Patient Care | January 2020 Hearing Review
By Michael A. Harvey, PhD, ABPP, and David Citron, PhD
What The Fiddler on the Roof can teach us about a needed change in patient counseling
Too many hearing care professionals have a resistant or ambivalent outlook about the use of motivational engagement tools which seek to change patients’ attitudes about their hearing loss. As the fiddler Tevye can tell you, change can be good—and even necessary—for all parties involved.
An incredulous audiologist asked, “Why on earth wouldn’t patients with hearing loss use hearing aids when they know it would benefit them?”
“Why on earth wouldn’t some audiologists use motivational engagement strategies when they know it would benefit them?” I, too, asked incredulously.
“You mean when it would benefit the patient, right?” the audiologist asked.
“You’re half right,” I responded, doing my best to remain incredulous. “Although motivational engagement strategies would clearly benefit your patients, it would also benefit you!”
This imaginary dialogue was precipitated by the second author (DC) while conducting a workshop for private practice audiologists on Motivational Interviewing (MI). It went well. All the participants enthusiastically endorsed the importance of learning these new skills, integrating them into their practice, and were looking forward to individualized follow-up that was offered at no cost. So far so good. However, none of the participants took advantage of further coaching and integration of any MI tools despite repeated offerings.
Motivating our patients can be mind-boggling, even intimidating, including for psychotherapists (like first author MAH) whose education, unlike many AuD programs, emphasizes the art and science of motivating people to change. This became crystal clear when I decided to build an outdoor patio. I’m not at all handy, but I researched different sizes and styles of pavers, leveling techniques, etc, and confidently estimated when it would be completed. The patio algorithm gave me great comfort and security: if I worked on it for 2 hours per day, I would make 2 hours of progress per day, and be finished in a very predictable time period. A done deal. Not so with my patients in psychotherapy. How many psychologists does it take to change a light bulb? Answer: Just one, as long as the light bulb wants to change. In contrast, pavers don’t have to be motivated to become a patio.
A version of patio pavers is the medical model. Although that model certainly endorses motivational engagement with patients (aka “bedside manner”), its emphasis is that if you render the proper diagnosis and prescribe the proper treatment, you will have a successful outcome. A done deal. That algorithm gives one (the doctor at least) great comfort and security, like how I felt when I built the patio.
Some healthcare professionals, including audiologists, may overly adhere to the medical model to the point of shunning personal adjustment counseling. A common rationalization is maintaining professional boundaries by not going beyond one’s scope of practice. In contrast, however, this convention can be viewed as an unhelpful constriction of those boundaries. Although it is clearly unethical for non-therapists to practice psychotherapy, this caveat can be misinterpreted to mean that you should not elicit and discuss patients’ feelings. In the words of surgeon Atul Gawande:
“The mistake clinicians make is that they see their task as just supplying cognitive information—hard, cold facts and descriptions. They want to be Dr Informative.” 1
Similarly, Clark and English2 noted that some audiologists continue to feel more confident in the provision of patient education or content counseling than addressing the psychosocial aspects of personal adjustment counseling so important to hearing rehabilitation.
For example, one audiologist (we’ll call him Dr Smith) acknowledged that MI could benefit his patients, but observed that “It’s cumbersome.” I (author MAH) responded with something like, “Yeah, it’s a new skill but it gets easier with practice.” In my imaginary continuing dialogue with Dr Smith, I would elaborate my response as follows:
“Yes, you’re right. It will benefit your patients, as there’s a ton of research indicating that using MI improves treatment outcomes with a variety of health problems.3-5 And I also agree with you that learning MI is cumbersome because there are a lot of skills to remember and practice.”
He would nod his head smugly.
“But I’m a bit confused though,” I would continue. “Please help me understand something. You’ve spent a lot of time and effort building your practice, keeping up with all the latest research and technology, training your staff, attending to some very fine details in patient care . . . [long list]. You’re dedicated to your patients and take a lot of time to try to connect with them. You make this a priority. Surely, you’re no stranger to mastering cumbersome challenges! So why wouldn’t you use additional motivational engagement tools when you know they would benefit your practice and increase patient loyalty, and also your financial bottom line?”
“You psychologists love this stuff, I can tell, but it’s not my cup of tea. It doesn’t come naturally to normal people,” he might respond.
