
Special Report | June 2017 Hearing Review
Editor’s Note: As reported in last month’s edition of The Hearing Review (“FTC Workshop Looks at OTC Hearing Aids and Regulatory Issues,” May 2017 HR, pgs 8-9), the US Federal Trade Commission (FTC) held an important workshop on April 18 titled, “Now Hear This,” which looked at myriad issues surrounding technology and competition in hearing aid distribution, as well as how over-the-counter hearing aids might impact customer satisfaction, the use of amplification products, consumer safety, and professional care. Four key subject areas were addressed by panels at that meeting, including 1) Innovations in Hearing Technology; 2) Innovations in Hearing Aid Delivery; 3) The Costs and Benefits of Hearing Care Regulations; and 4) Informing Consumer Choice in Hearing Healthcare, and as the HR article noted, divergent viewpoints were expressed. The following is the Hearing Industries Association’s (HIA) written response, submitted by HIA President Carole Rogin, on the most contentious issues covered at the FTC workshop (abridged by HR). Along with Rogin and HIA Executive Director Andy Bopp, the comments draw heavily on the collaborative work of industry audiologists Douglas Beck, AuD, Oticon; Harvey Abrams, PhD, audiology consultant for HIA and the Better Hearing Institute; Brent Edwards, PhD, Earlens; David Fabry, PhD, GN Hearing Systems, and Thomas Powers, PhD, audiology consultant for Signia.
The Hearing Industries Association (HIA) appreciates the opportunity to submit additional comments on the Federal Trade Commission’s (FTC’s) April 18, 2017 public Workshop on hearing aids entitled “Now Hear This.” HIA applauds the FTC for convening this meeting, which brought together a wide range of interested parties with different perspectives. While many of the presentations at the FTC Workshop brought clarity to several key points, there were several statements made to which HIA would like to further respond.
The objective of the Workshop was to address concerns with respect to the access and affordability of hearing aids. As detailed in our initial set of comments to the FTC submitted on March 31, 2017,1 HIA understands and appreciates these concerns and the need to address them. However, several panelists at the Workshop inaccurately characterized the hearing aid industry, the accessibility and pricing of hearing aids, the relevant technology, and the FDA regulatory scheme. HIA therefore takes this opportunity to respond to some of these comments.
The current situation is not as dire as many of the panelists implied. Technology is flourishing, patient satisfaction is thriving, and information is abundant. And while HIA recognizes that affordability is still an issue for some, it is a fallacy to presume that a Personal Sound Amplification Product (PSAP) can currently replace the hearing aid.
Patient satisfaction has never been higher in the US hearing aid market. MarkeTrak data shows an overwhelmingly high patient satisfaction rate. In 2016, patients reported overall satisfaction at a rate of 81% in contrast to 74% in 2008.2 Consumer satisfaction with current hearing aids is high and growing, with:
- 91% satisfaction rating for those obtained since 2014;
- 77% for hearing aids obtained between 2010 and 2013, and
- 74% for hearing aids obtained prior to 2010.2
Based on more than 30 years of data from MarkeTrak—a tracking survey of the hearing aid market—overall satisfaction with hearing aids is at its highest level ever. Consumer Reports supports this assertion with its finding that nearly 73% of survey respondents were “highly satisfied” with their hearing aids.3
Better products, in addition to better experiences with hearing care professionals, contribute to the improving satisfaction rates. As a number of panelists discussed at the Workshop, it is important not to understate the role of hearing care professionals in patient satisfaction. A total of 95% of hearing aid owners are satisfied with the professionals that fit them.2 In markets where there is no formal audiology education, such as Japan, outcomes and patient satisfaction are quite poor despite the adoption of the same hearing aid technology provided to hearing aid consumers in the United States.4 Similarly, in a study of AARP members on the “State of Hearing Health,” respondents reported that “finding a professional with a high level of training on hearing issues” was critically important.5
The satisfaction rates with both products and professionals indicate that the industry is meeting the needs of existing hearing aid patients. HIA acknowledges that there is an unmet need to address. But contrary to assertions at the Workshop, this unmet need will not be addressed simply by repositioning consumer electronic products as hearing aids under voluntary PSAP standards crafted by industry. And notwithstanding the consumer electronic industry assertions, because they are intended to be used in the treatment of a medical condition, hearing aids continue to be a medical device appropriately regulated by FDA.
