
Hearing Aid Fitting | February 2018 Hearing Review
You’re not alone when you ask, “Should I turn off the advanced features when doing REM?”
This study looks at how advanced hearing aid features may affect the results of routine real-ear measurement (REM). One of the key points is that, by using speech noise stimuli (like the ISTS stimuli) during REM, you should be able to obtain an accurate representation of speech gain while not having to turn off all of the advanced features.
There is much literature on the subject of using real-ear measurements (REM) for verification of hearing aid fitting. In our review of the literature from the last decade, we found, not surprisingly, that as hearing aids came into their own in the digital age the advancements tended to make verification methods more complicated.
How could the Hearing Care Professional (HCP) ensure that measurements were accurate? Initially, directional microphones were identified as a feature that could affect accuracy, but this could be overcome simply by using proper patient positioning facing the REM speaker. However, advanced features—such as automatic directional microphone control, automatic volume control, noise reduction, digital scene classifiers, and expansion—have become common in hearing aids, and their impact on REM may be less obvious. Complicating matters, proprietary naming of features often does not offer clues as to how one might expect them to affect REM.
There is evidence that hearing instrument fittings that include verification with REM lead to higher user satisfaction.1 As audiologists who work with hearing aid development for a manufacturer, REM is invaluable to us for additional reasons. We use REM not only for verification in individual hearing aid fitting to prescribed targets, but also as a tool in hearing aid development to ensure that new hearing aids actually do what they are supposed to when coupled to a person’s ear. We also use it to help us figure out what different hearing aid processing features actually do to the acoustic input signal, and how this might relate to what users report about their subjective experiences with these features.
Some of these goals are obviously beyond what is relevant for a typical busy hearing aid dispensing practice. However, questions that often come up both in our clinic as well as in practices where the HCPs want to use REM, is how to set the hearing aids for the measurements, and if there is anything important to know in terms of the measurement itself, such as signal types and levels.
ReSound fitting software includes a dedicated program aptly named “REM test” that is intended for REM. It disables special signal processing, such as environmentally dependent gain features, noise reduction, directionality, and binaural features, so that the HCP can measure the gain and output of the hearing aids without these features impacting the measurement. Other manufacturers have similar test modes for performing REM.
But using a special test program for REM may add inconvenience and time to the appointment. And considering that users wear the hearing aids in their everyday environments with all of these features active, is this really the way that the hearing aids should be assessed? Or, put another way, how bad is it to not use the special test program if you want to do REM?
In this article, we present and discuss measurements from our lab to provide some guidance on the impact of hearing aid feature settings on REM to those HCPs who already use REM, as well as to those who might be interested in using it more regularly.
Hearing Aid Technology and REM
How can you predict if an advanced feature influences real-ear measurement? REM was introduced to clinical practice about the same time as compression circuits began to appear in commercial hearing aids, shortly followed by multiband compression circuits. The simplicity of analog linear hearing aids had otherwise made for relatively simple gain assessment with REM. There were really only two things to examine: gain for a moderate input level, and perhaps also maximum output with high-input level pure-tones. REM equipment offered multiple prescriptive targets for linear amplification, and narrowband signals were good enough, since the hearing aids amplified any type of signal equally.
However, the idea of placing a microphone inside the ear canal to pick up and measure the actual sound level in the ear canal started getting complicated as compression circuits quickly became commonplace. With all of the procedural factors affecting REM results, signal types and levels were added to the mix, along with the fact that prescriptive targets for nonlinear amplification lagged hearing aid advancements. HCPs were even cautioned against using probe-mic testing with modern hearing aids.2 Today, there is broad agreement that REM can be used with compression hearing aids to verify match to prescriptive targets, as well as to predict audibility of speech. Equipment capabilities, peer-reviewed prescriptive targets, and protocols for REM have been devised and updated to make this practicable.
While guidelines for REM regarding amplification of speech without special processing are readily available, modern digital hearing aids are quite complex. Numerous advanced features that affect gain are found in today’s hearing aids, including different types of noise reduction and environmentally dependent gain adjustment. Other features do not directly act on the gain of hearing aids, but still affect the sound that comes out of the devices and would therefore affect what is measured via REM. These types of features are common to most digital hearing aids today, and include directionality, feedback cancellers, and frequency lowering. Should these advanced features be left at user settings during the measurement, or should they be disabled in order not to “interfere” with the gain?
Table 1 shows a list of features that are commonly found in advanced digital hearing aids. Each feature is designed to manipulate the signal for a single purpose, whether it be comfort, sound quality, or speech audibility. It is important to remember that, typically, in a single hearing aid program several of these features are activated at one time and acting on the same input. For example, Program 1 might have a digital pinna feature, expansion, noise reduction, bilateral compression, and automatic volume control. If mid-level background noise is detected by the hearing aid, the low frequency gain may be reduced along with filtering of the entire noise spectrum, as well as an increase in high-frequency gain to increase the probability of hearing speech and a change in the directional pattern.
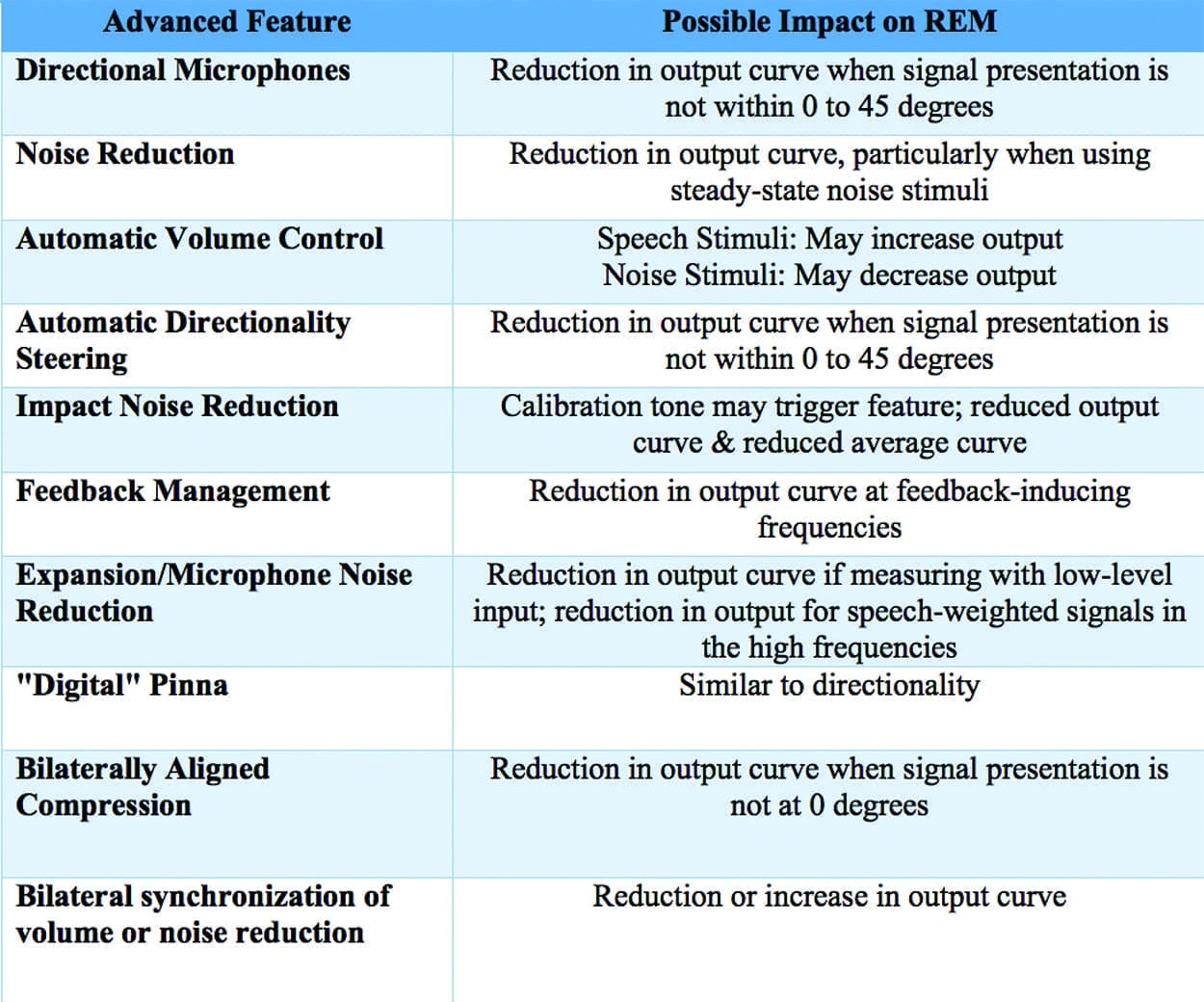
Table 1. Advanced hearing aid features and their possible impact on real-ear measurement.
We may know, in theory, how each of these features affect the signal, but the interaction among them may not be as clear. Conducting REM while in user settings, with a real-world input, allows the clinician to observe if the gain settings are appropriate with all these possible interactions taken into account. The point is that there is value in knowing how the combination of active features affects speech.
This naturally brings us to the test stimuli. Many approaches have been suggested regarding using particular stimuli, or disabling only certain advanced features. One suggested stimulus was speech-shaped noise.3 However, any type of steady-state signal can be expected to trigger noise reduction. It was therefore discussed that the noise reduction system could be turned off and the choice of test stimuli considered in order to prevent the noise reduction system from reducing gain while the measurement was being obtained.4 Speech and speech-modulated stimuli were introduced with the thought that this issue could be prevented, but also because the signal would better represent the sound that hearing aids are primarily designed and fit to amplify.
However, while turning advanced features off may allow the measurement to isolate the effects of compression only, it may cause a valuable observation to remain hidden. For example, perhaps the noise reduction in a particular hearing aid actually affects amplification for speech. Or perhaps an environmentally dependent volume or frequency response change is applied on top of the prescribed gain. Feedback managers may also impact gain, as they may layer feedback cancellation with gain reduction algorithms. In the case that the sum total of these advanced processing schemes reduces the gain relative to the prescription, it is wise to learn this during the fitting as well.
Current guidelines5-7 recommend modulated speech noise or a recorded speech passage at 65 dB SPL as a minimum for REM. With the appropriate stimuli, it is assumed that the hearing aids can be verified at user settings while still allowing the correct gain measures without feature effects.5,8,9 Finally, the Guidelines for Management of Adult Hearing Impairment7 from the American Academy of Audiology (AAA) suggest both that advanced features can be disabled while at the same time acknowledging that potential interactions among signal processing schemes may be missed. It is further recommended to verify special features individually.
Considering all this, it isn’t at all odd that HCPs still might ask, “Should all advanced features be turned on or off to ensure an accurate REM measure?”
Study Methods
To explore this question we conducted measurements using three sets of high-end behind-the-ear (BTE) hearing instruments currently on the market today. Each set of hearing aids was programmed to experienced user settings for a moderate hearing loss based on the NAL-NL2 fitting rule.
Program 1 was initial fit settings; therefore, all advanced features were set to the manufacturer’s default. Table 1 lists examples of features that were active in this condition. Program 2 was programmed with all advanced features off, or at least to the degree that the respective fitting software would allow. Real-Ear Aided Response (REAR) was conducted on the same adult ear at 65 dB SPL from a 0° azimuth to minimize any automatic directionality effects, in case it was active by default.
Both hearing aids were worn during the measurement even though only one ear was measured. This was to allow any binaural features to activate. There were two conditions: the first using the International Speech Test Signal (ISTS),10 and the second using ANSI Speech Noise stimulus, each of a 15-second duration. Both speech and noise were included, not only because they were recommended as the stimulus of choice at one time or another, but also because advanced hearing aid algorithms center their processing on the treatment of both speech and noise. Each of the two programs within the three sets of devices were measured with both stimulus types. The REAR curves were then compared within devices to determine if the features had an effect on the measurement.
Results
Figures 1a-c show difference curves between advanced features on and off with each of the stimulus types. The curves that are lower on the graph indicate that there is less of a difference between the measurements conducted with advanced features on and advanced features off. The higher the curve, the larger the difference between the gains with advanced features on and the gains with advanced features off, indicating a higher degree of impact of the advanced features on hearing instrument output. The data points at zero denote that the measurements matched exactly at that particular frequency, indicating no difference between the advanced features’ on and off conditions.