It’s true that psychologists are seldom satisfied with so-called “surface responses;” there must be “deeper” reasons for almost everything. There’s a joke about two shrinks passing each other in the hallway. The first says to the second, “Hello!” The second smiles back nervously and mumbles, “God, I wonder what that was all about?”
I return to Dr Smith and my $64,000 question: “Why wouldn’t you try ‘different cups of tea ’ that have been shown to improve quality of life for your patients and yourself?”
“You’re the psychologist, you figure it out. Then you can write an article about it.”
“Good idea. Maybe I will.”
Feeling Like a Fiddler on the Roof
Just as there is no personality type for the unmotivated patient, there is no personality type for “Dr Informative” healthcare providers. Rather, this avoidance can be understood in the context of how one copes with the numerable imposed stresses by the current health-care system: EMR, insurance company denials, online reviews, entitled patients, less-than-collegial colleagues, declining reimbursement, increasing regulation, increasing documentation requirements, and so on. Stated differently, it may be easier to venture into unfamiliar emotional territory when not simultaneously deluged by all these external pressures. By necessity, one’s tenuous struggle to remain balanced takes priority.
We’re reminded of the Broadway musical Fiddler on the Roof. It portrays the villagers of Anatevka set in 1905 at the Pale of Settlement in Imperial Russia. The villagers are struggling to continue their traditions—remain balanced—and keep their society running in a precarious often-dangerous world. The fiddler represents the traditions with which Tevye, the narrator and main character, is desperately trying to “scratch out a pleasant simple tune without breaking his neck.” I imagine that the fiddler made sure to play the same tune over and over again in the same well-defined, standardized manner with the same tempo and in the same key—all in the service of providing Tevye and the villagers with dependable comfort and security. Any deviation or improvisation from the routine would surely cause fear and anxiety against the backdrop of their anything but routine, scary world.
Tradition = safety
Tradition is to Tevye as the medical model is to those practitioners holding on for dear life to stay balanced in today’s tumultuous healthcare system. The medical model, with its well-defined, standardized diagnostic and prescriptive protocols, instrumentation, audiograms, programming modules, etc, provides a blueprint of what to do and when to do it. It serves as psychological armor—protection from the inherent anxiety and uncertainty of what one audiologist described as “messy emotional abreactions of patients.” Building a patio was a good respite from these abreactions; everything became so clear, much less “messy.”
All people, including healthcare professionals, tend to remain loyal to their traditions in the service of comfort and security. As an example, a physician began our psychotherapy session with the following question: “Did you know that emotional tears have high levels of prolactin, adrenocorticotropic hormones, and leucine-enkephalin that are produced by the anterior pituitary gland?”
“Gee, I had no idea,” came my frank admission. “But why are you asking me that?” He then recounted that his patient “broke down in tears without warning right in front of me in my office and I didn’t have the faintest idea what to do!” His anxiety was palpable. His personal “fiddler on the roof” was obviously organic chemistry.
I doubt that Tevye was an audiologist, but if he were, I wonder whether, like the participants in the second author’s (DC) workshop, he would have politely voiced enthusiasm for MI training but wouldn’t have taken advantage of it. Although MI has a structure and routine, it targets “messy” emotions and relies on some improvisation by the practitioner. This would be anathema to the routinized predictability of the status quo, the medical model, the patio pavers, the fiddler.
While learning MI is certainly cumbersome and may not come naturally, we believe that one potent underlying source of resistance is related to fear and anxiety. To continue my (author MAH) fantasied dialogue with Dr Smith, I asked him, “What might you be fearful and anxious about?”
“I’m afraid of opening up a can of worms!” he immediately replied.
“And then what?” I asked.
“I won’t know what to do or say to close that ‘can’ and stabilize the patient. I’m not a therapist, you know, and I never wanted to be a therapist. That’s why I’m an audiologist!”
He had a point about the can of worms. A hearing evaluation can trigger a slew of raw emotions associated with years of feeling short-changed at home and at work, missing words and conversations, feelings of inadequacy, loneliness, etc. The resulting affective eruption in the office can blindside both the patient and the audiologist.
It was now time to invite Dr Smith to explore his own internal emotional reactions to an affective eruption. “If you didn’t know what to do with a destabilized patient, how would you then feel about yourself?”
