
Research | February 2002 Hearing Review
By Karl Strom, editor
Mention Boys Town to most people and their minds instantly conjure up movie images of Spencer Tracy in his Oscar-winning role as the lovable Father Flanagan, the founder of the home for wayward boys. But mention Boys Town to someone in the hearing care field and they immediately think of pediatric audiology and genetic research.
And with good reason. Established in Omaha in 1972 and officially opened in 1977, this year marks Boys Town National Research Hospital’s (BTNRH) 25th anniversary of research into childhood hearing loss.
The hospital and research facility sees approximately 30,000 children each year.
In the last quarter-century, BTNRH has been at the forefront of auditory research, most notably in the use of otoacoustic emissions (OAEs) and auditory brainstem responses (ABRs) for clinical diagnostics and infant hearing screening, the application of pediatric amplification, the identification and treatment of syndromic hearing losses, and the mapping of the efferent auditory system. Starting from a vacant lot in 1972, BTNRH has grown into a 164,000-sq-ft. six-floor building adjoining St. Joseph Hospital on the campus of Creighton Univ. (near downtown Omaha). The hospital staff includes about 500 employees and sees approximately 30,000 children a year.
“One of the things we’ve attempted to do at BTNRH,” says Founding Director Patrick Brookhouser, MD, “is to bring in what I call clinician researchers—individuals who truly have a foot on both sides of the [clinical and research] fence and who are seeing patients and taking care of families at the same time they’re conducting research. These are scientists who bring their experiences from the clinic into the laboratory very rapidly. Often you’ll have a facility where the clinic and research laboratory are totally separated from each other—sometimes even in another building—and therefore the researchers don’t experience the same kind of pressure that can often arise from a clinical problem.”
The emotional impact of seeing how a family can struggle with a child’s hearing loss is important, according to Brookhouser. “Many researchers have the freedom of thinking, ‘Well, whenever I solve the problem, that’s when it will be solved,’ whereas a family that you see today with a young deaf child has many very real, immediate problems that they’re looking for answers to. So a certain urgency on a personal level enters into the scientific research here.”
Director of Research Walt Jesteadt, PhD, who is a founding member of the research staff, adds that the emphasis on pediatrics and developmental issues makes Boys Town fairly unique. “In actuality, I think we share many of the same characteristics of the House Ear Institute (HEI) and Central Institute for the Deaf (CID) which have also been recently featured in The Hearing Review (see Jan. and Nov. 2001 issues). However, we’re a little different because I think we’re slightly more self-contained. Unlike CID, we have an otolaryngology program, and unlike HEI, our clinical program shares the same facility as the research center.”
Research at Boys Town continues to expand with new scientists and a wider breadth of studies. “We’ve moved into new areas of research like genetics,” says Brookhouser,“while continuing to fill the information gaps for audiologists and service providers across the country relative to dealing with young children—especially in the area of newborn hearing screening.
“Additionally, I think for the first time, our field is actively seeking some kind of medical or pharmaceutical intervention for the inner ear, apart from a cochlear implant. The potential that has come from our 20 years of study in genetics is very exciting.” He points to the opening of the National Center for the Treatment of Usher Syndrome at Boys Town as one example.
Recognizing the potential hearing-related applications of existing products developed by software and technology firms, Boys Town is also in the process of establishing a Learning and Technology Center for Childhood Deafness and Vision Disorders. One of the goals of this center, says Brookhouser, is to provide something akin to telemedicine for the educational aspects of young children and their parents. In particular, the center would like to use the Internet to provide rural families with the same level of rehabilitative care that can be obtained in larger population centers.
Organization of the Research
Research at BTNRH is overseen by Brookhouser and Jesteadt, and the work is loosely divided into five areas: the Center for Audiology and Vestibular Services which is directed by Patricia Stelmachowicz, PhD; the Clinical Sensory Physiology Laboratory directed by Michael Gorga, PhD; the Center for Hereditary Communication Disorders directed by William Kimberling, PhD, and the Center for Hearing Research directed by Jesteadt. Additionally, the Center for Childhood Deafness is directed by Mary Pat Moeller, MS, which includes speech and language services and speech physiology, headed by Maureen Higgins, PhD, and the cochlear implant program, for which Lee Harker, MD, serves as neuro-otologist.
