
Screening a patient for potential skin cancer lesions and referring patients to a medical professional, when warranted, can result in a life-saving intervention. Here’s how to do it.
Patient Care | February 2018 Hearing Review
Knowing the ABCDEs of skin cancer can prove to be a life-saver
According to the Skin Cancer Foundation, skin cancer is defined as “the uncontrolled growth of abnormal skin cells. It occurs when unrepaired DNA damage to skin cells triggers mutations, or genetic defects, that lead the skin cells to multiply rapidly and form malignant tumors.”1 Skin cancer is the most prevalent form of cancer, affecting almost 1 in 5 Americans at some point during their lives, with increasing incidence each year.2 Skin cancer also accounts for approximately one-third of all diagnosed cancers. Although these statistics are high, skin cancer is also the most preventable type of cancer; therefore, education and skin cancer screenings are recommended. With early detection, outcomes are more favorable and lives can be saved.
Hearing professionals are uniquely positioned to screen for skin cancers of the face and head in that they provide services that focus on the visualization of the affected areas. Many hearing professionals have noticed and alerted patients to consult with their medical providers about a suspicious lesion on the ear. There are many stories of patients returning to thank the hearing professional after a physician confirmed a skin cancer. The patient’s perception of concern for their wellbeing may result in a patient for life. This article provides a skin cancer screening model utilized and validated in the authors’ clinic.
Understanding and Identifying Skin Cancers
Two non-melanoma skin cancers—basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)—are the most common forms of skin cancer, with an estimated 5.4 million existing cases in 2012 in the United States.3 Non-melanoma skin cancers can cause severe tissue damage and disfigurement if they are not detected early or are left untreated.
Melanoma follows BCC and SCC as the third most common skin cancer. According to the Centers for Disease Control (CDC), most cases of these types of skin cancer are caused by excessive exposure to ultraviolet (UV) light. UV light is a type of radiation that cannot be seen, but can infiltrate and cause changes to skin cells. Other risk factors for skin cancer include: skin that burns easily, previous history of skin cancer, having blonde or red hair, and having a disease or undergoing treatments that suppress the immune system.4
Primary care physicians (PCPs) could potentially be the first to identify a patient with a possible lesion. However, there are many barriers to routine skin cancer screening in primary care, including, but not limited to, the patient’s time constraints, lack of guidelines, lack of confidence in identifying potentially cancerous lesions, lack of training, inadequate reimbursement for preventative care, and inconsistent public health recommendations for screenings.5
There is no formal recommendation for who should be screened for skin cancer, creating uncertainty amongst PCPs, nurse practitioners, and physician assistants as to who or when to screen. While a total cutaneous exam may be impractical during a yearly visit to a PCP, implementing a brief skin cancer screening during routine audiometric evaluations for all patients is appropriate and feasible. There is significant overlap in at-risk populations for skin cancer and hearing loss.
The incidence of skin cancer, particularly BCC and SCC, increases with age. It has been well documented that men over 50 years of age are at a higher risk for hearing loss and malignant melanoma.6 In addition, the most common sites for skin cancer lesions are on the head, neck, and hands.7 Thus, otoscopy presents an ideal opportunity to more closely observe the patient’s head and neck region.
A study of dermatology referrals found that 56% of referrals were from specialty clinics, such as internal medicine, orthopedics, and hematology.8 The most common reason for referral from specialty clinics included skin rash (27%), skin infections (17%), and eczema/dermatitis (16%).
In order to adopt an interdisciplinary approach, it is important that health professionals outside of dermatology are well trained to provide a thorough skin cancer screening. Swetter et al9 found that PCPs who completed an “INternet curriculum FOR Melanoma Early Detection”(INFORMED) training improved diagnostic accuracy without leading to an increase in dermatology referrals or skin biopsies.