“What kind of question is that? This has nothing to do with how I’d feel about myself! [Showing irritation] I just can’t have a patient decompensating in my office, pure and simple! It’s well beyond my scope of practice.”
“Certainly I don’t blame you for not wanting a decompensating patient in your office. Who does? But may I ask you again: If that did happen, how would you then feel about yourself?”
“I wouldn’t be able to stabilize the patient. I’d feel frustrated, of course.” After some more prodding, he articulated that he would feel “inadequate” to the task of managing the out-of-control patient, again correctly emphasizing that that was not his training.
Struggling to manage emotionally destabilized patients often triggers earlier experiences or emotions that have nothing to do with one’s competence or training. No feeling exists in isolation. For example, the physician whose patient produced adrenocorticotropic tears recalled feeling terrified as a child of his mother’s emotional lability, secondary to her Bipolar Disorder. Until our discussion, he was unaware that he experienced flashbacks to his mother when his patients cried. This dynamic is termed traumatic transference: when one transfers the emotions that were associated with an earlier traumatic situation onto a present-day situation that is perceived as similar.
“Right, it’s not your training,” I responded. “Would you think back to earlier times in your life when you felt inadequate having nothing to do with audiology?”
Dr Smith’s eyes gazed upward as he retrieved an earlier experience. He recounted his confirmation speech in church at the age of 14. “The priest told me that, on that day, I would receive the gifts of the Holy Spirit through something he called ‘a sacrament of initiation.’ I had no idea what all that meant, but it obviously was a big deal. But I was so nervous I made a bunch of mistakes and screwed it all up.” He looked down at the floor as if he was 14 years old again.
I told Dr Smith about Brené Brown, a social worker who has studied two emotions that no one wants to talk about: shame and vulnerability. Shame is the most powerful, master emotion. It’s the fear that we’re not good enough. Vulnerability is basically uncertainty, risk, and emotional exposure. Most of us have experienced levels of shame and vulnerability. The only people who have never experienced these emotions are those who don’t have the capacity for empathy or connection.6
After my brief speech, Dr Smith asked, “So are you saying that I feel shame and vulnerability when I’m with patients? And are you saying I don’t take time to try to connect with them?” His voice reflected irritation and hurt.
“Absolutely no on both counts,” I quickly responded. “A foundation of audiologic treatment is to connect with one’s patients and provide a comfortable, safe setting. I’m speculating that when you do what feels most safe and familiar—connecting with patients, diagnosing, prescribing, etc—you feel competent and secure. But like all of us, when you leave that safe territory, when you bear witness to heightened levels of patients’ emotional concerns and their often messy ambivalence about improving their hearing, you’re in unfamiliar territory. At that point, you become anxious and fearful that things may go awry. Suddenly you don’t feel so competent anymore, and that’s when previous experiences of shame and vulnerability are likely to get triggered. In a sense, we ‘grow down’ and re-experience earlier emotions having to do with shame and vulnerability.”
Dr Smith neither nodded nor shook his head, but I could feel his “hard drive” working.
“So I have good news and bad news,” I continued. “First the bad news. This has to feel sh**ty. (Now he emphatically nodded his head.) Now the good news. All people, including professionals in my field of psychology, are prone to sometimes feeling shame and vulnerability and will run the other way. You’re very much not alone. I told Dr Smith about my patio, about Tevye the fiddler, and I recounted a quotation from a prominent psychiatrist, Irwin Yalom:
“How I long…for the certainty that orthodoxy offers…How comforting it would be to feel, just once, that I know exactly what I’m doing in my psychotherapeutic work for example, that I am dutifully traversing, in proper sequence, the precise stages of the therapeutic process. But, of course, it’s all an illusion. If they are helpful to patients at all, ideological schools with their complex metaphysical edifices succeed because they assuage the THERAPIST’S, not the patient’s, anxiety (and thus permit the therapist to face the anxiety of the therapeutic process). The more the therapist is able to tolerate the anxiety of not knowing, the less need is there for the therapist to embrace orthodoxy.”7
Personal and Professional Growth for the Patient and Practitioner
More good news: You can “detoxify” shame and vulnerability. Sometimes what feels anxiety-provoking can yield the most benefits. In the words of Carl Jung, “Find out what a person fears most and that is where he will develop next.”