1) Unmet Need/Accessibility
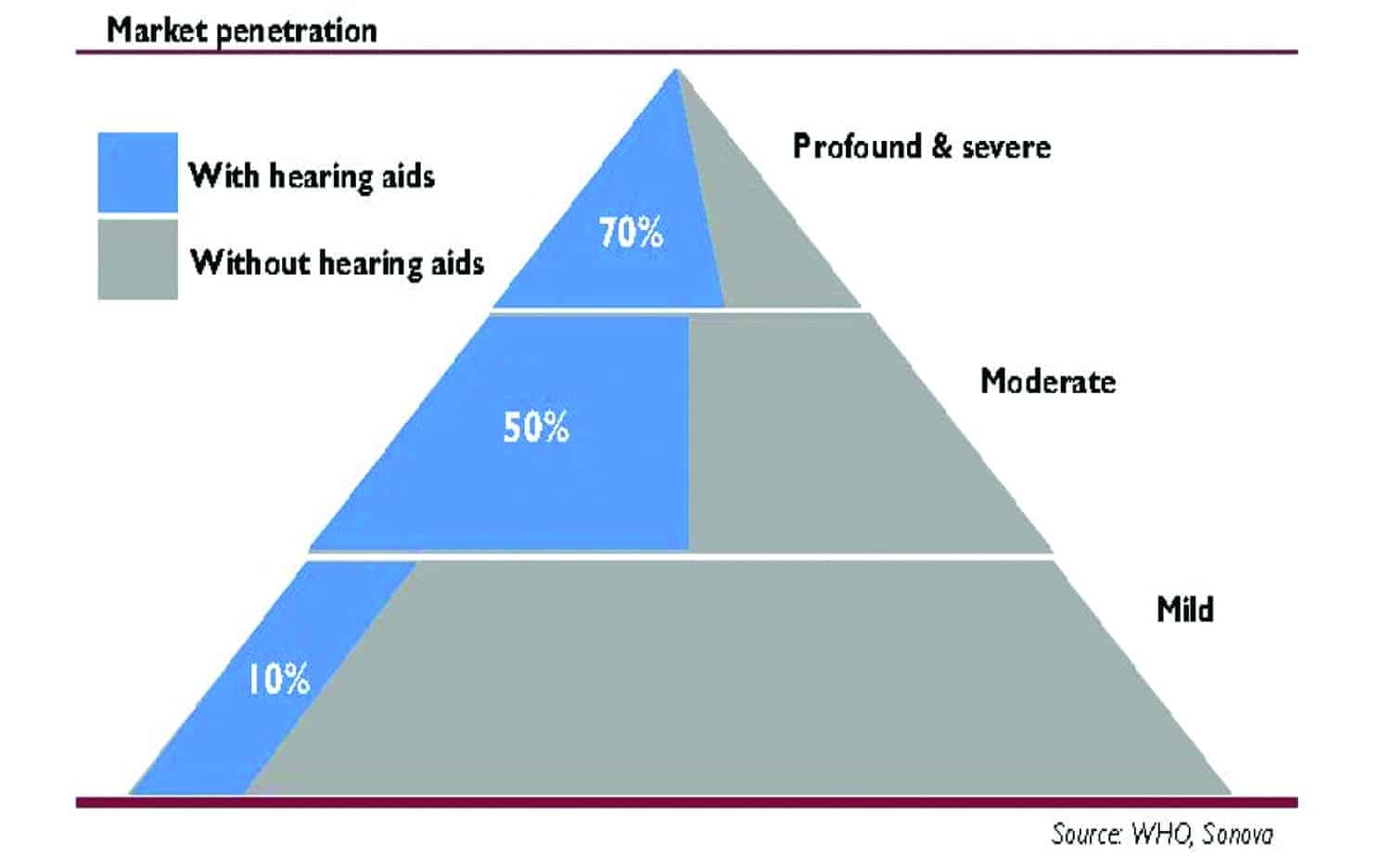
Figure 1. Hearing loss types, market size, and estimated market penetration of hearing aids (in blue). Sources: Niels Granholm-Leth, Carnegie Bank6; WHO, Sonova.
As noted, several speakers at the FTC Workshop, including Acting Chairman Maureen Ohlhausen, referred to the “unmet need” for hearing assistance. The vast majority of people with untreated hearing loss are those with mild hearing loss.6 As shown in Figure 1, approximately 70% of people with profound or severe hearing loss and 50% with moderate loss have obtained hearing aids, but only 10% with mild loss have. Therefore, the “unmet need” principally refers to a subset of potential patients—those with mild hearing loss.
In discussions surrounding the proposal of Over-the-Counter (OTC) hearing aids, the recommendation made by President’s Council of Advisors on Science and Technology (PCAST), National Academies of Sciences, Engineering, and Medicine (NASEM), and selected presenters at recent US Food and Drug Administration (FDA) and FTC Workshops, has been that OTC hearing aids serve to address an “unmet need.” To do so, the suggestion has been to make these hearing aids available to individuals with mild-to-moderate hearing loss.
However, the conflation of “mild-to-moderate” suggests that there is no difference between them in suitability for OTC status. This assumption seriously underestimates the significant communication challenges faced by those with moderate hearing loss, particularly those at the more severe end of that range. Compared to those with mild hearing loss, those with moderate impairment are likely to have greater sensory and neural damage leading to significant difficulties hearing and understanding speech in quiet environments and even more so in noisy environments or in the presence of multiple talkers.
Even more troubling is emerging evidence that links hearing loss to specific chronic conditions. For example, as reported by Drs Frank Lin and Luigi Ferrucci, hearing loss was significantly associated with reported falls with a 1.4-fold increased risk of an individual reporting a fall over the preceding 12 months for every 10-dB increase in hearing loss.7 According to these data, an individual with a moderate hearing loss may have up to a 4-fold increased risk of reporting a fall in the previous year compared to an individual with mild hearing loss.
In a landmark study examining the relationship between hearing loss and incident dementia, Lin and colleagues reported that, compared with normal hearing, the hazard ratio for incident all-cause dementia was 1.89 for mild hearing loss and 3.0 for moderate hearing loss.8 The risk of incident Alzheimer’s Disease also increased with the severity of loss at a rate of 1.20 per 10 dB increase in hearing loss. Therefore, individuals with moderate hearing loss could have over a 3-fold increased risk over time of an Alzheimer’s Disease diagnosis compared to those with mild hearing loss.
Additionally, the comorbidity of hearing loss and diabetes, hypertension, and stroke has been well-documented.9-11 The research on diabetes is varied: some reports show mild high-frequency hearing loss, some low-frequency loss, and some no threshold loss, but abnormal otoacoustic emissions or speech in noise results in all reports. However, data from numerous studies using the NHANEs database suggest that individuals with diabetes are at elevated risk for significant hearing loss when compared to persons without diabetes.12
While mild-to-moderate hearing loss by itself may present little “disability,” it may, in fact, be an indicator of more significant health conditions. Now that FDA has indicated that the physician referral requirement in adults considering use of amplification will no longer be enforced, this alone may present patient risks. In sum, the difference between mild and moderate hearing loss is more than a simple matter of “degree,” and the benefit to risk ratios are not the same. Therefore, OTC hearing aids should be designed to address the unmet needs of patients with mild loss rather than mild-to-moderate.
