
Hearing aids for people with a severe-to-profound hearing loss (SPHL) must be chosen more carefully than those for people with milder degree losses. This article presents a literature review of factors influencing hearing aid selection and use for the SPHL population, as well as how the new Widex Super440 device was designed by leveraging this information.
Today’s digital hearing aids fit individuals with a wide range of hearing loss from near-normal to profound. While it is intuitive that hearing aids for a severe-to-profound hearing loss (SPHL) need to deliver higher output and gain compared to those designed for a milder loss, the reality is that fitting SPHL hearing aid wearers requires considerably more than just higher gain/output.
Indeed, the unique psycho-physical abilities of people with SPHL—and the potential interaction between the higher gain demand and other processing features on the hearing aids—require special considerations from hearing aid designers and the clinicians fitting the devices. In this paper, we will review the challenges behind the development of a hearing aid for this population and discuss how the Widex Super440 is designed to meet those challenges.



Francis Kuk, PhD, is executive director of the Widex Office of Research in Clinical Amplification in Lisle, Ill; Hanne Pernille Andersen, PhD, is a member of the Audiological Research Department and Lars Baekgaard, MSc, is a research engineer at Widex A/S, Vaerloese, Denmark. Correspondence can be addressed to Dr Kuk at
Why Do People with a Severe-to-Profound Hearing Loss Require Special Attention?
It is generally acknowledged that people with SPHL have a more impaired auditory system than people with a milder loss. Furthermore, these people may also be conditioned to an amplification scheme that hinders their immediate acceptance of modern nonlinear amplification.
Consequences of a more impaired auditory system. The severe-to-profound (SP) nature of the SPHL implies that acoustic signals have to be presented at a high level before they can be audible. On the other hand, the level where loudness discomfort (LDL) occurs does not increase as linearly as threshold. This means that listeners with a SPHL typically have a reduced dynamic range of hearing of 30 dB or less.1 In the most severe cases, people with a SPHL are also more likely to have “dead” regions2 in the high frequencies that either are non-responsive to acoustic stimulation, or, when stimulated, result in a distorted input to the auditory system. This may degrade speech intelligibility.2,3A drastic decrease in frequency selectivity is also seen in this group of listeners.4 The decrease in selectivity worsens as the degree of hearing loss increases. It also worsens as the level of the input increases from a spread of excitation along the basilar membrane.5 This poses a dilemma. People with a SPHL need a high output level to hear the stimuli; however, their ability to resolve the stimulus difference decreases as the stimulus level increases. This may be another physiological reason why speech recognition in noise decreases as the overall input level increases beyond a comfortable level.3,6In general, people with a SPHL have acceptable temporal resolution when acoustic stimuli are presented at a sufficiently high and comfortable level.7 However, the temporal resolution becomes poorer as the sensation level of the stimulus decreases. This again creates a dilemma because a higher sensation level would also increase the spread of masking and reduce spectral specificity.
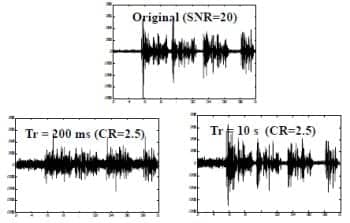
Figure 1. Effect of release time on the temporal waveform. Note that the waveform is smeared in the 200 ms case compared to the 10 s case.
Thus, a consequence of the need to provide high gain (in order to achieve audibility and optimal sensation level) is the further decrease in spectral resolution. This means SPHL individuals are even more susceptible to noise interference. Dubno and Dirks8 showed that the speech scores of people with a severe-to-profound hearing loss were much worse than that predicted from their loss of sensitivity alone. People with a SPHL are more dependent on a good SNR for optimal speech understanding.9The decrease in frequency selectivity and the somewhat intact temporal resolution may be a reason why people with a SPHL are more reliant on temporal cues for speech identification.10 Because these cues are helpful in providing voicing and amplitude information,11,12 they should be preserved as much as possible.