In the Veterans Administration (VA), a Patient Aligned Care Team (PACT) program was introduced in 2010 to provide veterans with a patient-centered, multidisciplinary approach to care focused on prevention of disease and wellness to improve veteran quality of life and satisfaction with their healthcare. The PACT initiative led to the development of the Audiology PACT (APACT) at the James A. Haley VA Hospital in Tampa, Fla, in 2014. It recognizes that older adults with a hearing loss demonstrate a high incidence of co-morbidities, including depression, cognitive decline, and memory impairments, as well as an increased risk for falls and skin lesions. One of the goals of the Audiology PACT is to identify these possible comorbidities and to offer appropriate referral services to elderly veterans.
As part of the APACT initiative, dermatologists from the James A. Haley VA Hospital provided the skin cancer screening training and a sharing agreement with reciprocal referrals. The agreement recognizes the importance of early identification of both hearing loss and skin cancers. The dermatologist also motivated the audiology staff to take a proactive approach in providing skin cancer screenings, as well as referrals, when clinically indicated.
When screening for skin cancer, the ABCDE criteria has been used by many medical professionals to determine if a patient needs a referral to a dermatologist. Figure 1 describes the criteria for skin cancer screening as well as a method for hearing care professionals to adopt when evaluating the skin for suspicious growths.
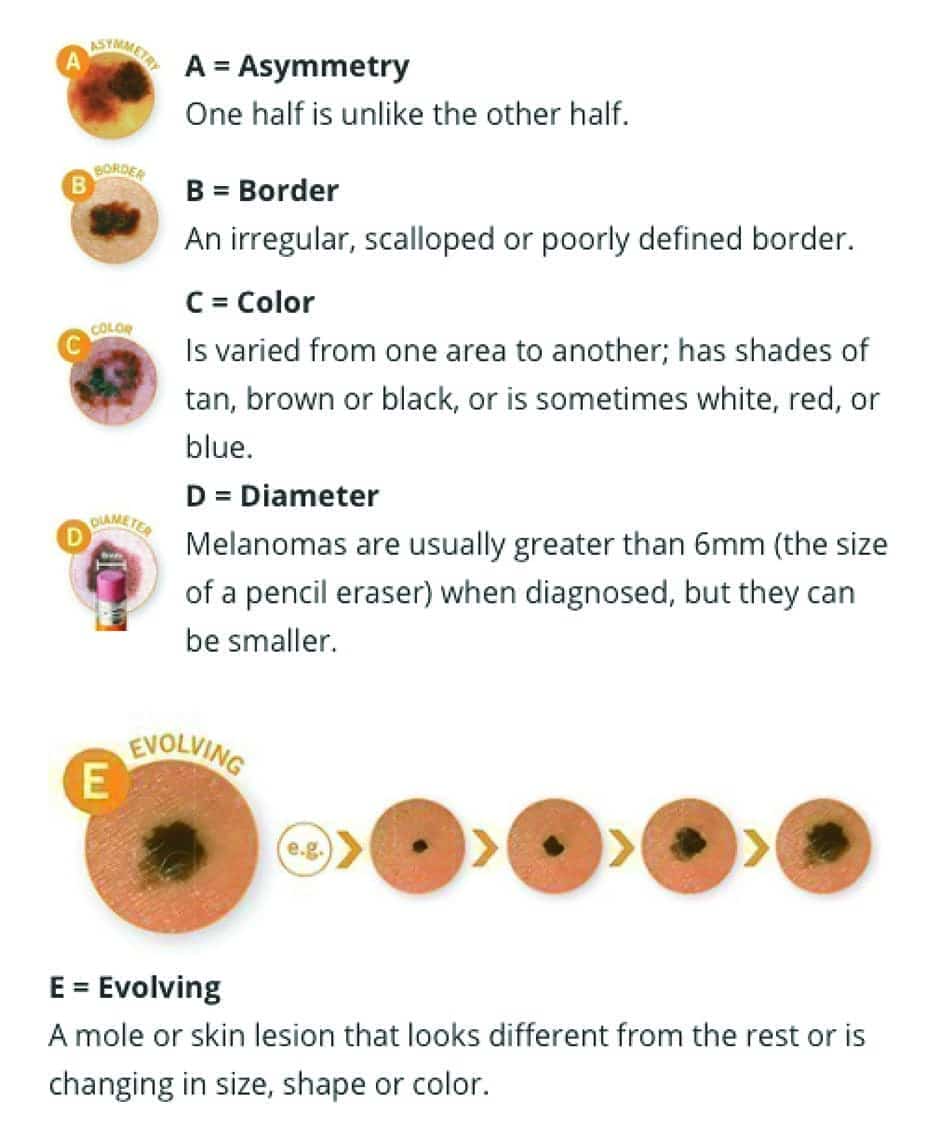
Figure 1. ABCDEs of skin cancer screening. Printed with permission from the American Academy of Dermatology.11
When there is a suspicious growth or mark, the ABCDEs include checking for:
- Asymmetry,
- Border irregularity,
- Color or shade variations,
- Diameter (>6 mm), and
- Evolving growth over time.