And, with respect to the “unmet need” with mild hearing loss, a significant portion of people with mild hearing loss do not want and do not believe they need a hearing aid.13 Professional literature indicates that many adults with hearing loss measured on an audiogram do not require hearing aids.14 Specifically, adults with normal cognitive function have intact language, a sense of turn-taking, world knowledge, vocabulary, and other adaptive and behavioral skills. As such, many adults with mild hearing loss choose to “fill in the blanks,” ask for a repeat or re-wording, or place themselves strategically in the environment to maximize sensory input (primarily hearing and vision). As Lucille Beck, PhD, of the Department of Veterans Affairs (VA) explained at the Workshop, the fact that a patient has hearing loss as demonstrated on an audiogram does not mean that he or she needs hearing aids.
Hearing aid recommendations are ideally based on communication needs,15 and communication needs cannot be predicted based on a mild hearing loss. Each individual must be assessed based on personal and unique needs. While some people with mild high-frequency hearing loss may want or need help, others do not. Indeed, just as not all people with dental problems seek dental care, and not all people with visual problems correct their vision, there certainly are people with hearing loss and listening problems who choose not to address these same problems for reasons of their own.
Further, a complicating factor for adults with mild hearing loss is that 10-15% of adults without hearing loss report difficulty understanding speech in noise.16-18 These people may indeed report or perceive hearing difficulty, but a hearing care professional may discover more of a listening issue than a hearing issue.19-20 Here, listening is the ability to make sense of sound while hearing is the perception of sound. The ability to listen is the result of hearing and cognitive processes: “listening is where hearing meets brain.”21 There are many reasons why an adult may “hear” but cannot understand: auditory processing disorders, attention deficit disorder, auditory neuropathy spectrum disorder, or synaptopathy, etc.22 Therefore, this “unmet need” category discussed at length at the Workshop may include both listening and hearing issues, in addition to those individuals who may not want to obtain treatment. Simply providing an OTC option for such people will not address their specific needs—especially those with moderate or greater hearing loss.
2) Cost
While cost is indeed a reason some people do not acquire hearing aids, objective research and market analysis has shown cost is not the primary driver. As noted above and as discussed extensively in HIA’s previously submitted comments,1 perceived need is the primary driver of hearing aid acquisition. This is supported by both Consumer Reports3 and MarkeTrak data.2 Similarly, a 2014 study released by the Consumer Technology Association (CTA) showed that the most common reason for consumers with “a little trouble hearing” not to seek medical care was not cost, but that their hearing difficulties were not bad enough to warrant action.23
Real-life examples have supported the contention that cost is not the sole barrier to hearing aid adoption. In many countries, hearing aids are available for free as part of national healthcare systems; this is true of the Scandinavian countries, the United Kingdom, and other nations within the European Union. Yet the uptake is rarely higher than 50% of eligible people (Denmark being an exeption with an adoption rate of 53% in 201624). Indeed, no other country with a high degree of private payers has higher penetration rates than the United States.
The Workshop discussion, informed by the PCAST report,25 cited the cost per pair of hearing aids as $4,700 every 5 years. This figure disregards the multitude of lower cost options, such as Costco’s premium products available for $1,799 per pair and Walmart’s hearing aids for $800 per pair. As discussed in HIA’s previous comments,1 consumers can find a custom-fitted hearing aid with service for as little as $500.26
It should also be noted that hearing aid payment assistance is available and legally required in every state under Medicaid for children, and provided in some states for those patients with hearing loss who cannot afford medical care.27 Additionally, 20% of all hearing aid distributions in the United States are provided to veterans as a benefit for military service while tens of thousands are distributed through other insurance companies.28 Consumer Reports states that its readers who purchased hearing aids spent an average of $2,710 of their own money even though many may have hearing aid coverage of which they are unaware, including federal workers and veterans.29 For those with private health insurance, just over one-third saved money on their hearing aid purchase, as some insurers (eg, Aetna) provide a discount plan through specific supply lines.30 Further, hearing aids and batteries qualify as a legitimate expense for consumers with health savings or flexible spending accounts. Therefore, some consumers may share the expense with third-party payers.
Undoubtedly, some people struggle to pay for hearing aids, but are not eligible for financial assistance; the cost may be too high for these consumers. But it is important to note that the majority of the costs for hearing aids are for the service rather than the device itself. Typically, only about one-third of the consumer’s cost is attributable to the device itself; the other two-thirds is the cost associated with a multitude of crucial hearing aid-related evaluation, testing, treatment, and warranty services provided by the hearing professional, often including “no-charge” multi-year follow-up care to adjust and maintain the devices as needed.31,32 These same office visit costs would necessarily be added to the total cost of a PSAP or OTC hearing aid should patients require additional services and adjustments, which the data show is extremely likely.
3) Information Costs and Consumer Access to Hearing Aids
A theme throughout the Workshop was that consumers have little information with which to make decisions related to hearing aid purchases. There was also an assertion that the consumer has no opportunity to try hearing aids or their specific features prior to purchase. Neither of these contentions is accurate.
Information sources are plentiful and varied. In addition to commercial sites, one can easily find information from the impartial American Academy of Audiology (AAA), American Speech-Language Hearing Association (ASHA), Academy of Doctors of Audiology (ADA), Better Hearing Institute (BHI), International Hearing Society (IHS), Consumer Reports, FDA, the FTC, and more. As referenced several times at the Workshop, the Hearing Loss Association of America (HLAA) publishes extensive resources assisting consumers in the hearing aid acquisition process. Hearing Review provides unbiased comparisons and reviews of hearing aids while Consumer Reports provides helpful information to guide consumers to save costs. Similarly, BHI, the education arm of HIA, provides a guide to purchasing a hearing aid, as well as an extensive collection of information about the hearing aid selection process and available technology.
More than 30 states have adopted laws that mandate trial periods of 30 days or more, and many retailers have contract requirements which allow the majority of consumers to “try before they buy.”33 Costco, for example, has a national in-store policy of a 180-day return period.34 Manufacturers offer these same types of programs, which enable consumers to try different levels of technology at home in real-life situations in order to determine the appropriate level of technology needed (eg, Amplifon has a 60-day trial period).35 In general, manufacturers absorb these costs related to the device while the professional may charge a nominal fee to cover their fixed costs of doing business. These professional fees are often state-regulated.