“One of the great qualities and distinguishing features about Boys Town is that we have very close ties between clinicians and basic scientists,” says Stelmachowicz. “As clinicians, we’re always trying to interest the basic scientists in our clinical concerns so we can gain new solutions and insights into our work. When we have some unique cases, we’re able to talk with experts in a number of disciplines. For example, Douglas Keefe, PhD, is an acoustic physicist and middle ear researcher here who has provided invaluable support on many of our projects.”
Brookhouser agrees that this type of interaction pays off on many different levels: “When the basic researcher is constantly being confronted by a clinician who is saying, ‘I just saw a strange case in which a child’s tests produced a number of unexplained results. How can that be?’ All of a sudden, that researcher has to go back to square-one and re-examine how a particular clinical manifestation occurs—even if it doesn’t seem to make sense from a theoretical standpoint. That’s a constant reality-testing experience, and it’s very conducive to good science.”
“I tell people that we have a fairly small hospital but a gigantic department,” says Gorga. “We have brilliant scientists all under one roof, who all talk to each other—and they even seem to enjoy talking to clinicians like me,” he says smiling. “As a consequence, my program has been pushed forward, and I think our clinical research consistently stands up to critical scientific review because we are surrounded by so many good scientists.” Almost all the research at BTNRH is funded by grants from the National Institutes of Health (NIH).
The following is an update on a few of the research activities at Boys Town, and is intended only as a sampling of the projects being undertaken. Many other distinguished scientists and clinicians are involved in important work at BTNRH whose work could not be covered here due to space restrictions.
Clinical and Behavioral Research
Optimizing amplification for infants and young children: The development and validation of techniques for selecting and fitting advanced hearing instruments for infants and young children is the focus of research being conducted by Stelmachowicz and Moeller. They have obtained an NIH grant which, in part, is designed to discover if there are specific differences in amplification needs between children and adults who have hearing loss, and to identify amplification goals for pediatric fittings.
The investigators’ position that children may require increased high and/or low frequency gain compared to adults has placed Boys Town on the cutting edge of a controversial debate in pediatric audiology. “There are camps of divergent opinions on the issue of high frequency audibility,” says Stelmachowicz. “And, in practice, adult data are often extrapolated to apply to children. With an adult, we know that we can cut out a lot of the high frequencies in meaningful speech, and they will essentially fill in the gaps…With children who have not fully acquired speech and language understanding, our theory is that the reduction of high-frequency signals will have a larger negative impact. And that’s what we found and published in a recent study in Journal of the Acoustical Society of America.”
She points out, for example, that the /s/ sound of an average female speaker can be at 9 kHz, and few hearing instruments come close to amplifying that frequency region. If it can be shown that it makes sense to provide audibility in this high frequency range, then manufacturers may have something more to work toward. “There are obviously a lot of different issues related to complex signal processing in non-linear circuits,” says Stelmachowicz. “The main question we’re interested in is, Do we see adult-child differences? If we do, then we should think about different, or at least altered, amplification rationales for children.”
“We’re now branching out from that study and trying to look at some specifics,” she says. “For example, most hearing aids cut out a lot of the low frequencies, and that strategy is based on good audiological reasoning that relates to the upward spread of masking. However, we also know that a lot of speech information and the quality of sound can be greatly diminished when the low frequencies are reduced. There is also some evidence that, when we cut out the low frequencies, kids who are trying to monitor their own voice may respond in negative ways. So the study is trying to answer some basic questions that could ultimately be used by the hearing industry to design better hearing aids for children.”
|
Facts on Boys Town
|
The second part of the study involves children’s use of multiple acoustic cues and the acclimatization process, with the hope of finding the best approach for subsequent hearing instrument fittings for children. Stelmachowicz and colleagues are trying to ascertain, for example, whether children who are previous users of hearing instruments should be re-fit in the same manner as adults. They are also trying to determine how long it takes to know if the new instrument is an improvement over the old one.