Although adhering to a standard patient interview protocol may be comfortable in contrast to MI, which may be cumbersome and perhaps even anxiety-provoking, departing from the status quo may make the interview more interesting for you and your patients. It can be quite enlivening for the practitioner, as it sparks one’s creativity. Similarly, a musician reflected that improvisation keeps the music new and interesting, not only for the audience, but also for the performer.
Regarding professional growth, audiologists who attended a MI workshop at the Ida Institute emphasized its value for themselves (https://idainstitute.com): “It’s also fun to have a completely different conversation with the client,” one audiologist said. “It’s not just the nodding client and the blabbering audiologist. It feels like a nice conversation, during which you get a lot of information in a short period of time.”
“So, it has benefited you, too?” he was asked.
“Yes, it certainly has. When I think about the way I used to consult, it may have appeared to the professional that I understood what I was doing. But they weren’t individual consultations.They were standard and they sounded good…I just wanted to appear professional on the outside.”
As another audiologist put it (paraphrasing), “Sharing in the growth and development of another person as they cope with hearing loss is an honor, a life-altering, spiritual experience for those who are open to it. Our clients’ resilience promotes our increased respect for the human spirit.
“We have the experience of knowing intimately people we would otherwise not have known, and of sharing vicariously in others’ life choices and struggles, their most intimate feelings, needs, and concerns which get sparked by their loss of hearing. Our connections with clients through humor, love, and pain contribute enormously to our growth as individuals, add complexity to our lives, and increase our capacity for empathy and understanding.
“At times we have had glimmers of wisdom resulting from our work. Our clients teach us the things we might have learned from grandparents, wise elders. Sharing joy and sorrow, laughter and pain, wisdom and ideas with another person is at the heart of what it means to be human.”
Tradition = safety but ≠ optimal patient and professional growth
So why don’t some audiologists jump on this win-win opportunity? Why didn’t any participants from author DC’s training take advantage of further coaching and integration of any MI skills despite repeated offerings? We have discussed the prominent influences of fear and anxiety, but these emotions, like all others, do not exist in isolation. They are couched in a complex array of ambivalent emotions.
Most, if not all, our decisions are beset by some level of ambivalence. For example, you may be thinking, “On the one hand, this article is okay and thankfully not too long, but on the other hand, I could be watching the ballgame, but on the other hand, I wouldn’t learn as much about MI, but on the other hand, I deserve more relaxation time, but on the other hand…” It was Sigmund Freud who first formulated the ambivalence principle: the simultaneous existence of contradictory feelings towards something or someone.8
Tevye:“Excuse my interruption here, but I was the first one to talk about ambivalence! [Glaring at MH & DC] If you would have done a more thorough lit review, you would have discovered that I talked about ambivalence in 1905—about my daughters choosing their own spouses out of love—before most of Dr Freud’s fancy theories. I said:
“They gave each other a pledge. Unheard of, absurd. You gave each other a pledge? Unthinkable. Where do you think you are? In Moscow? In Paris? Where do you think they are? America?…Some things I will not, I cannot, allow. [But] he’s beginning to talk like a man.
But what kind of match would that be, with a poor tailor? On the other hand, he’s an honest, hard worker. On the other hand, he has absolutely nothing. On the other hand, things could never get worse for him, they could only get better.”
MH/DC: “We’re sorry for our oversight.”
Tevye: [Not acknowledging our heartfelt apology.] “I bet even the enthusiastic audiologists at Dr Citron’s Motivational Interviewing workshop had the same ambivalence about adopting a new skill as a patient does in making a change in their health. As you may know, MI emphasizes the importance of giving a voice to both sides of one’s ambivalence. Although those audiologists may have found MI to be beneficial, taking the next step to make the change and investing in a new skill is another thing entirely; it amounts to a whole new way of doing things (reflective/active listening). And it’s not a one-off quick solution. It requires the skills to guide another through the introspective reflections necessary to build an internal motivation. Even though MI is evidence-based, they may ask if it’s worth their investment. My clinical opinion is that they are stuck in ambivalence about learning MI. You should have hired me to use motivational engagement strategies with them!”