4) Competition in the Industry
While a common refrain, the contention that competition does not exist in the hearing aid industry is plainly erroneous. There is vigorous competition between retailers and between manufacturers. Consumers may purchase hearing aids from multiple sources, including thousands of online retailers, speech and hearing clinics, hospitals, national hearing aid centers (Beltone, Miracle Ear), doctors’ offices, Costco, Sam’s Club, audiology offices, private hearing aid offices, Medicaid, and some not-for-profit organizations. In addition, CVS has just opened seven hearing centers within stores in the Baltimore-Washington area, with plans to expand to 50 locations by the end of 2017.36 The US Bureau of Labor Statistics reported that 6,221 retail businesses sell hearing aids in the United States as of July 2014, as well as 12,250 audiologists, and 5,570 hearing aid specialists.37
There is also robust competition with respect to the manufacturing side of the industry. While critics imply that the largest manufacturers control the market to the exclusion of other manufacturers and artificially set prices high, six manufacturers is an “unconcentrated” market with a healthy level of competition according to the Department of Justice and the FTC’s own economic measures of market share concentration.38 And in addition to the primary six manufacturers, there are numerous other hearing aid manufacturers currently innovating and marketing in the hearing market. At last count, there were 97 entities in FDA’s registered manufacturer database listed as manufacturers of hearing aids, both wireless and air conduction.
Hearing aid manufacturers compete on technology, with first-to-market technology innovations producing meaningful market advantage. Frequency lowering, binaural beamforming, advanced feedback cancellation, and made-for-iPhone wireless were all technologies that provided a competitive advantage to the first companies that introduced them into the market. Major manufacturers spend significant resources on research and development to support these competitive technology development efforts.
Additionally, hearing aid startup companies continue to introduce healthy competition to the industry by bringing innovative technology to market. Earlens, Eargo, and iHear are just three of many companies competing with innovative solutions for people with hearing loss. Partnerships between major manufacturers and startups are also providing a competitive technological advantage.
5) PSAPs & Hearing Aids are Not the Same
At the Workshop, representatives from the consumer electronics industry repeatedly stated that PSAPs and hearing aids are technologically the same and distinguished only by permissible marketing claims. It is accurate to state that FDA’s regulations do not mandate an inherent difference between a hearing aid and a PSAP, as the regulatory status is based on intended use. Current PSAPs, however, are designed only to increase amplification, and therefore do not treat hearing loss in the same way as hearing aids.
Hearing aids are designed to meet the vast array of personal amplification needs through flexible controls and sophisticated software. They are researched and developed based on the principles and observations of decades of audiologic research. Hearing aid manufacturers have developed extraordinarily sophisticated products, which include rechargeable batteries, tiny batteries, adaptive directional microphones, digital noise reduction, frequency compression and transposition, environmental classification, feedback management, multiband compression, music processing, digital platforms that perform more than 1 billion calculations per second, maintenance of interaural loudness cues and timing cues, telecoils, BlueTooth, Near Field Magnetic Induction (NFMI), very low distortion, and extended bandwidth (generally to 10-12 kHz).
Conversely, PSAPs, by definition, assist only with amplification. Dianne Van Tasell of Bose Corp explained at the Workshop that… PSAPs are not subject to the same quality systems that hearing aids are; consumer electronic companies use quality systems that are not sanctioned or approved by FDA…[The standards] developed by the consumer electronics industry make clear that PSAPs are intended only for amplification. The scope of the CTA standards states that the standard “includes technical performance metrics and associated target values for consumer products that provide personal sound amplification and/or enhancement to a user.”39 Thus, the focus is on loudness rather than managing the complex auditory consequences of sensorineural hearing loss.
PSAPs and hearing aids do share some of the same component categories, such as multi-channel compression, noise reduction, feedback cancellation, and directionality, but there are vast differences in the specific technology adopted. This is analogous to cars and motorcycles: both contain engines and transmissions, but the engines and transmissions in a car are not the same as that of motorcycles.
Under the FDA regulatory framework, the consumer electronic industry’s performance comparisons between PSAPs and hearing aids would be considered misleading.40 PSAP manufacturers have said the products are interchangeable but have not presented clinical data demonstrating comparable safety and efficacy between hearing aids and PSAPs. Nor have they even demonstrated that their products address the frequency and intelligibility issues critical to addressing hearing loss. Supporters of PSAPs assert that PSAPs are safe and effective for the same intended uses as hearing aids, yet have provided no data to support that assertion. Purported bench-test studies do not show how well PSAPs would address hearing loss when used by a consumer to self-diagnose and self-treat. Further, there are published bench-test studies that demonstrate significant problems with PSAPs.41
6) Safety/Efficacy of PSAPs is Unknown
Despite repeated assurances at the Workshop that PSAPs are safe and effective, this has never been established. The long-term effects and impacts of PSAPs are unknown. Studies have shown that many of the PSAPs currently on the market are unsafe and may damage hearing, and the literature on PSAP safety and efficacy in clinical use is nonexistent.42 Even with the adoption of the CTA’s voluntary standards, PSAP manufacturers can choose not to comply and continue to market PSAPs with unknown safety and efficacy standards. Voluntary standards do nothing to ensure the safety of all PSAPs.
A speaker at the Workshop suggested that voluntary standards will cause the good PSAPs to succeed while the bad PSAPs fail. However, this theory contradicts both economic principles and real-life examples. Under Gresham’s Law,43 “bad money drives out good” based on an asymmetry of information. If all bad products are passed off as good, a buyer will pay only the fair price of the bad product to reduce the risk of overpaying. Therefore, the bad product is purchased more than the good product, and the good product is priced out of the market. This exact scenario happened when the well-designed but comparatively costly ($299) PSAP, Soundhawk, eventually exited the market. While the Soundhawk has been called “the best performing PSAP,” it was more expensive than competitors and failed commercially; it is no longer marketed.41
Hearing loss is a medical problem. Treatment of this medical condition requires a medical solution. While PSAP manufacturers claim they can provide such a solution, they desire to do so without regulatory oversight. A significant part of the FTC’s mission is to ensure claims are supported by adequate scientific evidence. The FTC has a duty to protect people with hearing loss from false and misleading claims. If PSAPs have free rein to make hearing loss claims, the proliferation of hundreds of types of PSAPs with their own claims will raise regulatory and resource challenges to the FTC and product quality challenges for consumers.
