
Pediatrics | February 2014 Hearing Review
By Karen L. Anderson, PhD, and Jane R. Madell, PhD
By providing information about hearing aid retention strategies throughout early childhood, collecting accurate information about daily hearing aid wear challenges, and working as a team, it should be possible to find appropriate strategies to keep children “on the air,” facilitating listening, language, and learning.
Adjusting to hearing aid use can be very difficult for infants, children, and their families. Putting hearing aids on a child requires accepting the fact that the child has a hearing loss. