteristics, however, Edge Mode for Masks provides an effective, personalized acoustic solution in quiet and noisy listening environments.
Acknowledgement
The authors thank Tracie Tuss, AuD, for her assistance in the data collection.

Correspondence can be addressed to Dr Fabry at: [email protected].
Original citation for this article: Fabry D, Burns T, McKinney M, Bhowmik A. “Unmasking” benefits for hearing aid users in challenging listening environments. Hearing Review. 2020;27(11):18-20.
References
1. Hsu J. Starkey’s AI transforms hearing aids into smart wearables. IEEE Spectrum. https://spectrum.ieee.org/the-human-os/biomedical/ devices/starkeys-ai-transforms-hearing-aid-into-smart-wearables. Published August 27, 2018. Accessed September 2020.
2. Burwinkel J, Xu B, Crukley J. Preliminary examination of the accuracy of a fall detection device embedded into hearing instruments. J Am Acad Audiol. 2020;31(06):393-403.
3. Harianawala J, McKinney M, Fabry D. Intelligence at the edge. Starkey white paper. https://starkeypro. com/pdfs/technical-papers/Intelligence_at_the_Edge_ White_Paper.pdf .
4. Eikenberry SE, Mancuso M, Iboi E, et al. To mask or not to mask: Modeling the potential for face mask use by the general public to curtail the COVID-19 pandemic. Infectious Disease Modelling. 2020;5:293-308.
5. Hulzen RDT, Fabry DA. Impact of hearing loss and universal face masking in the COVID-19 era. Mayo Clinic Proceedings. 2020;95(10):2069-2072.
6. Goldin A, Weinstein B, Shiman N. How do medical masks degrade speech reception? Hearing Review. 2020;27(5):8-9.
7. Corey RM, Jones U, Singer AC. Acoustic effects of medical, cloth, and transparent face masks on speech signals. Journal of the Acoustical Society of America. 2020;148:2371.
8. Martin L. NAL update: Impact of face masks and face shields on communication. Hearing Review. 2020;27(10):28-29.
9. National Acoustic Laboratories. NAL mask adjustments to overcome the effect of face masks for hearing aid users. https://www.nal.gov.au/nal-mask-adjust/.