The growth in question does not need to meet all of the ABCDE criteria to require a referral; however, the more risk factors, the higher the risk for melanoma.10
In this clinic, audiologists and audiology technicians implement a skin cancer screening of the pinna, head, and face whenever otoscopy is performed. Based on the discussed criteria for skin cancer screenings, the provider may notify the patient of their findings and ask if the patient has been seen by their primary care doctor or a dermatologist for the indicated lesion. The provider would then refer when appropriate.
This brief assessment during otoscopy can have a large impact on the patient, and the audiologist or audiology technician may be the first specialist to identify such lesions. Skin cancer screenings are important because they identify potential risks and can lead to early intervention with the hopes of better outcomes to treatment.
Effective Screening Protocol
In a recent newspaper article from England,12 an audiologist was lauded for identifying a patient’s skin cancer during a routine hearing aid check. The audiologist “spotted a large lump” on the patient’s ear and referred him to his general practitioner (GP). The GP then referred the patient to a dermatologist, who commented that the audiologist’s early intervention led to treatment with radiotherapy instead of having part of his ear removed. The article is one of many that highlight the importance of screenings and the role of the hearing care professional.
With the implementation of the APACT, the audiology staff in this clinic have referred many veterans with suspicious skin lesions. An illustrative case involved a 64-year-old veteran who was seen for an audiological evaluation in 2014. The audiologist noticed a black/brown irregular skin lesion on the left mastoid process that was not obvious to the patient due to its location. A subsequent referral to dermatology resulted in a tele-medicine encounter where images of the lesion were sent to a VA dermatologist and a biopsy was ordered. The lesion tested positive for melanoma and it was excised. The early identification and intervention led to minimal tissue area damage and an overall good outcome. In contrast, experienced hearing care professionals have likely seen patients needing hearing aids who do not have a pinna on which to place the devices as a result of disfiguring skin cancer surgeries (Figure 2).

Figure 2. Example of a skin cancer total resection of the pinna.
Screening protocols, such as the one at the Tampa VA, are not uncommon outside of the United States. A 2015 review by the Kaiser Permanente Center for Health Research revealed that in some countries:
1) Training and developing a referral protocol for non-dermatologists contributed to a 48% reduction in melanoma mortality;
2) There was no physical or psychological harm inflicted to the patients undergoing screenings by non-dermatologists;
3) Specificity for trained professionals was good at 86%.13
In the United States, most PCPs do not have sufficient training in screening to feel confident in their skills and, therefore, screening rates remain quite low.13 Self-detection and opportunistic screenings are the methods of choice.14 Subsequently, on the VA’s informational website, veterans are reminded to ask their doctors about the risk for skin cancer at future appointments.
Hearing care professionals can offer skin cancer screenings by either learning to use the ABCDE method or by simply encouraging patients with suspicious growths in the head area to visit a dermatologist. Additionally, a dermatologist to whom you refer patients may also provide guidance and instruction for you and your staff. Hearing care professionals can also include brochures and handouts in the waiting rooms available for free from the Centers for Disease Control (visit: https://www.cdc.gov/cancer/skin/index.htm).