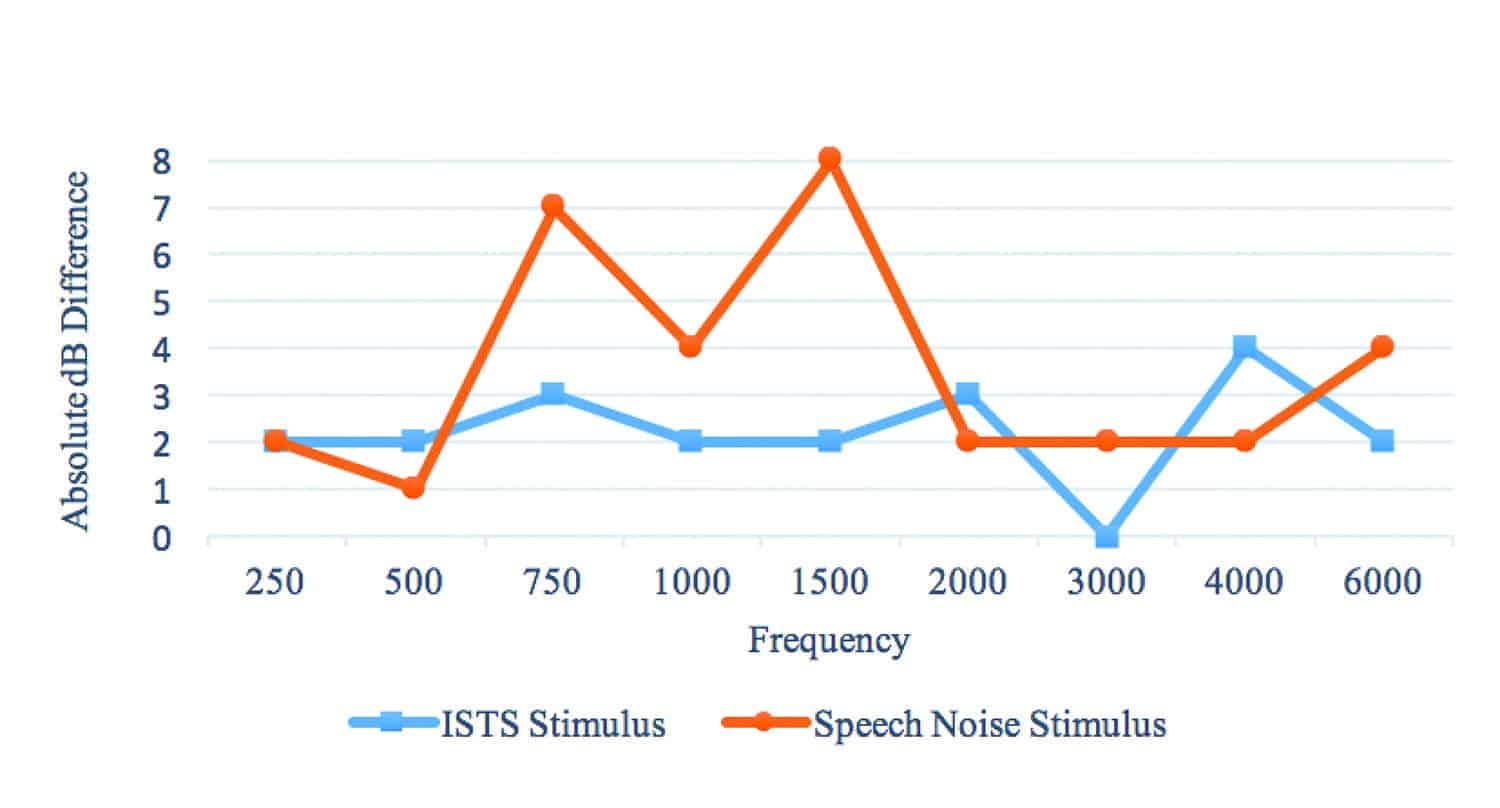
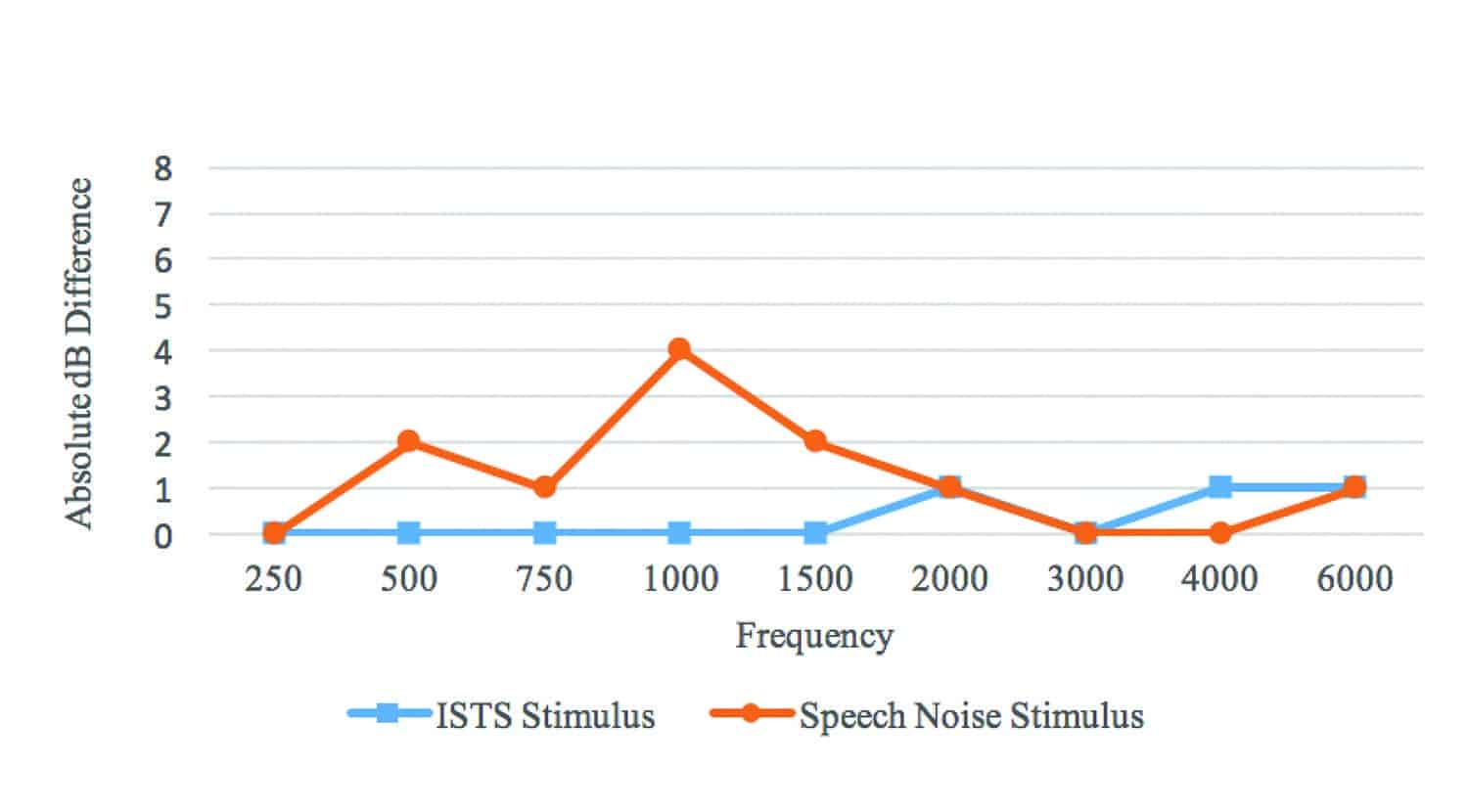
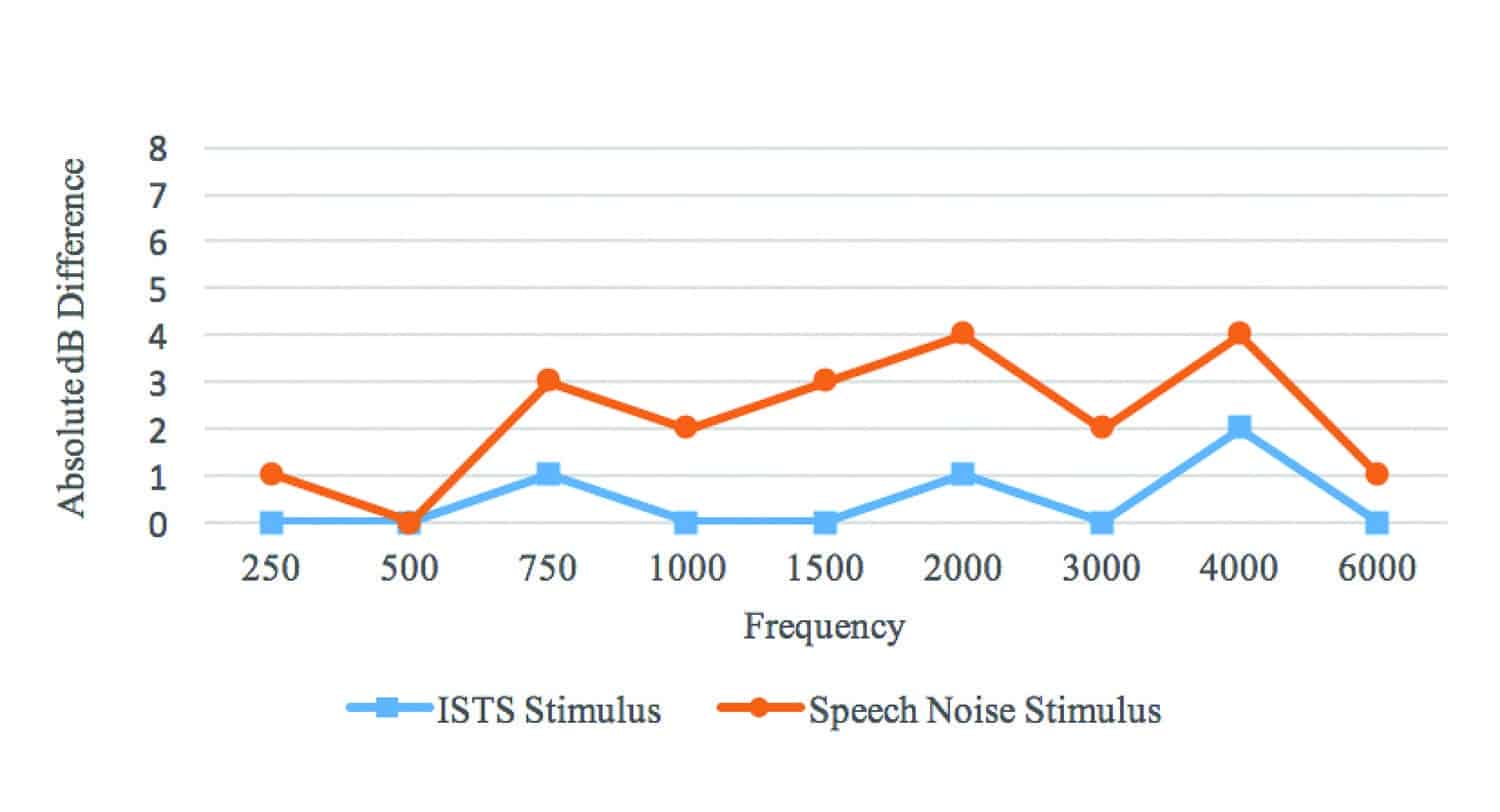
Figure 1a-c. REAR absolute differences between Program 1 (user settings) and Program 2 (features off) for each of the three sets of hearing instruments (Hearing Aids A, B, and C). Absolute values were used instead of raw values to highlight the degree of variation between features’ ON and OFF measurements. Fifteen-second ISTS stimulus showed less difference between programs than ANSI Speech Noise stimulus for each device.
It is apparent that the ISTS stimulus resulted in little deviation between Programs 1 and 2 for any of the three test hearing aids, leading to the conclusion that when verifying with a speech stimulus, the advanced hearing aid features will have little to no impact on the ability to match gain targets.
The measurements using ANSI Speech Noise stimulus, on the other hand, were significantly affected by advanced features. More variability among the behavior of the three different devices was also more evident when using the speech noise stimulus than ISTS. Differences between programs reached up to 8 dB in some cases.
Another factor worth noting with the noise measures was the signal duration. Two of the three sets of instruments did not demonstrate active noise reduction during the 15-second measurement, suggesting that stimulus duration had no impact on their output curves. However, the attack time on one set was so short that it began to affect the noise stimulus within a couple of seconds, showing a visible reduction as the measurement was taking place. This prompted an additional measurement, a REAR with a 30-second noise stimulus duration. As shown in Figure 2, the additional run time allowed the noise reduction system to further reduce the signal beyond the 15-second measure, creating a greater gap between the initial “features off” measurement and the “features on” measurement.
