|
In a previous paper1we have described the effects of vent diameter on the gain/output characteristics of a hearing aid and the interactions between the amplified sounds and sounds that enter directly through the vent. The research suggests that clinicians should choose an optimal vent diameter for the wearers in order to minimize the occlusion effect, while preserving as much audibility and sound quality as possible.
The second implication is that one should consider the effect of venting in the prescriptive gain/output target in order to realize the intended real-ear gain. That is, one should prescribe different coupler gain settings that reflect the vent dimensions and the individual wearer characteristics so that the same real-ear output may be obtained for the same hearing loss (Author’s Note: It is possible that the optimal output target may be sensitive to different criteria like intelligibility or comfort. For example, open-fittings are designed to optimize hearing comfort relative to occlusion. In this case, the preferred high frequency gain is frequently much less than the prescribed target that has been solely based on audibility/intelligibility consideration. Since open-fitting is a case of maximum vent diameter, it is possible that different real-ear output may be desired for different vent dimensions. This possibility is being explored).
The ability to specify the correct coupler settings to achieve the intended real-ear output may reduce the need for real-ear verification and yet ensure a predictable (and hopefully desirable) real-ear output. The difficulty in achieving that goal and how Widex realizes that objective is the topic of this paper.
Challenges in Assessing Real-ear Output
Vent effect. When a hearing aid is worn in-situ, the sound pressure level (SPL) that is measured at the wearer’s eardrum is not only determined by the coupler output of the hearing aid, but is also influenced by the effect of any venting used on the hearing aid. This effect, termed the vent effect, is the difference in sound pressure level (SPL) measured at the eardrum of the hearing aid wearer consequent to the use of a vent (intentional or unintentional) on the hearing aid/earmold.

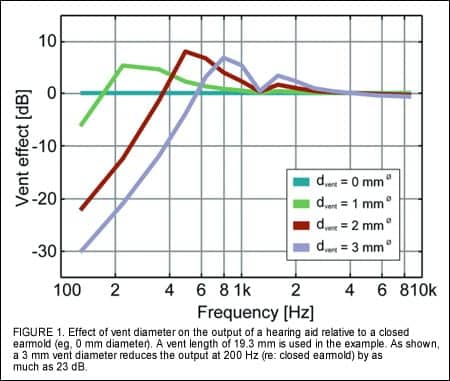
Vent diameter and length. The vent effect is controlled by the physical dimensions of the vent. It has been shown that the diameter of the vent and the length of the vent are two important parameters that affect the vent effect.2 Figure 1 shows that, as the vent diameter increases, the output in the low frequencies decreases and the frequency at the vent-associated resonance increases. The dip at 1.2 kHz is the first resonance of the receiver tubing system.
Figure 2 shows the effect of vent length on the vent effect using a vent diameter of 2 mm. As the vent length increases, the amount of low frequency output reduction decreases (eg, less effect) and the frequency of the vent-associated resonance decreases.

Leakage. Other factors may also affect the magnitude of the vent effect. For example, leakage between the hearing aid and the ear-canal wall (unintentional venting) is one such factor. Figure 3 shows the simulated output from a 10.7 mm long earmold with a 2 mm vent diameter as different amounts of leakage are introduced. The diameters of the leaks are 0.05 mm (small), 0.2 mm (medium), and 0.5 mm (large). When these leaks are added to the 2 mm vent, the resulting cross-sectional areas correspond to equivalent vent diameters of 2.2 mm, 2.6 mm, and 3.3 mm respectively. The small leak does not alter the vent effect of the 2 mm vent significantly while the large one does. This is because the equivalent size of the small leak is much smaller than that of the vent diameter. The change in slope of the medium leak is due to the greater losses from the leak than from the vent.

Residual volume in the ear canal. The residual volume between the hearing aid and the eardrum affects the magnitude of the vent effect as well. Figure 4 shows the magnitude of the simulated vent effect (2 mm vent diameter with a vent length of 19.3 mm in three sizes of residual ear canal: small (0.5 cc), normal (0.7 cc), and large (0.9 cc). As one can see, the smaller ear has a larger vent effect (eg, more low frequency reduction) and a lower magnitude of vent-associated resonance.