Longitudinal study of speech and language development: The third part of the above grant is a five-year longitudinal study being conducted by Mary Pat Moeller, Pat Stelmachowicz and colleagues. The study compares normal-hearing babies with early-identified hard-of-hearing babies and late-identified babies (identified at 18 months or later). The goal is to examine the effect of audibility on specific aspects of speech and language learning. Moeller and her colleagues are following babies and tracking early speech development, mother-child interactions, and other factors that might be impacted by reduced audibility.
“We’re particularly interested in identifying early markers of success with amplification or markers that indicate a need for adjusting the amplification,” says Moeller. “A good example is a little girl we saw who had a moderate hearing loss. At about 16 months of age, her speech was extremely hypernasal. After ruling out a number of physical anomalies, we discovered that her hearing aid was not giving her enough audibility in the low frequencies to make the oral-nasal distinction. When we made an adjustment to her amplification, her nasality almost disappeared. That’s an example of what we’re looking for; we’re trying to understand if there are some developmental landmarks that signal the need for increased audibility, or that indicate the fitting is successful.” The study also seeks to understand if early-identified (and amplified) babies keep the same rate of language development as those babies with normal hearing.
Optimal approaches in speech therapy: Maureen Higgins, PhD, a speech physiologist, is the primary investigator of an NIDCD grant designed to analyze speech development and therapy strategies for children who have cochlear implants. Higgins and her colleagues are studying the speech movements of these children to learn how the additional auditory input and corresponding feedback provided by the devices influence speech production development. They are also examining ways that therapy approaches can be modified to achieve optimal speech production outcomes and are comparing efficacy data for different treatment strategies. Higgins says this type of data is lacking at the present time and could have important ramifications for clinical practices.
Information dissemination: The Center for Childhood Deafness has produced literature and videos designed to help educate hearing-impaired children and/or their parents. The Center also recently launched a comprehensive website at www.babyhearing.org designed for those parents whose babies have failed a newborn hearing screening test.
Research in Human Sensory Physiology
OAEs and ABRs: One of the best known contributions that Boys Town has made to the audiological field relates to its research on OAEs and ABRs. Today, most distortion product otoacoustic emissions (DPOAEs) instrumentation incorporate a template, developed by Michael Gorga and colleagues, that helps interpret DPOAEs in the clinic. Similarly, with regard to ABRs, many clinics throughout the world are using normative data developed at Boys Town for ABR latencies in neonates and young children. Additionally, the use of tone-burst ABRs has been given a big boost by the information generated by Gorga and BTNRH clinicians.
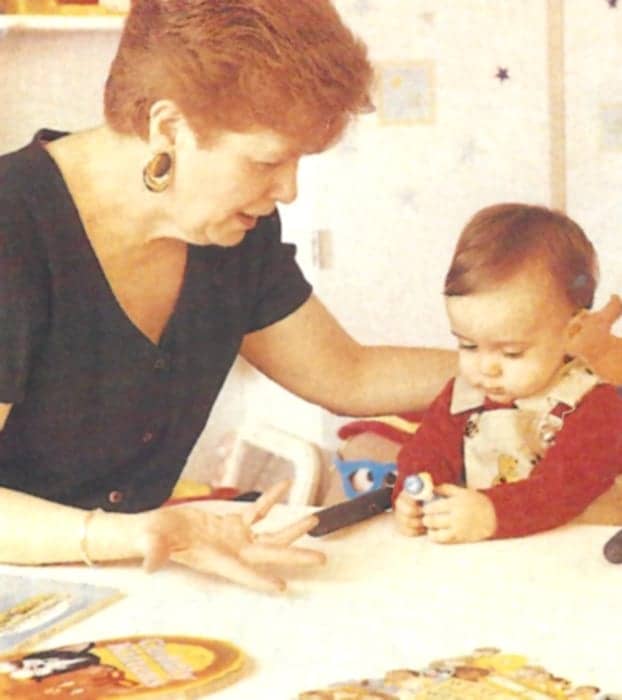
Mary Pat Moeller, MS, is conducting a five-year longitudinal study to examine aspects of audibility on speech and language acquisition in infants and children.