Conversely, hearing aid manufacturers have an excellent track record of safety, and their products are safe and effective. There are virtually no reports of damage secondary to hearing aids dispensed properly through hearing healthcare professionals. For nominal cost—approximately 20¢ per $1,000—hearing aid manufacturers have complied with FDA’s Quality System Regulations (QSR) to ensure the safety and efficacy of the products.
To be clear, PSAPs and the proposed OTC hearing aid class are not intended to be interchangeable. OTC hearing aids, by definition, will be medical devices. As devices, they will need to meet FDA’s safety and efficacy requirements, as well as substantiate their claims.
7) Entry Level vs Premium Products
Some discussion at the Workshop questioned the benefits of premium hearing aids in comparison to entry level hearing aids. HIA would like to clarify that there are, indeed, technical differences between the product segments. As Jan Metzdorrf discussed, these differences are distinguishable to users based on lifestyle factors, such as the variable environments in which they are used. For example, the very best noise reduction circuits are available only in premium hearing aids. Additionally, the maintenance of spatial cues (interaural loudness and timing differences), which help patients know where to focus their attention and thereby improve speech in noise, are features available only in higher level products. Similarly, multiple wireless systems, such as NFMI and Bluetooth (BT), are available together only in premium products.
Of note, many of the features currently available in “entry level” products were available in premium products just a few years ago. The value of products available at all price points continues to increase as the development and application of new technologies is incorporated into entry level units within a relatively brief time frame.
On the Innovations in Hearing panel discussion, Jani Johnson, AuD, PhD, explained a University of Memphis study that purportedly showed that there was no satisfaction difference between entry and premium level hearing aids; the study noted that there is no information provided on feature benefit and no validation done.44 But this is not so. All major manufacturers thoroughly test their technology and have extensive education programs in place; however, this information is directed to audiologists rather than patients. Explanations regarding how the technology works, how it differs from other technologies, the clinical protocols used, the outcome data obtained, and the types of hearing loss that benefit from the technology are made available in various forms, including in trade journals, scientific conferences, professional organization conventions, and peer-reviewed journals.45-47
8) CTA Standards
Editor’s note: Due to space requirements, this section was heavily abridged; see the technical details of HIA’s response at goo.gl/C3Vv89.
Bill Belt of CTA discussed the CTA-developed voluntary standards for PSAPs (ANSI/CTA-2051) at the FTC Workshop, and he emphasized that “most hearing aids would fail” the voluntary standard. That may be so, as hearing aids were not designed to pass this arbitrary standard, but passing of the standard does not ensure that a PSAP user with hearing loss would benefit.
Significantly, these standards were drafted by the very industry they are intended to control without any third-party engagement. The standards document does not acknowledge any other contributors, though previous reports by Mead Killion, PhD, stated that the CTA PSAP Committee includes unnamed “representatives from manufacturers, test labs, and other industry organizations” (Slide 6 of Killion).48
Mr Belt and Dr Killion have both suggested that these PSAP standards are better for the hearing industry because “existing hearing aid standards describe how to measure hearing aids, but are completely silent on what they should do.” But this is not so. For decades, FDA has used ANSI standard testing to define terms and performance standards using a common agreed-upon set of definitions, terms, and performance parameters. This standard also includes labeling. Because of the sophistication and flexibility of modern digital hearing aids, ANSI standards have never been intended to be used to describe how hearing aids should work or what they should do.
…Examination of the data for sections 4.2 and 4.3 in Category 1 reveals why hearing aids may “fail” the [CTA] voluntary standard, when in fact, they are doing exactly what hearing aids should do: provide high-frequency emphasis amplification to compensate for hearing loss for patients with a wide range of hearing losses.
…Frequency response smoothness [as stipulated by the CTA standard] is useful for listening through speakers in the real world. Hearing aid manufacturers and their component manufacturing partners have devoted considerable resources to create a targeted peak at the 2500-3500 Hz region to compensate for the loss of the ear’s natural resonance when a device or earmold is inserted into an ear canal (ie, insertion loss). The restoration of this resonance peak—which has been employed by every hearing aid manufactured throughout the world in the last several decades—maximizes the perception of fidelity and naturalness of the amplified sound. The fact that the CTA standard places a premium on smoothness at the expense of restoring the ear’s natural resonance is a stark indication of the fundamental difference between consumer electronics (eg, speakers) and hearing aid technology…
[Relative to Maximum Acoustic Output], although standard hearing aids available today will not have maximum acoustic outputs in excess of 120 dB SPL in the 2-cc coupler, devices that use “power” receivers designed for individuals with more severe hearing loss will provide levels in excess of the CTA standard levels. Again, while this would represent a “failure” to meet the [CTA] standard, it would achieve exactly what hearing aids are designed to do: compensate for hearing loss…
[Relative to self-generated noise standards], the analogous measure used in hearing aid standards is “Equivalent input noise (EIN),” which describes the difference between the coupler SPL with no input signal and the HFA gain for a 50 dB input SPL. The [CTA] measures used to derive the minimum performance standard are incomplete and do not instruct how the microphone and/or vents should be occluded during testing, what input signal level is used for comparison, nor what the appropriate volume control setting (if applicable) should be, all of which may impact findings significantly.
In summary, the [CTA] technical standards are designed for quality control purposes and to ensure sound amplification or enhancement to a user—meaning the standard only ensures the product makes sounds louder. There is no discussion of audibility, intelligibility, or assistance in hearing. Furthermore, the three examples from the standard illustrate that, while current hearing aids may fail the [CTA] standard, it is because they are designed to amplify sounds for individual hearing losses rather than provide “flat” insertion gain.