Middle ear compliance. The compliance (freedom of movement) of the middle ear also interacts with the vent dimensions to affect the vent effect. Figure 5 simulates and compares the vent effect of an ear with otosclerosis and an ear with ossicular discontinuity to that of a normal ear (using an earmold with a 2 mm vent diameter and 19.3 mm vent length). The ear with the otosclerosis has a less mobile middle ear and thus a lower compliance compared to a normal ear. The ear with discontinuity will have a hyper-mobile middle ear and thus a high compliance. Compared to an ear with normal compliance, an ear with a high compliance (discontinuity or a “loose” system) will have less vent effect (eg, less low frequency output reduction) and a lower vent-associated resonance. On the other hand, an ear with a low compliance (eg, “stiff” system) will have more low-frequency output reduction (eg, more vent effect) and a higher frequency at which the vent-associated resonance occurs. Furthermore, the magnitude of the vent associated resonance is also higher than the normal ear.

The previous figures show that there are at least five major variables—vent diameter, vent length, leakage, residual volume, and middle ear compliance—that control the magnitude of the vent effect. Thus, simply knowing the vent length and vent diameter does not always allow one to accurately predict the real-ear effect of a vent. Instead, the dispensing professional needs to know more about the client (such as middle ear characteristics) and how he/she is wearing the hearing aid (such as leakage). If one relies only on the coupler gain of a hearing aid and/or the nominal vent dimensions on a hearing aid/earmold to predict its in-situ output, the measured in-situ output may be very different from the intended in-situ output. This can result in unexpected losses of speech audibility and poorer sound quality.
The above reinforces the need for real-ear measurements unless the dispensing professional can reliably and accurately predict the in-situ output by incorporating the vent effect in the prescriptive gain/output target specification. Unfortunately, all the prescriptive targets assume a closed earmold in their gain/output formulation. The potential effect of venting is not included in any current fitting formulae.
Difficulty in Controlling Vent Variables
One possible reason for the non-inclusion of vent effect in prescriptive gain/output considerations is the difficulty in fully identifying (and controlling) the magnitude of each of the five variables (and possibly others). The effect of vent diameter and vent length on the output of a hearing aid is fairly predictable by noting the physical dimensions of the vent.2 However, leakage caused by slits during conventional shell-making cannot be easily controlled or measured. A slit as small as 0.05 mm has an equivalent vent diameter of 1 mm.3
Fortunately, the recent introduction of laser-fit shell-making technology (called CAMISHA) pioneered by Widex4may solve this problem. In this technology, the impression of the wearer’s ear canal is scanned by a laser to obtain an accurate “3-D image” of the impression. This virtual impression is then made into a virtual shell/earmold, the dimensions of which can be specified by the shell technician.
In the earlier versions of this technology, the virtual shell has the exact dimensions of the impression. There is no leakage between the final shell and the ear canal of the wearer. Recent development in this laser-fit shell-making technology allows the technicians to specify different “offsets” which can reduce/enlarge sections of the virtual shell, or the entire shell, by a specific percentage. Consequently, the amount of leakage in a shell/earmold may be better controlled in today’s laser-fit shell-making approach than conventional approaches. Obviously, since the goodness of the shell using laser-fit shell-making technology is dependent on the goodness of the ear impression taken by the clinician, the amount of leakage or the accuracy of the vent effect prediction is dependent on the goodness of the ear impression.
The effect of the residual volume and the middle ear compliance is more difficult to estimate and control because its magnitude is difficult to measure using clinical equipment. This means that, unless the wearer has the average residual volume and/or middle ear compliance (eg, the volume of their ear canals are the same as the normative data), it will be difficult to accurately predict the vent effect simply from knowing the physical dimensions of the vents used on the hearing aid.
These difficulties mean that in-situ vent effect cannot be easily predicted—it can only be measured directly with the hearing aid in-situ. Consequently, if one were to estimate if sufficient gain is received by the wearer, or to examine the changes in the low frequency response of the hearing aid2 or of the occlusion effect3 consequent to venting, one has to perform real-ear measurements with the hearing aids in-situ.
However, such measurements may not always be possible to perform either because the clinicians do not have the necessary equipment or the wearer may not be cooperative. Furthermore, there is a risk that the insertion of a probe-tube microphone results in additional unintended leakage which is not present during real-world use of the hearing aid.
A system that could predict the in-situ vent effect without extensive measurements is obviously desirable. In such a case, one would know the real-ear output received by the wearer without spending the extra time and resources to get that information.
In addition, if one can take the results of the vent prediction and compensate for that vent effect in the coupler gain prescription, one may ensure that more wearers receive appropriate gain regardless of the vents used (intentional and unintentional) on their hearing aids (or of their ear characteristics) on their first trial of the default hearing aid settings. Not only would it minimize the need for real-ear verification, it would also minimize the need for gain adjustment on the hearing aids to reach the prescribed gain/output target (because it would have been compensated).
Getting a Handle on Vent Variables
Although one cannot easily measure the residual volume of a wearer’s ear-canal or his/her middle ear compliance, one may not need to have the exact or precise information to predict the overall vent effect on the hearing aid output. After all, it is this overall vent effect that one is interested in and not the residual volume or middle ear compliance. If one can study the output of a vent system by adjusting its length, diameter, and amount of vent leakage on individuals with different residual volumes and middle ear compliance, one may be able to apply appropriate statistical analysis on the data and generate a model that predicts in-situ output as a function of different overall vent effects formed by different combinations of the previously listed variables.
Alternatively, one may be able to use the same model to estimate the overall vent effect the output information is known. If additional information—such as vent length, leakage, compliance, or residual volume—is available, one may be able to use the model to predict the vent diameter. Thus, modeling the output performance of a vent as a function of different vent variables may be a solution to estimating the effective vent effect experienced by a wearer.