Conditioning to analog linear hearing aids. Historically, the majority of people with a SPHL have been aided with linear hearing aids that use either peak clipping or compression limiting for output control. While such hearing aids may be acceptable for inputs at a moderate level, their use is limited at both the low and high input levels without volume control adjustment. Low-level sounds are not audible; high-level sounds decrease the specificity of stimulation and risk “noise” exposure with prolonged listening.13
For example, OSHA guideline recommends that no person should be exposed to sounds at 120 dBSPL for more than 8 minutes.14 Yet, it is not uncommon to measure real-ear output exceeding 130 dBSPL from a hearing aid for this group of wearers. Obviously, this group of listeners may have no choice but to risk the potential of further damage to their hearing.
One way to minimize the risk of hearing damage is to ensure that the maximum output of the hearing aid is set to a low level. This is done with either peak clipping or broadband compression limiting. Compression limiting leads to additional temporal distortion of the output waveform, while peak clipping leads to spectral distortion, which may be habituated by some SPHL listeners.
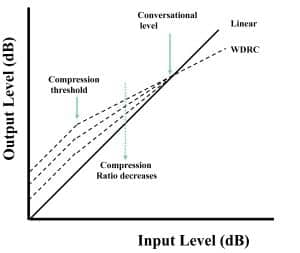
Figure 2. Hypothetical input-output curve to show that at a fixed compression threshold and gain for conversational input, a lower compression ratio often results in lower gain (output) for softer sounds.
Thus, one should expect that the loudness relationship of everyday sounds and the temporal waveform of the input may have been altered for these listeners. Any attempts to provide a new form of amplification for this group of listeners must also consider this human factor.
Considerations in Hearing Aids for People with SPHL
People with a SPHL need hearing aids that provide high gain for soft and conversational sounds, but low gain at higher inputs in order to avoid spectral and temporal distortion so that temporal cues within the input signal may be preserved. They need carefully managed hearing aid output to minimize the risk of additional hearing loss. They need to better utilize the residual neurons and a better signal to noise ratio (SNR) to offset the loss in spectral resolution. Many will also need to unlearn from their previous linear hearing aid experience.
1) Achieving high gain within a narrower dynamic range. Hearing aids can be designed with active feedback cancellation and advanced compression to take full advantage of the patient’s residual hearing (dynamic range).
Using active feedback cancellation. A hearing aid that delivers a high gain/output must ensure its stability. Thus, an active feedback cancellation algorithm is critical for these hearing aids. In addition to providing a higher maximum available gain, the feedback system must be able to accurately differentiate a true feedback sound from a non-feedback sound such as a musical note, and be able to respond with appropriate speed to changes in the feedback path.15
Using multiple-channel, slow-acting wide dynamic range compression (SA-WDRC). A WDRC hearing aid provides more gain for low input and less gain for high input levels. This ensures greater audibility, maximizes comfort, minimizes the risk of distortion, and reduces the risk of overexposure to loud sounds than a linear hearing aid.16 Indeed, research in the last 10 years supports the use of WDRC hearing aids for people with a severe to profound hearing loss.17-19
The time constants on a WDRC hearing aid may affect the effectiveness of the circuit for this population. A WDRC hearing aid that uses a fast attack and release time (ie, fast-acting) reduces the peak-to-peak intensity difference and can smear the temporal envelope of the input signal20,21 and consequently make speech understanding more difficult.12,19 However, some researchers reported benefits of a FA-WDRC in restricted situations.22,23
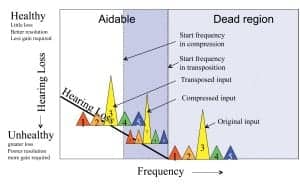
Figure 3. Hypothetical comparison between the efficacy of a frequency transposition algorithm and a frequency compression algorithm for someone with a severe hearing loss in the low-mid frequency and a severe-to-profound loss in the highs
As illustrated in Figure 1, the temporal waveform may be better preserved using WDRC with long time constants (ie, slow-acting [SA] compression) than with short time constants (ie, fast-acting [FA] compression).24 Ringdahl et al25 showed that 88% of the subjects preferred the Widex P38 super power hearing aids (3-channel, SA-WDRC) to their own linear hearing aids in a study. This suggests that SA-WDRC can be beneficial to people with a severe-to-profound hearing loss.