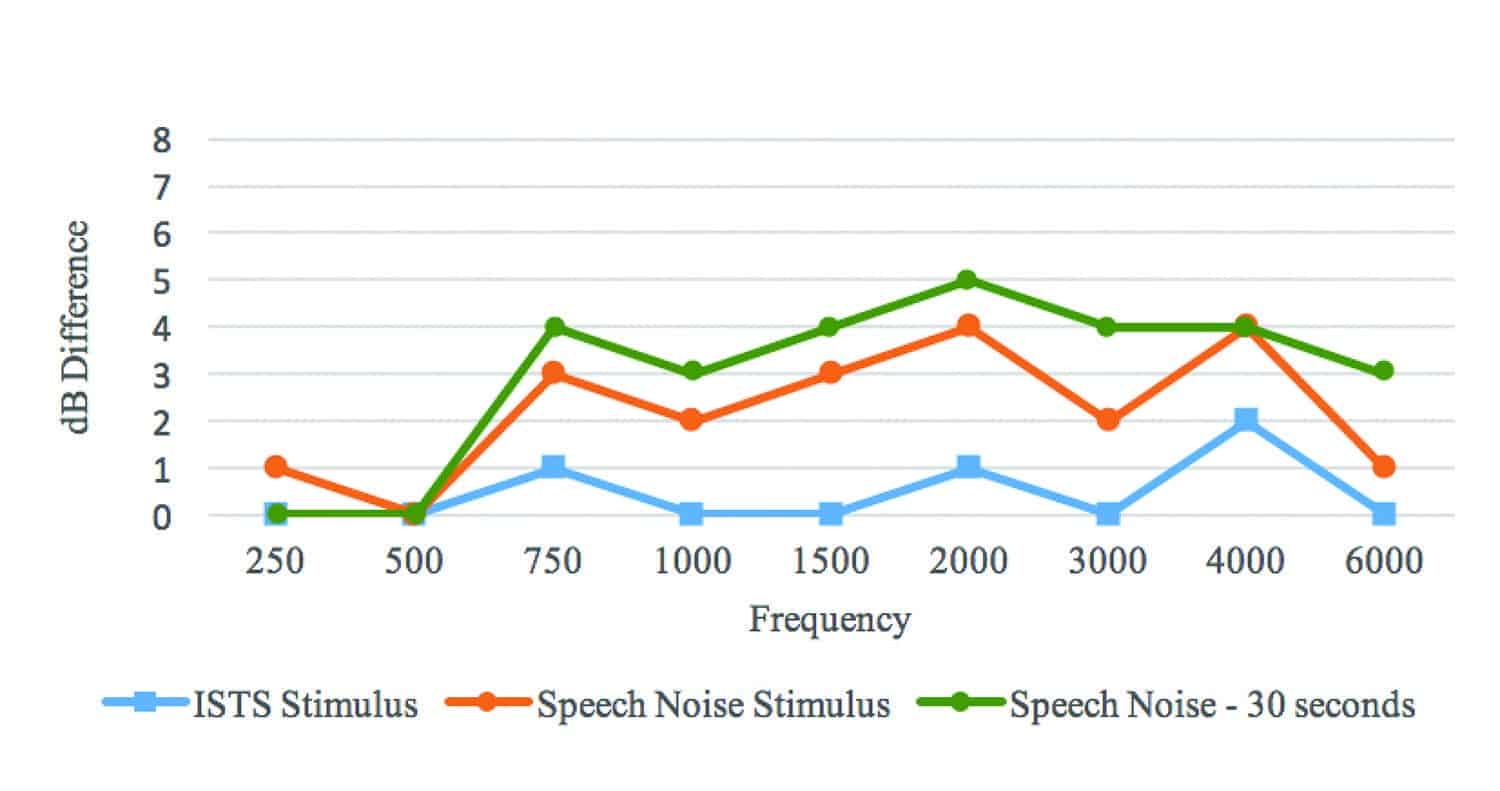
Figure 2. REAR absolute differences between Program 1 (user settings) and Program 2 (features off) for Hearing Aid C, including the additional 30-second noise measurement. This particular device seems to have a two-stage attack time on the noise reduction feature. While some gain reduction was noted for the 15-second noise measurement, additional reduction was exhibited after 30 seconds of exposure to the noise stimulus.
Discussion
Although this was not an exhaustive investigation, the measurements reported here reflect key considerations when performing REMs in the clinic. As shown, the steady-state speech noise (a stimulus without modulation) triggered a degree of gain reduction regardless of the device tested. This suggests that noise management features can be expected to have an impact on REM results if they are not turned off when using a steady-state noise as the stimulus. In comparison, there were fewer differences between the programs when the ISTS speech stimulus was used, suggesting that speech signals do not trigger the noise management technology in the same way that static noise does.
This suggests that REMs taken using speech stimuli will be a more accurate representation of how the hearing aid can be expected to amplify isolated speech, which is what fitting rule targets prescribe. This also allows the fitter to observe any impact of the noise reduction system on speech, if any. Using a steady-state noise stimulus may impact REM results by implying that the gain settings need to be adjusted more than necessary, which can result in patient dissatisfaction, noncompliance, or even negatively impact speech perception.