As an example, we demonstrated in the previous paper1that the available gain before feedback on a hearing aid is systematically related to the vent diameter of the hearing aid/earmold system. Figure 6 is a simulation that shows the relationship between the maximum available gain before feedback and vent diameter. In general, maximum gain decreases as vent diameter increases. More decrease is seen in the high frequencies than in the low frequencies. In addition, the rate of decrease is more rapid in the high frequencies. With the model, one is able to estimate how much gain is available before feedback for various vent diameters, assuming a particular vent length, leakage, middle ear compliance, and residual volume.
Alternatively, the specific vent diameter can be predicted for an average individual if information on the maximum gain before feedback is available. Similar relationships between maximum gain before feedback and the other “vent” variables may also be simulated.
Relating Vent Effect Variables to Gain/Output Settings
The direct relationship between the maximum in-situ gain before feedback and the acoustic characteristics of the hearing aid shell/earmold system led Widex engineers to develop a complex model that relates the maximum in-situ gain before feedback to the vent diameter, vent length, leakage, middle ear compliance, and residual volume of the wearer’s ear-canal. Using this model, the maximum in-situ gain can be predicted if one knows the magnitude of the overall vent effect. Conversely, if one knows the maximum in-situ gain of the hearing aid, one can predict the overall vent effect. Information on the overall vent effect can be used to compensate for the changes in the in-situ gain/output from the vent effect. This ensures that wearers receive a more consistent gain/output.
Furthermore, if one assumes that the wearer is an average individual with the typical ear canal characteristics (average vent length, average leakage, average middle ear compliance, and average residual volume), one can predict the equivalent vent diameter of the wearer/vent system from the maximum in-situ gain information. Consequently, the magnitude of the equivalent vent diameter will be identical to the nominal (or physical) vent diameter if the wearer is indeed “average.” Otherwise, the magnitude of the equivalent vent diameter will likely deviate from the nominal vent diameter in a manner predicted from the interactions of the five factors listed in the previous paragraphs.
How AISA Works
One of the key features in the new Inteo hearing aid is the patent-pending algorithm called the Assessment of In-Situ Acoustics (AISA). This algorithm estimates the overall vent effect of the wearer and his/her hearing aid system in order to predict the equivalent vent diameter and compensate for its effect on signal processing. The steps involved in this algorithm include:
1. Estimation of maximum in-situ gain before feedback. The first part of the AISA algorithm is the feedback test. This is part of the 2-step fitting process for all Widex Senso and Inteo hearing aids. During the mandatory feedback test, modulated sinusoids are generated within the hearing aid and used as signals to drive the feedback paths. The output of the hearing aid from these inputs is measured by the microphone system in order to estimate the maximum in-situ gain before feedback.
2. Estimation of overall vent effect. The maximum gain that is measured during the feedback test is used to estimate the overall vent effect experienced by the wearer and the hearing aid system. This is done by comparing the available gain measured after the feedback test to the modeled available gain for various modeled vent diameters. Figure 7 compares the measured in-situ gain (top) and the modeled gain (bottom) for various vent diameters with a length of 19.3 mm. The vent diameter associated with the modeled available gain (eg, closest in magnitude to the measured available in-situ gain across most frequencies) corresponds to the best estimate of the in-situ vent effect.