New technologies are also being introduced to expand screening methods, such as smartphone apps, which have been evaluated in clinical studies and are demonstrating promise. A 2017 study by Thissen et al15 utilizing 108 subjects using smartphone apps reported an outcome of 80% sensitivity and 78% specificity in detecting premalignant conditions. The authors stated, “Although less accurate than the dermatologist’s clinical eye, the app may offer support to other professionals who are less familiar with differentiating between benign and malignant lesions.”15
Given our older adult patient base, hearing care professionals often find themselves on the “front lines” for the diseases and disorders that are more prevalent in this population. While we should be careful never to “diagnose,” the hearing care clinician can play an important role in recommending a patient for medical referral and/or to see a dermatologist for a suspect mole or skin lesion.
Correspondence can be addressed to can be addressed to HR or: [email protected]
Original citation for this article: Armero O, Glick I, Harris K, Hicks C, Hinton A. A skin cancer screening model for hearing care professionals. Hearing Review. 2018;25(2):12-14.

Biography: Oscar Armero, AuD, and Ilana Glick, AuD, are Clinical Audiologists, and Kelsey Harris, Charissa Hicks, and Ashley Hinton are doctoral audiology residents at the James A. Haley Veterans’ Administration Hospital in Tampa, Fla.
References
-
Skin Cancer Foundation. What is skin cancer? 2018. Available at: https://www.skincancer.org/skin-cancer-information
-
Altman JF, Oliveria SA, Christos PJ, Halpern AC. A survey of skin cancer screening in the primary care setting: a comparison with other cancer screenings. Arch Fam Med. 2000;9(10)[Nov-Dec]:1022-1027.
-
Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the US population, 2012. JAMA Dermatol. 2015;151(10)[October]:1081-1086.
-
American Cancer Society. Risk factors for melanoma skin cancer. May 20, 2016. Available at: https://www.cancer.org/cancer/melanoma-skin-cancer/causes-risks-prevention/risk-factors.html
-
Loescher LJ, Harris Jr JM, Curiel-Lewandrowski C. A systematic review of advanced practice nurses’ skin cancer assessment barriers, skin lesion recognition skills, and skin cancer training activities. J Am Acad Nurse Pract. 2011;23(12)[December]:667-673
-
Heckman CJ, Darlow S, Manne SL, Kashy DA, Munshi T. Correspondence and correlates of couples’ skin cancer screening. JAMA Dermatol. 2013;149(7):825-830.
-
Buettner PG, Raasch BA. Incidence rates of skin cancer in Townsville, Australia. Int J Cancer. 1998;78(5)[November 23]:587-593.
-
Chowdhury SN, Podder I, Saha A, Bandyopadhyay D. Interdepartmental dermatology: Characteristics and impact of dermatology inpatient referrals at a teaching hospital in Eastern India. Indian J Dermatol. 2017;62(1):29-32.
-
Swetter SM, Chang J, Shaub AR, Weinstock MA, Lewis ET, Asch SM. Primary care-based skin cancer screening in a veterans affairs health care system. JAMA Dermatol. 2017;153(8):797-801.
-
Tsao H, Begolka WS. Reply to: “Time to move forward after the report of the AAD Task Force for the ABCDEs of Melanoma.” J Am Acad Dermatol. 2015;73(4)[October]:e151.
-
American Academy of Dermatology. What to look for: ABCDEs of melanoma. Available at: https://www.aad.org/public/spot-skin-cancer/learn-about-skin-cancer/detect/what-to-look-for
-
Lynch L. ‘I went for a hearing aid check and found I had cancer’– Styvechale man reveals how life was saved by routine check. Coventry Telegraph. May 14, 2017. https://www.coventrytelegraph.net/news/i-went-hearing-aid-check-13025678
-
Wernli KJ, Henrikson NB, Morrison CC, Nguyen M, Pocobelli G, Blasi PR. Screening for skin cancer in adults: Updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2016;316(4):436-447.
-
Robinson JK, Halpern AC. Cost-effective melanoma screening. JAMA Dermatol. 2016;152(1)[January]:19-21.
-
Thissen M, Udrea A, Hacking M, von Braunmuehl T, Ruzicka T. MHealth App for risk assessment of pigmented and nonpigmented skin lesions – A study on sensitivity and specificity in detecting malignancy. Telemedicine and e-Health. 2017;23(12):948-954.