Another finding of this investigation relates to the duration of measurements. When completing REMs, HCPs may attempt “live changes” to the gain settings—continually running the stimulus while making changes to the gain settings in the hearing device and observing the immediate effect on the measurement. During this investigation, duration of the ISTS speech stimulus had no distinguishable impact on the output of any of the devices. However, the static speech-shaped noise did trigger increased noise reduction with the longer run time. Specifically, the degree of gain reduction in one device (Hearing Aid C) increased with the increased duration of exposure to the speech-shaped noise. Given this result, the longer a noise stimulus is run, the more noise reduction may apply. This could prompt the HCP to increase gain unnecessarily, with the possible worst-case result of overamplification.
Surveys have consistently found that, despite best practice recommendations, only about 40% of all those who fit hearing aids actually run REMs on a consistent basis. One of the most oft-cited reasons for not completing REMs is the time required to complete the measurements. The results here suggest that REM can be measured accurately and efficiently without having to make time-consuming advanced feature changes by utilizing speech stimuli, regardless of the device being fit—thereby ensuring that both the HCP and the hearing aid user can be confident in the fitting and getting the hearing aids set up for optimal outcomes.
Solutions for Conducting REM
This study looked at the impact of advanced features on versus off during routine REM when attempting to match prescriptive targets. It highlights three key points:
- Stimulus type matters. As presented above, static noise stimuli, even if it is speech-shaped noise, can trigger noise reduction and advanced features, which can alter the REM response.
Simple solution: Use speech stimuli, such as the ISTS stimuli. This allows the fitter to avoid turning all the advanced features off, which can take time away from the remaining fitting process.
- Measurement duration. The duration of the stimuli may change the degree of noise reduction or the application of other advanced features.
Simple solution: If you are running REMs and prefer to make adjustments in real-time, use speech stimuli; this should give you an accurate representation of gain for speech and is unlikely to activate the advanced features.
- Although not demonstrated in this investigation, directionality can affect the results of REM. Most advanced hearing aids use automatic algorithms that turn directionality on and off, and the HCP won’t know what mode the microphone is in. Additionally, some hearing aids have advanced algorithms to align gains on bilaterally fit devices to preserve interaural cues.
Simple solution: Use a speech stimulus, and make sure the user is facing the speaker from which the stimulus is presented.
Correspondence can be addressed to HR or Dr Koehler at: [email protected]
Original citation for this article: Koehler ED, Wright NA. How should modern hearing aids be programmed for verification with REM? Hearing Review. 2018;25(2):24-28.

References
-
Kochkin S. MarkeTrak VIII: Consumer satisfaction with hearing aids is slowly increasing. Hear Jour. 2010;63(1)[January]:19-32.
-
Mueller HG. Probe microphone measurements: 20 years of progress. Trends Amplif. 2001; 5(2): 35-68.
-
Dillon H, Keidser G. Is probe-mic measurement of HA gain-frequency response best practice? Hear Jour. 2003;56(10)[Oct]:28-30.
-
Mueller HG. Probe-mic assessment of digital hearing aids? Yes, you can! Hear Jour. 2001;54(1)[Jan]:10-17.
-
Mueller HG. Probe-mic measures: Hearing aid fitting’s most neglected element. Hear Jour. 2005;58(10)[Oct]:21-30.
-
British Society of Audiology and British Academy of Audiology. Guidance on the use of real ear measurement to verify the fitting of digital signal processing hearing aids. July, 2007. Retrieved October 4, 2017: http://www.thebsa.org.uk/wp-content/uploads/2014/04/REM.pdf
-
Valente M, Abrams H, Benson D, et al. 2007. Guidelines for the audiologic management of adult hearing impairment: American Academy of Audiology Task Force. https://audiology-web.s3.amazonaws.com/migrated/haguidelines.pdf_53994876e92e42.70908344.pdf
-
Aazh H, Moore BCJ. The value of routine real ear measurement of the gain of digital hearing aids. J Am Acad Audiol. 2007;18(8):653-664.
-
Mueller HG, Picou EM. Survey examines popularity of real-ear probe-microphone measures. Hear Jour. 2010;63(5)[May]:27-32.
-
Holube I, Fredelake S, Vlaming M, Kollmeier B. Development and analysis of an International Speech Test Signal (ISTS). Int J Audiol. 2010;49(12):891-903.

Thank you for a very interesting and informative article.
My observation when completing REMs using speech stimuli is that the client almost 90% of the time prefers the software settings but not the REM settings! Is this normal?
Hi, Glad to hear you enjoyed the article.
I am going to make the assumption that when you say settings that are talking about gain settings. Let me know if I am incorrect in that.
It is not uncommon to hear that gains fine tuned to match target are not readily accepted by the wearer as they are often higher than those estimated by the software.