Finally, and perhaps most significantly, the standard states that the existence of this standard does not “preclude any member or nonmember of the [CTA] from manufacturing or selling products not conforming to [it].” In other words, it is purely voluntary, and members can ignore the standard with impunity. As discussed in Point #6, voluntary standards are meaningless from the perspective of ensuring safety and efficacy.
9) FDA’s Regulations and Standards Apply to More than only 6 Companies
During the Workshop, Bill Belt also stated that FDA hearing aid regulations apply to only six companies. This is incorrect. While there are six manufacturers who hold the majority of market share, there are 97 companies registered as hearing aid manufacturers with FDA. FDA’s regulatory authority extends to all 97 manufacturers and would apply to any other future hearing aid manufacturers. Notably, FDA regulations have not impeded an outpouring of technological upgrades and breakthroughs.
Furthermore, the reason that FDA regulations do not apply to the consumer electronic companies and devices currently classified as PSAPs is because these companies have labeled their products as “PSAPs,” thereby avoiding FDA regulation. Any product intended for the treatment of hearing loss constitutes a medical device under the purview of FDA. Any consumer electronic company can sell its product as a hearing aid. They would simply have to comply with the regulatory system to ensure that devices are safe and effective.
10) Hearing Aids Are Not Comparable to Eye Glasses
Hearing aids are often compared to eye glasses, but this is not an apt comparison. This comparison ignores the fact that vision and hearing (and vision loss and hearing loss) are different physiological and pathophysiological processes. Sensorineural hearing loss is similar to macular degeneration in that both affect the sensory structures. It is not akin to presbyopia, which is routinely addressed by consumers using OTC reading glasses.
Although reading glasses are generally available without a prescription, glasses to correct other vision defects do require a prescription. Most—if not all—eyeglass vendors will not distribute eyeglasses correcting near-sightedness without a prescription dated within the last year from a vision professional. For this reason, many Americans routinely have their vision checked by professionals. These eye examinations generally include checks for other medical conditions, including glaucoma, cataracts, and macular degeneration, which are identifiable by medical professionals.
By way of comparison, very few Americans visit hearing professionals for routine hearing evaluations, except for those who need or wear hearing aids. Statistics show that only 28.6% of adults in the United States (aged 20-69 years) in the last 5 years had a hearing examination, whereas an estimated 46% of the US adult population had an eye exam in the year 2015 (a much more restricted period).49,50
FDA has rejected the analogy between OTC hearing aids and OTC reading glasses. Eric Mann, MD, PhD, the clinical deputy director for FDA’s section for Ophthalmic and Ear, Nose, and Throat Devices, noted in a 2014 speech that, in addition to not providing any benefit for more serious vision problems, reading glasses do not mask any more serious vision problems (eg, glaucoma, cataracts, or macular degeneration). However, Dr Mann noted PSAPs—and, for that matter, OTC hearing aids—could mask more serious conditions. An apparent improvement in hearing could cause the consumer to skip or delay the intervention necessary to address serious underlying conditions.51
There is yet another distinction. Eyeglasses rely on a stable, mature technology. The eyeglasses sold today do not fundamentally differ from those sold centuries ago. Curved lenses correct for defects at the front of the eye by changing the point of focus on the retina. As noted above, hearing aids have undergone dramatic changes in the past decade, and more innovation is forthcoming. Hearing aids must employ sophisticated signal processing to compensate for damaged sensory and neural structures…This large, increasing technological gap between simple, stable eyeglasses and complex, evolving hearing aids is another reason why the analogy is inapt.
As Jan Metzdorrf explained during the Workshop, hearing aids are more analogous to a prosthetic limb, as both require fitting, training, and rehabilitation. Success with each is also highly dependent on cognitive abilities. These are not attributes of eyeglasses.
11) Stigma
Admittedly, hearing aids have had an associated stigma. HIA and manufacturers have worked diligently to reduce stigma through changing style, size, color, and related developments. Of course, as an industry, we welcome and celebrate the removal of stigma-related barriers to hearing aids. To that end, there are ample variations of hearing aids on the market, including the fun and flashy kinds KR Liu described during the Workshop and the barely visible kind. Consumers have a choice about whether to embrace their hearing aids or hide them, and it is not the manufacturer’s role to mandate which type of hearing aid is worn.
12) Manufacturers Do Not Trick Patients on Websites
The consumer information panel of the Workshop included some discussion of manufacturer websites allegedly “tricking” patients. Of note, Barbara Kelley of the Hearing Loss Association of American (HLAA) told of her experience on WebMD, which reportedly redirected her directly to a manufacturer website after a failed hearing screening test. We could find no such hearing screening test on WebMD. What we did encounter was a banner for one manufacturer at the top of the WebMD page that was clearly marked as an advertisement. Clicking on the banner takes the consumer out of WebMD and into the clearly identified manufacturer’s website where the consumer can take an online hearing test.
Furthermore, HIA and its manufacturers are unaware of any advertisements designed to “scare” patients. While the citation of dementia studies to entice consumers to buy hearing aids was also cited on the consumer information panel, we could not find examples of these types of advertisements (it should be noted that the NAS Report acknowledged the link between untreated hearing loss and the risk of dementia). We did find discussions of the link between hearing aids and dementia on several blogs, including both those of AARP and manufacturers, but these were not in the context of advertisements.
13) Manufacturers “Lock” Hearing Aids
A hurdle mentioned at the Workshop is that hearing aids may be “locked,” which limits transferring service to another provider. When a hearing aid is “locked,” it means that the software can be accessed only by professionals who have been trained on and dispense that particular brand.52 Locking does not limit a patient to a particular office; it restricts adjustments to those providers who have been trained on that specific device. All hearing aid manufacturers have unique software, and locking is merely a tool to ensure that only trained persons can access the controls. Of note, most practices dispense products associated with several different manufacturers, and as such, those practices have the ability to access controls across many models of hearing aids. Therefore, “locking” is not as limiting as it sounds and actually provides patients with the assurance that the hearing healthcare professional has experience with specific brands of hearing aids.
To be clear, most hearing aids are not locked, and programming information can be shared between professionals provided appropriate HIPAA guidelines have been followed.
Conclusion
HIA appreciates the opportunity to comment further and respond to the FTC Workshop on these important topics. We look forward to working with the FTC, FDA, and other stakeholders to improve the outcomes for and enhance the well-being of Americans with hearing loss.
References (Updated May 26, 2017)
-
Hearing Industries Association (HIA). RE: Hearing Health and Technology – Workshop, Project No. P171200. March 13, 2017. Available at: https://www.ftc.gov/system/files/documents/public_comments/2017/03/00029-140425.pdf
-
Abrams HB, Kihm J. An Introduction to MarkeTrak IX: A New Baseline for the Hearing Aid Market. Hearing Review. 2015;22(6):16.
-
Clason D, et al. Consumer Reports & hearing aids: Hear well in a noisy world. October 2, 2015. Available at: http://www.healthyhearing.com/report/40211-Consumer-reports-hearing-aids
-
European Hearing Aid Manufacturers Assn (EHIMA). JapanTrak 2015. Available at: http://www.ehima.com/wp-content/uploads/2016/02/JAPAN_Trak_2015-1.pdf
-
Keenan T. The state of hearing health: A study of AARP members. December 14, 2011. Available at: https://assets.aarp.org/rgcenter/general/hearing-issues.pdf
-
Granholm-Leth N. Hearing Healthcare: Market conditions better than perceived. Copenhagen: Carnegie Sector Report; January 27, 2017.
-
Lin F, Ferrucci L. Hearing loss and falls among older adults in the United States. Intern Med. 2012; 172(4)[Feb]:369.
-
Lin F, et al. Hearing loss and incident dementia. Arch Neurol. 2011;68(2):214.
-
Lerman-Garber I, et al. Sensorineural hearing loss – A common finding in early-onset Type 2 Diabetes Mellitus. Endocrine Practice. 2012; 14[July]:549.
-
Lin HC, et al., Sudden sensorineural hearing loss increases the risk of stroke: A 5-year follow-up study. Stroke. 200839(10)[Oct]:2744.
-
Rolim L, et al. Interaction between diabetes mellitus and hypertension on hearing of elderly. CoDAS. 2015;27(5)[Sept]:428. Available at: http://www.scielo.br/scielo.php?pid=S2317-17822015000500428&script=sci_arttext&tlng=en
-
Bainbridge K. Diabetes and hearing impairment: An epidemiological perspective. March 2010. Available at: http://www.asha.org/Articles/Diabetes-and-Hearing-Impairment-An-Epidemiological-Perspective
-
Calderone J. Hearing loss: No more suffering in silence? Consumer Reports. 2017;Feb. 2.
-
Timmer B. It may be mild, slight, or minimal, but it’s not insignificant. Hearing Review. 2014;21(4):30-32. Available at: https://hearingreview.com/2014/04/may-mild-slight-minimal-insignificant
-
US Food and Drug Administration (FDA). How to get hearing aids. December 7, 2016. Available at: https://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/HomeHealthandConsumer/ConsumerProducts/HearingAids/ucm181479.htm.
-
Ferrite S, et al. Validity of self-reported hearing loss in adults: performance of three single questions. Revista de Saúde Pública. 2011;45(5):824.
-
Calviti KC, Pereira LD. Sensitivity, specificity and predictive values of hearing loss to different audiometric mean values. Braz J Otorhinolaryngol. 2009;75(6):794.
-
Kochkin S. MarkeTrak VIII: 25-year trends in the hearing health market. Hearing Review. 2009;16(11):12-31.
-
Tremblay K, et al. Self-reported hearing difficulties among adults with normal audiograms: The Beaver Dam Offspring Study. Ear Hear. 2015;36(6):e290.
-
Seong Jun Choi, et al. Effect of low frequency on speech performance with bimodal hearing in bilateral severe hearing loss. Laryngoscope. 2016;126(12):2817.
-
Beck DL, Flexer C. Listening is where hearing meets brain…in children and adults. Hearing Review. 2011;18(2):30-35. Available at: https://hearingreview.com/2011/02/listening-is-where-hearing-meets-brain-in-children-and-adults
-
Beck DL, Clarke JL, Moore DR. Contemporary Issues in Auditory Processing Disorders: 2016. Hearing Review. 2016;23(4):22. Available at: https://hearingreview.com/2016/03/contemporary-issues-auditory-processing-disorders-2016
-
Consumer Technology Association (CTA). Personal sound amplification products: A study of consumer Aattitudes and behavior. CEA Market Research Report. August 6, 2014. Available at: https://www.cta.tech/cta/media/policyImages/policyPDFs/Report-Personal-Sound-Amplification-Products-A-Study-of-Consumer-Att.pdf
-
European Hearing Aid Manufacturers Assn (EHIMA). EuroTrak Denmark 2016, slide 3, http://www.ehima.com/wp-content/uploads/2016/09/EuroTrak_2016_DENMARK.pdf.
-
President’s Council of Advisors on Science and Technology (PCAST). Letter to President Obama. October 2, 2015. Available at: https://obamawhitehouse.archives.gov/sites/default/files/microsites/ostp/PCAST/pcast_hearing_tech_letterreport_final.pdf
-
Consumer Reports. Hearing aid buying guide. September 2015. Available at: http://www.consumerreports.org/cro/hearing-aids/buying-guide
-
Hearing Loss Assn of America. Medicaid regulations. January 2015. Available at: http://www.hearingloss.org/sites/default/files/docs/MEDICAID_REGULATIONS.pdf
-
Jacobsen S. US hearing aid sales gain 6 percent in June, led by Veterans: Data. Reuters, July 18, 2014.
-
Calderone J. 5 ways to cut hearing aid costs. Consumer Reports. February 2, 2017. Available at: http://www.consumerreports.org/hearing-aids/save-on-cost-of-prescription-hearing-aids
-
American Hearing Aid Associates (AHAA). Your Hearing Network. Available at: https://www.yourhearingnetwork.com
-
Gandel C. Why do hearing aids cost so much? October 3, 2016. Available at; http://www.aarp.org/health/conditions-treatments/info-05-2011/hearing-aids-cost.2.html
-
Abrams HB. You say you can make a $100 hearing aid? Go ahead! July 10, 2013. Available at: http://hearinghealthmatters.org/hearingeconomics/2013/you-say-you-can-make-a-100-hearing-aid-go-ahead
-
Hearing Loss Assn of America (HLAA). Consumer protection laws. May 2013. Available at: http://www.hearingloss.org/sites/default/files/docs/Consumer_Protection_Laws.pdf
-
Gary Swearingen. Comments presented at: FTC Now Hear This Workshop, Washington, DC;April 18, 2017.
-
Jan Metzdorff. Comments presented at: FTC Now Hear This Workshop, Washington, DC;April 18, 2017.
-
Berk B. CVS Pharmacy opens audio and optical centers. Drug Store News. April 20, 2017. Available at: http://www.drugstorenews.com/article/cvs-pharmacy-opens-audio-and-optical-centers
-
Staab W. Hearing aid market. November 17, 2015. Available at: http://hearinghealthmatters.org/waynesworld/2015/u-s-hearing-aid-market
-
US Dept of Justice. Herfindahl-Hirschman Index. July 29, 2015. Available at: https://www.justice.gov/atr/herfindahl-hirschman-index
-
American National Standards Institute (ANSI). ANSI/CTA-2051. Personal Sound Amplification Performance Criteria. January 2017.
-
21 U.S.C. § 352(a). Misbranded drugs and devices. Available at: http://uscode.house.gov/view.xhtml?req=(title:21%20section:352%20edition:prelim)
-
Smith C, Wilber LA, Cavitt K. PSAPs vs hearing aids: An electroacoustic analysis ofperformance and fitting capabilities. Hearing Review. 2016;23(7)[July]:18-24. Available at: https://hearingreview.com/2016/06/psaps-vs-hearing-aids-electroacoustic-analysis-performance-fitting-capabilities
-
Calderone J. Can PSAPs help your hearing? Consumer Reports February 2, 2017. Available at: http://www.consumerreports.org/hearing-ear-care/can-psaps-help-your-hearing
-
Taylor J. Gresham’s Law. The Encyclopedia of Central Banking. Edgar Algar Publishing;2015.
-
Cox RM, Johnson JA, Xu J. Impact of advanced hearing aid technology on speech understanding for older listeners with mild-to-moderate, adult-onset, sensorineural hearing loss. Gerontology. 2014; 60(6): 557-568.
-
Mroz M. Hearing aid technology. Healthy Hearing. Updated May 9, 2017. Available at: http://www.healthyhearing.com/help/hearing-aids/technology
-
Beck DL, Le Goff N. A Paradigm Shift in Hearing Aid Technology. Hearing Review. 2016;23(6):18. Available at: https://hearingreview.com/2016/05/paradigm-shift-hearing-aid-technology
-
Edwards B. The future of hearing aid technology. Trends Amplif. 2007. 11(1)[Mar]:31-45. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4111503
-
Killion M, Gudmundsen G. New CTA PSAP Quality Standard [Slide 6]. Presentation at: ADA Audacity Conference; San Diego. Nov. 12, 2016. Available at: http://www.audiologist.org/_resources/2016_presentations/DisruptiveInnovation-Killion.pdf
-
Health Indicators Warehouse. Recent hearing exams: adults 20-69 years. Available at: https://web.archive.org/web/20160513155408/https://www.healthindicators.gov/Indicators/Recent-hearing-exams-adults-20-69-years_748/Profile/Data
-
Vision Council Research. US Optical Overview and Outlook [Slide 6]. December 2015. Available at: https://www.thevisioncouncil.org/sites/default/files/Q415-Topline-Overview-Presentation-Stats-with-Notes-FINAL.PDF
-
Mann E. FDA regulation of hearing aids. April 18, 2017. Available at: https://www.ftc.gov/system/files/documents/public_events/1022593/mann.pdf
-
Starkey Hearing Technologies. Inspire Overview: Device Access Settings. 2015. Available at: http://www.starkeyhearingtechnologies.com/inspirehelp/st-pl/Fitting/Device_Access_Settings.htm



Hearing loss is indeed a medical problem and may indicate the need for treatment. The loss of hearing may suggest only that cerumen is present or that the patient has a tumor. Without a proper evaluation a differential diagnosis is impossible. We have seen patients who were told that they should purchase hearing aids when in fact, they had a tumor. Hearing aids should be the last option when treatment is sought for hearing loss, not the first.
I disagree that “locking” is simply a way to assure that a trained professional is involved in the programming of a hearing aid.
The true reason is that, in most cases, it ties the user to the dispenser who sells a particular brand of hearing aid. That limits the patient’s ability to seek assistance.
All public comments on the OTC initiative:
https://www.ftc.gov/policy/public-comments/initiative-690
Thank you, Tarik. These are the comments to the last FTC workshop. However, I believe the comment period for this section is closed. Stay tuned for comments regarding the June 9 NASEM dissemination meeting: https://goo.gl/lAL4Mt. Thanks again.
1) The claim: “digital platforms that perform more than 1 billion calculations per second”, is completely inaccurate.
2) As one of the 97 entities in FDA’s registered manufacturer database, we do not support the Hearing Industries Association (HIA). This organization is not representing all 97 entities. Full disclosure should list which entities are represented by this organization.
Thanks for your comments, Dean. I can’t answer for #1, but as for #2, the Hearing Industries Assn is the trade group representing hearing aid manufacturers and special equipment suppliers related to hearing healthcare. Their members (several of whom are identified in the foreword of the article) can be found by clicking on the hyperlink to HIA (hearing.org) and clicking on “Meet the Members.”