3. Reporting of “Equivalent Vent Diameter.” The estimated overall vent effect may be reported in a number of ways. Considering that most clinicians are familiar with the effect of vent diameters, the overall vent effect is reported as the equivalent vent diameter (in mm). This means the overall vent effect has the equivalent characteristics of an X mm vent diameter when it is worn by the average individual. It is important to remember that this equivalent vent diameter includes the influence of all five variables discussed previously that contribute to the overall vent effect. Thus, it may not have the same value as the nominal or physical vent diameter unless the wearer has the average ear canal characteristics.

Figure 8 is a scatter-plot comparing the equivalent vent diameters to the nominal (or physical) vent diameters measured in 8 subjects (or 16 ears) with normal middle ears. Data points that fall on the diagonal dotted line would suggest perfect matches. One can see that the match between the estimated vent diameters and the nominal vent diameters is excellent (within 0.5 mm). Differences that are noted probably reflect the effect of the residual volume, vent length, leakage, and middle ear compliance on the prediction. When these effects are considered in isolation, vents that are used in small ears (or small residual volume) will have estimated diameters that are larger than the nominal values; while larger ears (or large residual volume) have estimated vent diameters that are smaller than the nominal values. Likewise, a longer-than-average vent length would yield a smaller estimated vent diameter than a shorter vent length.
4. Calculation of “true hearing loss.” The sensogram is an estimation of the person’s hearing loss with the hearing aid in-situ. From that regard, the magnitude of the sensogram has considered the effect of the residual volume and vent dimensions.5Gain specified using the sensogram is more accurate than gain specified using audiometric thresholds. This is because audiometric thresholds are typically done with headphones or insert earphones which not only give a different residual volume but are also “closed.”
In the fitting of the Inteo, the accuracy of the sensogram fitting is further improved with the use of the AISA algorithm. The measured sensogram is corrected with the magnitude of the overall vent effect in order to estimate the “true” hearing loss of the wearer—the hearing loss that is independent of the influence of the vent dimensions. Consequently, the measured sensogram may be different from the corrected sensogram especially in the low frequencies.
5. Gain assignment based on “true” hearing loss or corrected sensogram settings. Once the true hearing loss is calculated, the fitting software will assign gain based on the true hearing loss using Widex’s proprietary targets while assuming a closed earmold.
6. Compensation for vent effect is made in final gain assignment. Gain that is assigned based on the “true” hearing loss is modified to compensate for the in-situ vent effect that will be experienced when the hearing aids are worn. The gain in the low frequency region is increased by an amount proportionate to the total vent effect. Future refinements will also include gain modification at the appropriate frequencies to minimize potential phase cancellation.
The objective is to ensure an optimal real-world in-situ gain for all vent (intentional and unintentional) conditions. In other words, an optimal real-ear gain should be observed for all individuals with the same hearing loss regardless of differences in their vent diameters, vent lengths, leakage, middle ear compliances, or residual volumes. This also means that the coupler output of hearing aids selected for different individuals with the same hearing loss may be different because of the differences in any or all of the above said variables for the vent effect.
Clinical Implications
The AISA algorithm automatically estimates the equivalent vent effect of the wearer’s hearing aid/vent system. Furthermore, it appropriately compensates for the vent effect to ensure that the desired real-ear gain and optimal sound quality are realized. Figure 9 summarizes the steps discussed in this paper.

There are several points that one should be aware of in order to ensure accurate results from the use of this feature. First, AISA takes the sensogram thresholds and corrects them according to the results of the overall vent effect estimation. This assumes that the measured sensogram has included the overall vent effect. On the other hand, if the clinician does not perform the sensogram but simply enters the audiogram thresholds as the measured sensogram, AISA will underestimate the true hearing loss of the wearer in the low frequencies and yield a gain setting that has less low frequency gain than the hearing loss (and vent effect) requires. Consequently, one must perform the sensogram reliably and accurately so AISA can accurately estimate the true hearing loss.
It is also important to obtain a reliable and accurate feedback test. This is because the estimation of the overall vent effect is based on the magnitude of the maximum available in-situ gain before feedback. Any inaccurate estimation, such as performing the test in a noisy place, sudden movement, or noise in the environment, may confound the results and make the estimation invalid. In addition, because AISA is a model-based algorithm that is based on average ears, atypical ears and ears that have undergone surgery, etc, may result in a “strange” estimation. While we are confident in this estimation, additional studies are being conducted to establish its clinical applicability.
The immediate benefit of the AISA algorithm is a gain prescription that has considered most, if not all, of the acoustic effects brought forth by intentional and unintentional venting. This ensures more consistent gain use among hearing aid wearers despite potential differences in their real-life vent effects. Hopefully, this will lead to consistent audibility and a consistently better sound quality.
There are other benefits of the AISA algorithm. This algorithm allows clinicians to estimate the equivalent effect of atypical vent configurations, such as the reverse horn vent.6By reporting the vent effect as the equivalent vent diameter (in mm), the clinician can compare the equivalent vent diameter with the nominal vent diameter on the hearing aid/earmold or with the recommended vent diameter to assess the adequacy of the nominal vent diameter in reducing the occlusion effect. Nominal vent diameter that appears to be significantly larger than the equivalent vent diameter suggests that the “real-world, in-situ” vent used by the wearer may be smaller than what appears. This may explain why the nominal vent diameter may not yield the expected relief in occlusion effect. This information allows clinicians to adjust the vent dimensions (ie, length and diameter) to further improve the wearers’ perception of their own voice during vocalization.
Summary
Accurately measuring the overall vent effect in a wearer’s hearing aid/earmold system is important to ensure that the wearer fully enjoys the optimal frequency output characteristics required for their hearing loss. The AISA algorithm on the Inteo provides an easy and accurate way to assess the overall acoustic effect of the hearing aid/earmold system in-situ. In addition, it is designed to provide all the necessary gain adjustments to ensure that the wearers enjoy a smooth and natural sound quality.
References
1. Kuk F, Keenan D. How do vents affect hearing aid performance? The Hearing Review. 2006;13(2):34-42.
2. Lybarger S. Earmolds. In: Katz J, ed. Handbook of Clinical Audiology. Third edition. Baltimore: Williams and Wilkins;1995:885-910.
3. Kuk F, Keenan D, Lau C. Vent configurations on subjective and objective occlusion effect. J Am Acad Audiol. 2005;16(9): 747-762.
4. Cortez R, Dinulescu N, Skafte K, Olson B, Keenan D, Kuk F. Changing with the times: applying digital technology to hearing aid shell manufacturing. The Hearing Review. 2004;11(3):30-38.
5. Ludvigsen C, Topholm J. Fitting a wide range compression hearing instrument using real-ear threshold data: A new strategy. In: Kochkin S, Strom KE, eds. High Performance Hearing Solutions, Vol 2. The Hearing Review. 1997;[Suppl]4(11):37-39.
6. Kuk F, Keenan D, Lau C, Dinulescu N, Cortez, Keogh P. Real-world performance of a reverse horn vent. J Am Acad Audiol. 2005;16(9): 653-661.