MH/DC: “Wow, we’re quite impressed with your clinical acumen, particularly because you were employed as a milkman in Anatevka!”
Tevye: “Thank you, but if you’re so impressed, you should make me at least the third author of this article.”
MH/DC: “Sorry, Tevye, Hearing Review has some weird editorial rule against listing fictitional authors in its bylines.”
Becoming Motivated to Use Motivational Interviewing
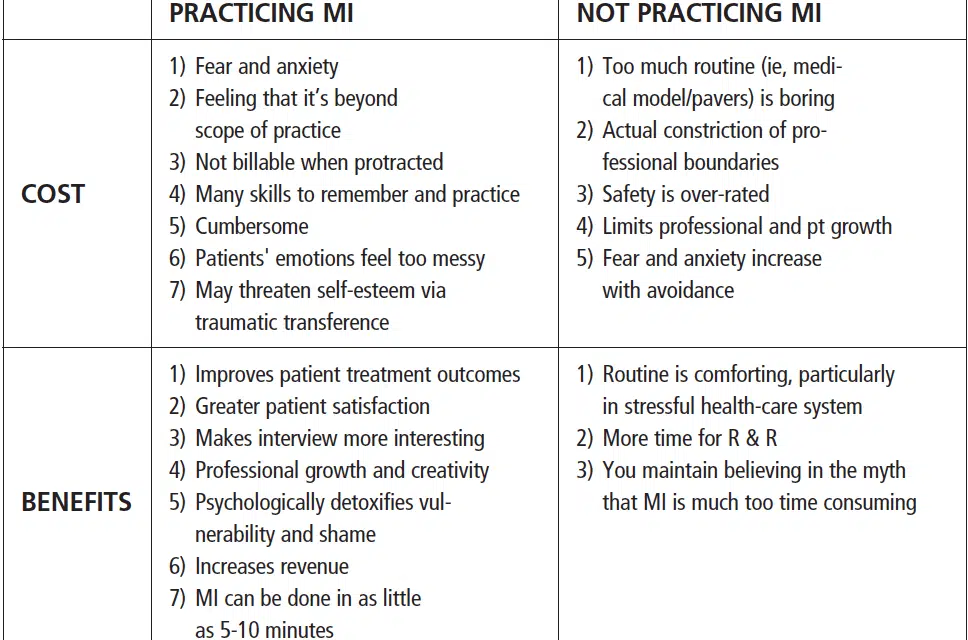
The MI decisional balance sheet is a visual tool that summaries the pros and cons of change. Figure 1 elucidates both sides of what may be some clinicians’ ambivalence about using motivational engagement tools.

Change is always easier when it happens to someone else. We, too, must admit how easy it is for us to become numb to the fear and anxiety that patients experience in a crisis, and how ambivalent or flat out resistant we can be when similarly challenged. We would all do well, even Tevye, to heed the words of audiologist John Greer Clark: “We ask our patients to step outside of their comfort zones every day. We have got to be able to do the same on their behalf. They deserve this from us.”
References
1. Gawande A. Being Mortal: Medicine and What Matters in the End. New York, NY: Metropolitan Books, Kindle Edition;2014:206.
2. Clark JG, English KM. Counseling-infused Audiologic Care. 3rd ed. Cincinnati, Ohio: Inkus Press, Kindly Edition;2018.
3. Beck DL, Harvey MA. Motivational interviewing. The Hearing Professional.2018:58-65.
4. Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. New York, NY: The Guildford Press;2012.
5. Beck DL, Harvey MA, Schum DJ. Motivational interviewing and amplification. Hearing Review.2007;14(11):14-20.
6. Brown B. I Thought It Was Just Me (But It Isn’t): Making the Journey from “What Will People Think? to “I Am Enough.” New York, NY: Avery Publishing;2007.
7. Yalom ID. Love’s Executioner and Other Tales of Psychotherapy. New York, NY: HarperCollins;1990:35.
8. Freud S. New Introductory Lectures on Psychoanalysis. New York, NY: W.W. Norton and Company;1933.
CORRESPONDENCE can be address to Dr Harvey at: [email protected]
Citation for this article: Harvey MA, Citron D. The Tevye Phenomenon: Why one may be ambivalent about using motivational engagement tools. Hearing Review. 2020;27(1):14-19.