“Part of our mission is not just to serve the patients we see at our hospital but also to disseminate information so other clinicians can do a better job at serving their patients,” says Gorga. “We were pleased that manufacturers picked up on the concepts that we published in a 1997 paper in Ear and Hearing.” In that paper, Gorga, staff scientist Stephen Neely, DSc, and colleagues presented a large-scale study of DPOAEs for normal-hearing and hearing-impaired ears, and helped develop an approach for interpreting these measurements.
Future OAE Research: Current research in the Clinical Sensory Physiology Laboratory focuses on using DPOAEs to understand suprathresholds in hearing-impaired individuals. Ultimately, the laboratory hopes to provide a reasonably quick measure of response growth that can then be related to loudness recruitment. With this information, future clinicians may be able to set the output limitations of hearing instruments with greater confidence.
When asked about where he thinks the future of OAE and ABR research will lead, Gorga says that these measurements probably do have a finite amount of information that they can provide. However, he believes that future research will yield new data about the interaction between the peripheral and higher-level central auditory functions. “I think that we’re going to start examining more closely the interactions between the brain and the impaired ear,” says Gorga. “For example, some children when given a cochlear implant do remarkably well. But not all children do. What you want to know is why—given the same signal and seemingly identical conditions—one child does fantastic while another child doesn’t do well at all. Obviously, one child is able to extract optimal levels of information from the signal while the other child is not. If we could better understand this process, perhaps we could make some device changes or make rehabilitative adjustments to help optimize the child’s hearing…I think there will eventually be a lot more research on the synergy between peripheral and central processing that leads to new rehabilitative schemes.”
Auditory neuropathy: Gorga says there is little question that there are varying degrees of severity in auditory neuropathy (c.f., auditory dysynchrony) and, in the genetic-related forms of the disorder, he says the patients may have more homogenous types of auditory problems.
“Auditory neuropathy can be a very difficult disorder to understand, partially because our measurements in humans are necessarily all indirect,” says Gorga. “On what is the diagnosis of auditory neuropathy based? It’s based on very abnormal ABRs with OAEs present, with or without hearing loss, poor speech reception, and absent acoustic reflexes. Well, it would be theoretically possible to make lesions in a whole slew of places along the entire auditory pathway that could yield these effects…But, depending upon where that lesion is, you can expect to get very different results from the rehabilitative intervention [e.g., a cochlear implant versus a hearing aid]. For example, if the lesion is at the inner hair cell and the nerve fibers are completely intact, then a person might do well with a cochlear implant. However, now let’s imagine severing the 8th nerve; in this case, the cochlear implant is going to be less effective. On the other hand, if it is a dysynchrony-type problem that resembles demyelination [i.e., the nerve can’t keep a sharp temporal sequence], a stimulus provided by a cochlear implant may be able to overcome that problem.”
Visual reinforced audiometry is one of several tools used for assessing the hearing health of infants.
Although this suggests an increasingly complicated future for treating the different hearing loss pathologies, Gorga is exuberant about the new tools and diagnostic technologies that are surfacing: “Just think back on the last 20 years about how many kids you fit with amplification and, at the beginning of the fitting you thought, ‘Boy, I’m going to really help this kid.’ Then, lo and behold, some of those kids didn’t do nearly as well as you would have predicted given their hearing loss and the device that was provided to them. Well, I sit back and shudder sometimes at the thought of fitting a hearing aid on a child who had auditory neuropathy…At least today, when we combine our measurements with OAE and ABR data, we can detect if we’re dealing with a child with some special disorders. Maybe the rehabilitation aspect is still fairly complicated, but we’re certainly in a much better position to counsel the family about reasonable expectations. And instead of fitting a hearing aid—which is designed to fix a part of the hearing system that doesn’t have much to do with part that is broken in the case of auditory neuropathy—we can instead get a better idea of what the best rehabilitative plan might be for these kids.”
Hereditary Communications Disorders Research
Consisting of 30 people, including 10 PhDs and 1 MD, the Center for Hereditary Communications Disorders is studying genetic hearing loss, including Usher syndrome, Alport syndrome, Branchio-oto-renal (BOR) syndrome, auditory neuropathy, and several other disorders.
Usher and Alport syndromes: Usher syndrome is a recessive genetic disorder which combines hearing loss of varying degrees with a gradual loss of vision through retinitis pigmentosa. It is the leading cause of blindness in the developed world, and is the cause of about 50% of all deaf/blind cases.
William Kimberling and colleagues have a remarkable track record in discovering and characterizing several of the Usher-related genes. The Center has become internationally known for its expertise in Usher syndrome, and has access to more than 1300 families worldwide who carry the genes for the syndrome. In 1989, the lab was the first to identify the location of the Usher Type 2A gene, and in the mid-90s they (along with researchers at the Pasteur Institute in France) discovered the Myosin 7A gene which is responsible for Usher Type 1. The Usher 2 gene was discovered by BTNRH shortly thereafter and the lab actually earned the right to name the protein associated with the gene (they named it Usherin).
“[Usherin] is part of the basement membrane in the eye and the ear,” says Kimberling. “And that was a tremendously lucky happenstance for us, because Dominic Cosgrove, PhD, was here researching Alport syndrome which is also a basement membrane disease. He came up with a hypothesis on how we might be able to decrease the severity of Alport syndrome. And it looks very much like something that might work. Drug companies are currently interested in this development.”
Clinical audiologist Jodi Winfrey conducts newborn hearing screening using otoacoustic emissions.
“The interesting thing [about Cosgrove’s observation] is that it looks like Usher Type 2 might go through the same pathological pathway, so we’re able to use the same logic, the same materials [competing antibodies], and we may even be able to stop the progression of the retinitis pigmentosa in Usher 2. We’re currently working on testing this hypothesis and hoping that within two years we will be talking with the FDA about setting up clinical trials.”
While Kimberling says that his team initially expected gene therapy to be a key component in treating Usher syndrome and other genetic disorders, he now believes that conventional therapies may ultimately prove to be more useful. “Gene therapy has turned out to be a tough nut to crack,’ he says. “The surprising thing is that, in many cases, simpler approaches are effective in, at least, mitigating the impact of these genes. For example, Vitamin A in certain forms of Usher syndrome is effective in slowing down the progression of retinitis pigmentosa.” He believes that other forms of recessive hearing loss —even though the conditions are called “congenital deafness”—are rarely developmental in nature; rather, they take the form of degenerative diseases.
And the difference between a degenerative and developmental disease, according to Kimberling, is much like the difference between being able to patch a wall in your basement, as opposed to finding out that the entire foundation of your house is bad. “With any disease that is degenerative, there is at least some hope of interfering with that degeneration,” he says. “Even with Connexin 26 [hearing-related] diseases, there may be a way to delay the progression of the hearing loss. The fortunate thing about being involved in Usher syndrome research is that we rub elbows with the vision scientists…and that’s making us consider other options. We’re also starting to look at problems like hair cell rescue…For example, there is a type of Usher syndrome that appears to be a good candidate for preventing the hearing loss aspect of the disorder via dietary factors.”
Hearing science still doesn’t have a good idea about how many hearing losses are truly congenital, says Dr. Brookhouser: “It is still not well understood how many children are born with hearing loss, versus how many are being born with relatively normal hearing and then having it deteriorate over a period of months or years.” he says. “And, if we find out the latter occurs more frequently, that raises the possibility of preventing the onset of these hearing losses. If the child is born with a hearing loss, then you’re obviously concerned with treating it in some way. But I think we’re going to eventually find that a number of these losses are, in fact, progressive over time and they may lend themselves to some kind of intervention.”
The advances made at the Center for Hereditary Communications Disorders has prompted the creation of a new BTNRH facility, the National Center for the Treatment of Usher Syndrome, that will include three new laboratories designed to contribute knowledge about the vision aspects of Usher syndrome.
Genetic aspects of auditory neuropathy: Philip Kelley, PhD, is studying nonsyndromic recessive hearing losses and has recently become interested in auditory neuropathy. “We have evidence now that auditory neuropathy might be a lot more common in some forms.” says Kimberling. “It’s a genetic disorder, it’s recessive, it’s inherited, and it’s not usually associated with other central problems.”
He explains that, while auditory neuropathy may be a defect of the inner hair cells, it may also be due to a defect in the communication between the inner hair cell and spiral ganglion. This might help explain the mixed results in treating auditory neuropathy (or dysynchrony) with cochlear implants (also see Gorga’s previous remarks). “The mixed results are understandable,” he says, “because we have some auditory neuropathies that do involve the inner hair cells while the spiral ganglia are perfectly fine; these types of auditory neuropathies will respond to a cochlear implant. But the ones involving the spiral ganglion and the 8th nerve itself—and we have a family with this type of problem—obviously would not respond well to a cochlear implant. So it’s clear that differential diagnosis early on is very important in this disorder.”
The research team at BTNRH has located the gene for auditory neuropathy and plans to publish its findings in the near future.
Neurobiological Research
The research conducted in the Center for Hearing Research has a strong emphasis on developmental biology and the efferent system, much of which reflects the work that W. Bruce Warr, PhD, has been doing at BTNRH since 1978. Warr has become one of the leading anatomists of the olivocochlear system. More recently, Warr and colleagues have published papers on fluorescent labeling of olivocochlear neurons in chinchillas, cochlear root neurons in rats, and postnatal development of the efferent synapses in rat cochlea.
Similarly, Edward Walsh, PhD, is researching how the auditory system develops in mice that have a genetic hypothyroid disorder, with the low thyroid function leading to hearing loss. “Although this is a genetic disorder,” says Jesteadt, “[Walsh] has been able to basically correct for the deficiency with drug treatments to the mothers during pregnancy, or the newly born mice, and he’s even used other drugs to artificially produce the deficiency. So we have a pretty good handle on what the system is doing in terms of actual control mechanisms. This gives us a model for a naturally occurring problem in efferent system development.”
Walsh’s developmental physiology laboratory has recently teamed up with the neurochemistry laboratory of Barbara Morely, PhD, to examine a knock-out mouse model that lacks acetylcholine esterase. This chemical is responsible for clearing out acetylcholine [the neurotransmitter in the efferent auditory system responsible for the firings between synapses]. Morely’s laboratory has produced a large body of work in recent years on the role of neurotransmitters in the transduction process of auditory function.
Jesteadt’s own work deals with the perceptual impact of nonlinearity in the auditory system, particularly relative to masking and loudness growth. He is also interested in models of sensorineural hearing loss and how to simulate hearing loss, which is something many people have tried to do in order to give parents and teachers a better idea of what hearing-impaired children are coping with. Additionally, Jesteadt and Keefe are conducting studies that compare OAEs with behavioral data.
The most recent person to join the BTNRH neurobiology group is David He, PhD, who came from Peter Dallos’ lab at Northwestern where he was involved in identifying the gene related to outer hair cell motility. It is hoped that his research will ultimately yield better models for congenital hearing loss and shed more light on the developmental aspects of cochlear function.
Similarly, Stephen Neely, DSc, is interested in the cochlear mechanics, and was one of the first to develop models that described non-linearities related to OAEs. For example, Neely, Warr and Gorga were the first to show that stimulating one ear can produce an effect on OAEs in the opposite ear. “It’s a different way of looking at the physiological value of binaural hearing and demonstrates that the wiring of the efferent system is directly involved in the mechanisms underlying OAEs,” says Jesteadt.
“Those types of things happen here often,” he adds. “Someone says ‘Well, the auditory system should work this way,’ then they walk down the hallway and find someone who knows a little bit more about another part of the system, and they eventually discover some new concept. That’s one of the things that’s really fun about Boys Town.”
“Having scientists in both the clinic and in the laboratory has been very important,” says Dr. Brookhouser. “They’ve also involved many of their MA-level clinicians in the research, as well, so there is an interaction that ends up benefiting everyone. As these clinicians are seeing patients, they’re also involved in the development of research projects which are important for the advancement of knowledge in their fields.”
“The mind-set of clinicians here is that they are constantly learning,” says Stelmachowicz. “We have some clinicians that have been working at BTNRH for over 20 years, and they are so energetic and integral to the research that is accomplished.” She says many clinicians do smaller, independent research studies that often prove to be extremely important for answering clinical questions. “For example, some of the FM studies that Dawna Lewis, MA, has been involved with have addressed important questions about classroom amplification. We’ve also done earmold acoustic studies in children, modification of the APHAB to suit children, and pursued many other ideas. I think that one of the reasons we have such a stable staff is that everyone is provided with an opportunity to find their own niche…This, in turn, helps everyone understand the value of the basic research being performed here.”
“We encourage collaboration,” says Jesteadt, “and there’s no real good reason to come to a center like this if you’re not the kind who likes to interact with other clinicians and researchers in neighboring disciplines.”
Gorga agrees and stresses the need to embrace the role of the clinician-researcher for all hearing care professionals. “Those of us who treat hearing loss cannot continue to serve our patients without becoming familiar with the concepts—at least on a rudimentary level—of the molecular geneticists and biologists. Our disciplines are all going to continue to interact and grow closer together…Audiologists are in a unique position, because we are on the front lines serving patients, and that’s where we bring our expertise of patient care to the table. In order to do this at the highest level, we need to interact with and to understand the work being done by basic scientists. In particular, audiologists at Boys Town are afforded a very unique opportunity. If you were hired at Boys Town and then proceeded to lock yourself in your office, do your job, and not interact with anyone, nobody here would yell at you, but you certainly would be a fool.”
|
Sleuthing the Human Genome So how do scientists find the gene that is responsible for a particular syndrome or hearing-related disorder? The initial process of zeroing in on the “guilty” gene (and/or protein) is to collect genealogical information from families with that inheritable disorder and then use gene mapping techniques to find the approximate location of the gene. “By locating that gene on a particular chromosome,” says William Kimberling, PhD, “we can then go back to the genome data base [from the Human Genome Project] and look for the candidate genes—those genes that might be related to the disorder. Depending on how big that region is, it could be 3-4 genes, or 30-40, or a couple hundred.” At this point, the geneticists start looking at the candidate genes in a systematic way to find a mutation (or change) that could inactivate that gene. “Once you find the actual mutation, you have an indication that there is some correspondence between the gene and the disease,” says Kimberling. “For example, the gene for a specific form of myosin, called Myosin 7A, was known for several years, although its function wasn’t fully appreciated. Then Boys Town and a group in France discovered that mutations in that Myosin 7A gene caused the severe form of Usher syndrome. Well, suddenly, in a way of speaking, this finding revealed ‘the gene’ for Usher syndrome [or Myosin 7A], which is now referred to as the ‘Usher gene.’ So that’s basically the first step. You need to get to the stage where you can say, ‘Here is the gene, and when that gene codes for a particular protein, or when that gene isn’t activated and the protein isn’t produced, we’ll see [in the case of Usher syndrome] a hearing impairment or hearing impairment with retinitis pigmentosa.’ The whole process is usually very lengthy, with the time-frame depending on how lucky you are in choosing the right candidate gene.” Once the gene is pinpointed, says Kimberling, the research becomes more exciting, because scientists then have the ability to use many different tools, such as knock-out mice, to learn more about the disorder. Additionally, the researchers can start screening large populations of patients, provide a precise diagnosis, and find families who have different forms of the mutation. Additionally, antibodies for the protein might be made. “All of a sudden,” says Kimberling, “because you can identify the protein and the gene, there is an explosion of questions and hypotheses that arise by knowing their basic functions.” Ultimately, this provides important ideas on how to treat, prevent and/or retard the progression of the disease or disorder. |
Acknowledgements
‘The Hearing Review thanks the Boys Town staff members who took time out of their busy schedules to be interviewed for this article. We also extend a special thanks to Patricia Stelmachowicz, PhD, and Marsha Johns.