The reduced dynamic range of people with a SPHL would suggest a high compression ratio (CR). However, the fact that speech fluctuates within an intensity range of 30 to 40 dB at any vocal effort level26 suggests that linear processing or WDRC with a low CR could place the full range of speech into the residual dynamic range of listeners—even those with SPHL. In reality, many studies that demonstrated the successful use of FA-WDRC used a low CR (<2:1) (eg, Barker et al27 and Keidser et al28). This is because temporal waveform distortion is minimized with the low CR. On the other hand, a lower CR would also mean that less gain is available at a low input level (Figure 2). The use of a low compression threshold and SA-WDRC could allow the use of higher gain and lower effective CR.24
The level of the low frequency input (being the most intense) often controls the action of the compressor in a single-channel WDRC device. This affects the output in all frequency regions and could compromise audibility of the higher frequency sounds. Multiple channels allow independent gain adjustment and provide better specificity in signal processing. Algorithms such as amplitude compression, noise reduction, feedback cancellation, directional microphone, and output limiting may be enhanced with more channels.
On the other hand, too many channels may not be desirable when a high CR is used.19 One must consider the type of WDRC (SA versus FA) and the compression characteristics in selecting the nonlinear hearing aid for people with a SPHL. Ideally, a multichannel SA-WDRC that provides high gain, low CT, and a CR lower than 3:1 is desirable.
2) Achieving optimal use of residual surviving neurons. Hearing aids for SPHL typically had a limited bandwidth. In some cases, it was limited to <5000 Hz in the high frequencies. Although hearing aids with an extended bandwidth have become available,29 these hearing aids have less than 110 dBSPL OSPL because of the trade-off between the output and bandwidth. Thus, some high frequency regions may not be able to receive adequate (or any) output even though an active feedback cancellation system is available.
However, in many cases, the degree of hearing loss is so profound that the registered responses are actually mediated by nearby frequency regions or result in severe distortion. Amplification of such regions may result in a distorted sound percept or poorer speech understanding.3 Thus, focusing on making the most of the surviving neurons by optimizing output in the lower frequencies may be a better strategy than attempting to apply amplification in the high-frequency region.
Fitting target for severe-to-profound hearing loss. To better utilize the remaining frequencies in a SPHL, the gain target has to prescribe more gain in the low-to-mid frequency regions than for a milder loss (eg, NAL-RP30). For example, while the gain prescription for a mild-to-moderate hearing loss is about 1/3 to1/2 the degree of hearing loss, the gain prescription for a SPHL is typically 1/2 to 2/3 the hearing loss. Similarly, it is desirable that the OSPL in the low-to-mid frequencies of such hearing aids be high to allow a high low-frequency output.
Using frequency lowering. Frequency lowering moves information from the high frequency areas to a lower frequency area where there are surviving neurons for its decoding.31 There are two main forms of frequency lowering: frequency transposition (FT) and frequency compression (FC). In frequency transposition, the unaidable high frequency is moved to a frequency region that is typically one to two octaves lower. In frequency compression, the frequency area above a start frequency is compressed so that they are fitted within a narrower frequency region. In both cases, the higher frequency sounds are heard as a lower frequency substitute.
Various authors have demonstrated the potential benefit of this type of signal processing algorithm for people with a severe-to-profound loss in the high frequencies but mild-to-moderate loss in the low-mid frequencies.32-34
There may be theoretical advantages for a FT algorithm over a FC algorithm for those with a moderately severe to severe loss in the low-to-mid frequency (ie, the SPHL group). Figure 3 shows that, because FC needs to squeeze the unaidable frequencies into a region of aidable hearing, a relatively high compression ratio and a low start frequency will be needed. Otherwise, even though FC is used, the high frequency sounds may still not be audible or not resolvable (because of the poorer resolution resulting from the severe degree of hearing loss).
On the other hand, the transposed sound from a FT algorithm is more likely to be in a frequency region of better hearing than the FC. This makes it more likely to be audible and be resolvable. Gou et al35 have reported the efficacy of FT on people with a severe loss in the low-mid frequencies.
3) Compensating for poorer temporal and frequency resolution. The high gain requirement of this group for optimal audibility and temporal resolution means that the output of the hearing aids has to be high. Furthermore, the spread of excitation on the basilar membrane at high input, coupled with the already-reduced frequency resolution, makes it necessary that a more favorable SNR be available.
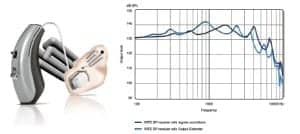
Figure 4. Left: Illustration of the SUPER440 RITE with the receiver in the concha earmold along with the convoluted sound bore “Output Extender.” Right: Output of the SUPER440 with the typical sound bore (dark blue) and Output Extender sound bore (light blue).
Using directional microphones. Directional microphones are also beneficial for people with a severe degree of hearing loss. Ricketts et al36 applied the AI-DI calculation and concluded that people with a severe degree of hearing loss could also benefit from the technology. Ricketts and his colleagues37 subsequently reported 14% to 17% improved speech identification with a directional microphone over an omnidirectional microphone.
There are many considerations in designing a directional hearing aid for people with SPHL. First, hearing aids with a directional microphone typically have less low-frequency sensitivity than their omnidirectional counterparts. This can result in a loss of loudness and voicing information for people with SPHL who may have only residual hearing in the low frequencies.
One can achieve comfortable loudness by amplifying the lower frequencies and/or keeping the hearing aid in an omnidirectional mode in quiet, switching to the directional mode only when there is noise. The latter is the basis of the fully adaptive directional microphone.38
To further improve the specificity of directional functions, multiple channel adaptive directional microphones may be used so they may maintain the omnidirectional pattern in some channels and the directional in others. Indeed, one of the many advantages of a multichannel adaptive directional microphone is seen in noisy background where the noise is restricted to a narrow frequency range.39
The loss of loudness also originates from a second source. A directional microphone reduces its sensitivity to sounds from the sides and back. Indeed, Kuk et al40 showed as much as 40% decrease in speech recognition scores when soft speech was presented from the back of a fixed directional microphone.
There are several techniques to ensure audibility of speech sounds presented from the back. One is to have an adaptive directional microphone with an activation threshold (from omnidirectional to directional) above 50 to 55 dBSPL so it will not unnecessarily attenuate useful soft sounds from the back. Another option is to integrate acoustic scene analysis within the directional microphone system so the directional microphone will only be activated if the input from the back is noise.41
A more recent approach to ensure audibility/intelligibility of speech from the back is the use of a microphone mode that has a reverse-cardioid polar pattern. In this case, the user can select to use this microphone mode when he/she has identified that desirable sounds are presented from the back and undesirable sounds from the front. Kuk and Keenan42 showed a 7 to 8 dBSNR improvement in such conditions with a reverse cardioid microphone over an omnidirectional microphone and a directional microphone.
Using noise reduction (NR) algorithms. The effectiveness of NR algorithms has not been reported extensively for the SPHL population. Keidser et al43 found that real-world use of a combined NR and directional microphone program yielded greater comfort in noisy situations for people with SPHL. However, because of the reduced output, the authors recommended that these features only be utilized in a separate program when sufficient audibility of speech sounds can be ensured.
Classic noise reduction algorithms differ by the amount of gain reduction in the frequency channel as a function of the input level, the SNR detected at that frequency channel, and the frequency importance of that channel.44 Some newer algorithms also consider the user’s degree of hearing loss and may increase gain in the mid-frequency regions in order to maximize the speech intelligibility index (SII-based NR) for the wearer in that environment.45 These differences could be critical for those with SPHL.
It is unclear which form of noise reduction is most optimal for people with a SPHL. On the one hand, the classic form of NR may bring the output of the hearing aid to below the hearing thresholds of the SPHL individuals, making both speech and noise softer and more comfortable with or without improving intelligibility. On the other hand, SII-based NR could ensure audibility, but risk comfort and may not be preferable to those with SPHL. More research is necessary to elucidate this point.
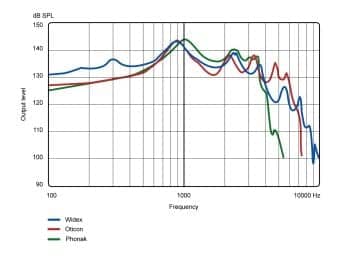
Figure 5. Comparison of coupler output of the Widex SUPER440 (in blue) to two other leading super-power hearing aids in red and green (ear-simulator data).
4) Overcoming the “linear” experience. Listeners with a SPHL typically wear linear BTE hearing aids, or nonlinear hearing aids with essentially linear characteristics, with an omnidirectional microphone and no noise reduction.
Many of the newer nonlinear hearing aids include feedback cancellation algorithms, directional microphones, noise reduction algorithms, and frequency lowering. Some BTE devices also have a “digital pinna” that compensates for the pinna effect to enhance front/back localization. Some devices also utilize receiver-in-the-ear technology (RITE).
The use of these features may produce dramatic changes in the loudness perception for someone with a SPHL. These listeners will likely require a period of adjustment to the newer nonlinear devices. However, the use of the conventional “acclimatization” program on most modern hearing aids would not be appropriate because it typically reduces the initial recommended gain and not adjustment to the different sound percept.
Using laser shell/earmold technology. RITE hearing aids extend the receiver from the body of the hearing aid to the wearer’s concha. This allows for more room to be devoted to other hearing aid components. This means the potential for a smaller size and a more cosmetically appealing appearance from the use of thin-wire.29 A potential drawback to the use of RITE hearing aids in SPHL listeners is the absence of the significant tubing resonances found in traditional BTE hearing aids.29 It may not be possible to electronically compensate for this loss in SPHL listeners because of insufficient output from the hearing aids. Lack of sufficient output around 1000 Hz would significantly affect the loudness and clarity of the amplified sounds.
One approach to compensate for the loss of tubing resonance is through acoustic modification of the sound bore. Using laser-fit shell making technology introduced by Widex,46 one may extend the length of the sound bore by creating a labyrinth within the earmold/shell that houses the RITE receiver to result in a resonance peak around 1000 Hz (or at other optimal frequencies, within limits). Widex has introduced this and called it the “Output Extender”—a receiver/mold that is available for Widex’s super-power hearing aids (Fusion HP and Super SP). Figure 4 shows an illustration of the Output Extender earmold (left) and a diagram with the shift of the resonance peak generated by the Output Extender (right).
Acclimating to nonlinear processing and high-frequency information. A complaint from some experienced wearers with SPHL when nonlinear hearing aids are first introduced is that “sounds are not loud enough.”47 In some individuals, one may also observe a decrease in speech identification scores when a frequency response that de-emphasizes the low-mid frequencies and emphasizes the high frequencies is used.48
An immediate reaction of some is to “linearize” the fitting by reducing the gain of the hearing aid for soft sounds and increasing the gain for loud sounds. In addition, the user frequency-response is reset to what the listener is accustomed while the directional microphone and noise reduction algorithms are deactivated. While this may please the wearer initially, it does not give the wearer the opportunity to acclimate to the new sound percept so he/she may receive its full benefit. In practice, a period of acclimatization is needed for this group of individuals to the new signal processing.28,49-51 Indeed, evidence is emerging that people with SPHL can acclimate to and benefit from nonlinear processing, directional microphone, and noise reduction like people with a milder loss.43
In order that listeners with SPHL may acclimate to the new sound perception offered by nonlinear hearing aids, clinicians must first make sure that the recommended nonlinear hearing aids meet the minimum criterion of audibility for soft sounds across as broad a frequency range as possible. They should also make sure that the adaptive features (such as adaptive directional microphone and noise reduction) on the hearing aids, while reducing loudness by necessity, would not compromise audibility. Once that is ascertained, the clinicians should counsel the wearers of the changes in the hearing aid technology, set right expectations for the new hearing aids, and insist that the wearers try out the new settings for a period of 2 to 4 weeks. The wearers’ experience should be discussed during the follow-up visits to determine if adjustment may be necessary.47
Clinicians who are less willing to insist on their patients trying out a new setting may utilize the multiple-memory capability on most modern nonlinear hearing aids. In addition to the recommended settings, one may program into a memory a set of electroacoustic settings that mimic the wearers’ own hearing aids. They can then be instructed to compare the relative preference for each memory in their daily lives. Hopefully, the opportunity to compare between settings will encourage them to adapt to the new settings sooner.
Business NOT as Usual: Designing a Super Power Hearing Aid
The new Widex Super440 is a small wireless RITE hearing aid that uses a 675 battery. It is based on the same C-ISP signal processing platform as the Clear440 hearing aids. Thus, it has all the features and benefits of the clear hearing aids.52 The following summary lists how the features on the Super440 have addressed the special considerations raised in the earlier sections.
- High gain with minimal distortion risk. The Super440 has an OSPL90 of 138 dBSPL and a maximum gain of 78 dB. It allows the fitting of individuals with PTA in excess of 100 dBHL. It is a 15-channel SA-WDRC with a compression limiter to prevent output saturation distortion. Two adaptive systems—the TruSound Stabilizer system and the TruSound Softener system—manage sudden changes (as brief as <1 ms) in the input signal to ensure maximum and consistent intelligibility of speech and listening comfort in all listening conditions. An active feedback cancellation system is used to ensure the maximum stable gain in many situations.
Two compression regions, low level compression (LLC) and high level compression (HLC), are utilized to separately manage inputs above and below 50 dBHL. The unique compression ratios for each region help to maintain the temporal waveform of the output over a wide input range. Additionally, it minimizes the risk of extended exposure to high output. - Maximizing the use of residual neurons. A proprietary gain prescription formula that attempts to optimize intelligibility is used. An Output Extender (OE) is available as an option to extend the resonance peak to below 1000 Hz to allow maximum utilization of the surviving neurons.
The bandwidth of the Super440 is broad (7000 Hz) to allow flexibility in fitting hearing losses of various degrees and configurations. In addition, it has as much as 135 dBSPL output at 300 Hz (Figure 5). A frequency transposition algorithm (Audibility Extender) is available to move the unaidable high frequencies to lower frequencies. - Compensating for poorer SNR. The Super440 has a fully adaptive 15-channel directional microphone (HD-Locator) that has an activation threshold at 55 dBSPL and a speech tracker to make sure that quiet speech presented from the back is not attenuated. A digital pinna is available to provide front/back localization cues. In addition, a Reverse Focus microphone allows the wearer to change the microphone to focus on sounds presented from the back. In addition, assistive listening devices like the M-DEX and the TV-DEX allow better enjoyment of sounds from TV, MP3 player, cell phone, etc at an enhanced SNR.53
There are two noise reduction algorithms on the hearing aid—the classic noise reduction algorithm and the SII-based Speech Enhancer (SE) algorithm. Clinicians may experiment with each algorithm to decide on the most efficient one for the individual SPHL wearer. - Considering previous linear experience. Proper counseling is important for some people with a SPHL to fully acclimate to nonlinear hearing aids. However, it is also recognized that some wearers will not acclimate easily to the default program. Thus, Widex has a “classic” program on the Super440 that essentially uses linear gain (less gain for soft and more gain for loud) with an omnidirectional microphone and classic noise reduction. Wearers may compare the classic program and the default program in their real-life situations to select the best one to use. Obviously, the programming software is flexible enough to allow clinicians to select any combinations of the electroacoustic characteristics that are the most optimal for the wearer.
Conclusion
Hearing aids for people with a SPHL must be chosen more carefully than those for people with a milder degree of hearing loss. They must be given all that technology offers in order to maximally utilize the fewer residual neurons that they have.
References
- Pascoe D. Clinical measurements of the auditory dynamic range and their relation to formulas for hearing aid gain. In: Jensen J, ed. Hearing Aid Fitting: Theoretical and Practical Views. Proceedings from the 13th Danavox Symposium; Copenhagen, Denmark: Stongaard Jensen; 1988:129-151.
- Moore B. Dead regions in the cochlea: Diagnosis, perceptual consequences, and implications for the fitting of hearing aids. Trends Ampl. 2001;5(1):1-34.
- Ching T, Dillon H, Byrne D. Speech recognition of hearing-impaired listeners: Predictions from audibility and the limited role of high-frequency amplification. J Acoust Soc Am. 1998;103:1128-1140.
- Faulkner A, Rosen S, Moore B. Residual frequency selectivity in the profoundly hearing impaired listener. Brit J Audiol. 1990;24:381-392.
- Gulick L, Gescheider G, Frisina R. Hearing: Physiological Acoustics, Neural Coding, and Psychoacoustics. Oxford University Press. NY; 1989;161-187.
- Studebaker G, Sherbecoe R. Speech recognition at higher than normal speech and noise levels. J Acoust Soc Am. 1995;97(5):3358.
- Rosen S, Faulkner A, Smith D. The psychoacoustics of profound hearing impairement. Acta Oto-Laryngol. 1990;[Suppl]469:16-22.
- Dubno J, Dirks D. Associations among frequency and temporal resolution and consonant recognition for hearing-impaired listeners. Acta Oto-Laryngol. 1990;[Suppl] 469:23-29.
- Boothroyd A, Springer N, Smith L, Schulman J. Amplitude compression and profound hearing loss. J Speech Hear Res. 1988;6:362-376.
- Van Tasell D, Soli S, Kirby V, Widin G. Speech waveform envelope cues for consonant recognition. J Acoust Soc Am.r. 1987;82:1152-1161.
- Grant K. Encoding voice pitch for profoundly hearing impaired listeners. J Acoust Soc Am. 1987;82:423-432.
- Boothroyd A. Signal processing for the profoundly deaf. Acta Oto-Laryngol. 1990;[Suppl]469:166-171.
- Macrae J. Temporary and permanent threshold shift caused by hearing aid use. J Speech Hear Res. 1995;38: 949-959.
- Occupational Safety and Health Administration (OSHA). Occupational Noise Exposure; Hearing Conservation Amendment; Final Rule. Federal Register. 1993;448(46):9737-9785.
- Kuk F, Jessen A, Klingby K, Henningsen L, Peeters H, Keenan D. Changing with the times: Additional criteria to judge the effectiveness of active feedback cancellation algorithm. Hearing Review. 2006;13(9): 38-48.
- Moore B. Signal processing to compensate for reduced dynamic range. In: Beilin J, Jensen G, eds. Recent Developments in Hearing Instrument Technology. Proceedings of the 15th Danavox symposium. Scanticon, Denmark; 1993:147-166.
- Flynn MC, Dowell RC, Clark GM. Aided speech recognition abilities of adults with a severe or severe-to-profound hearing loss. J Speech Lang Hear Res. 1998;41(2):285–299.
- Souza P, Bishop R. Improving speech audibility with wide dynamic range compression in listeners with severe sensorineural loss. Ear Hear. 1999;20(6):461-470.
- Souza P, Jenstad L, Folino R. Using multichannel wide-dynamic range compression in severely hearing-impaired listeners: effects on speech recognition and quality. Ear Hear. 2005;26(2):120-131.
- Drullman R, Festen J, Plomp R. Effect of temporal envelope smearing on speech reception. J Acoust Soc Am. 1994;95(2):1053-1064.
- Verschuure J, Maas A, Stikvoort E, de Jong R, Goedegebure A, Dreschler W. Compression and its effect on the speech signal. Ear Hear. 1996;17:162-175.
- Davies-Venn E, Souza P, Brennan M, Stecker G. Effects of audibility and multichannel wide dynamic range compression on consonant recognition for listeners with severe hearing loss. Ear Hear. 2009;30(5):494-504.
- Marriage JE, Moore BCJ, Stone MA, Baer T. Effects of three amplification strategies on speech perception by children with severe and profound hearing loss. Ear Hear. 2005;26(1):35-47.
- Kuk F. Rationale and requirements for a slow acting compression hearing aid. Hear Jour. 1998;51(6):45-53,79.
- Ringdahl A, Magnusson L, Thelin L, Edberg P, Israelsson B. Clinical evaluation of a digital power hearing aid. Hearing Review. 1999;7(3):59-64.
- Pearsons K, Bennett R, Fidell S. Speech Levels in Various Noise Environments. EPA Report #600/1-77-025. Washington DC: Environmental Protection Agency (EPA); 1977.
- Barker C, Dillon H, Newall P. Fitting low ratio compression to people with severe and profound hearing losses. Ear Hear. 2001;22(2): 130-141.
- Keidser G, Dillon H, Dyrlund O, Carter L, Hartley D. Preferred low- and high-frequency compression ratios among hearing aid users with moderately severe to profound hearing loss. J Am Acad Audiol. 2007;18(1):17-33.
- Kuk F, Baekgaard L Considerations in fitting hearing aids with extended bandwidth. Hearing Review. 2009;16(10):32-39.
- Byrne D, Parkinson A, Newall P. Hearing aid gain and frequency response requirements for the severely/profoundly hearing impaired. Ear Hear. 1990;11(1):40-49.
- Braida L, Durlach N, Lippmann R, Hicks B, Rabinowitz W, Reed C. Hearing aids–a review of past research on linear amplification, amplitude compression, and frequency lowering. ASHA Monographs. 1979;19:1-114.
- Auriemmo J, Kuk F, Lau C, Marshall S, Thiele N, Pikora M, Quick D, Stenger P Effect of linear frequency transposition on speech recognition and production of school-age children. J Am Acad Audiol. 2009;20(5):289-305.
- Kuk F, Keenan D, Korhonen P, Lau C. Efficacy of linear frequency transposition on consonant identification in quiet and in noise. J Am Acad Audiol. 2009;20(8):465-479.
- Wolfe J, John A, Schafer E, Nyffeler M, Boretzki M, Caraway T. Evaluation of nonlinear frequency compression for school-age children with moderate to moderately severe hearing loss. J Am Acad Audiol. 2010;21(10):618-628.
- Gou J, Smith J, Valero J, Rubio I. The effect of frequency transposition on speech perception in adolescents and young adults with profound hearing loss. Deafness and Education Intl. 2011;13:17-33.
- Ricketts T, Henry P, Hornsby B. Application of frequency importance functions to directivity for prediction of benefit in uniform fields. Ear Hear. 2005;26(5):473-86.
- Ricketts T, Hornsby B. Directional hearing aid benefit in listeners with severe hearing loss. Int J Audiol. 2006;45(3): 190-197.
- Ricketts T. Directional hearing aids. Trends Ampl.f. 2001;5(4):139-176.
- Kofoed A, Kuk F, Peeters H, Lau C, Crose B. Performance of a fully adaptive multiband directional microphone in a low- pass noise. Poster presented at: American Auditory Society annual meeting, March 2009, Scottsdale, Ariz.
- Kuk F, Keenan D, Lau C, Ludvigsen C. Performance of a fully adaptive directional microphone to signals presented from various azimuths. J Am Acad Audiol. 2005;16(6): 335-349.
- Kuk F, Keenan D, Lau C. Preserving audibility in directional microphones: implications for adults and children. Hearing Review. 2005;12(11):62-68.
- Kuk F, Keenan D. (2012) Efficacy of a reverse cardioid directional microphone. J Am Acad Audiol. 2012;23(2). In press.
- Keidser G, Hartley D, Carter L. Long-term usage of modern signal processing by listeners with severe or profound hearing loss: a retrospective survey. Am J Audiol. 2008;17(2):136-146.
- Kuk F, Ludvigsen C, Paludan-Muller C. Improving hearing aid performance in noise: challenges and strategies. Hear Jour. 2002;55(4):34-46.
- Kuk F, Paludan-Muller. Noise management algorithm may improve speech intelligibility in noise. Hear Jour. 2006;59(4):62-65.
- Cortez R, Dinulescu N, Skafte K, Olson B, Keenan D, Kuk F. Changing with the times: applying digital technology to hearing aid shell manufacturing. Hearing Review. 2004;11(3):30-38.
- Kuk F. Adaptation to enhanced dynamic range compression (EDRC)—Examples from the SENSO P38 hearing aid. Sem Hear. 2001;22(2):161-171.
- Convery E, Keidser G. (2011). Transitioning hearing aid users with severe and profound loss to a new gain/frequency response: benefit, perception, and acceptance. J Am Acad Audiol.22(3):168-180.
- Kuk F, Potts L, Valente M, Lee L, Picirrillo J. Evidence of acclimatization in persons with severe-to-profound hearing loss. J Am Acad Audiol. 2003;14(2):84-99.
- Flynn M, Dowell R, Clark G. Aided speech recognition abilities of adults with a severe or severe-to-profound hearing loss. J Speech Lang Hear Res. 1998;41(2):285-299.
- Convery E, Keidser G, Carter L. Transitioning Hearing Aid Users With Severe and Profound Hearing loss From Linear to Nonlinear Amplification: Three Case Studies. Austral and New Zeal Jour Audiol. 2008;30(1):73-85.
- Kuk F, Crose B, Kyhn T, Mørkebjerg M, Rank M, Nørgaard M, Föh H. Digital Wireless Hearing Aids III: Audiological Benefits. Hear Review. 2011;18(8):48-56.
- Andersen H, Holm H, Rose S. Cognitive ergonomics: Making it simple. Hear Review. 2012;19(2):40-46.
Citation for this article:
Kuk F., Andersen H., Baekgaard L. Hearing Aids for Severe-to-Profound Losses: Business as Usual? Hearing Review. 2012;19(03):38-48.


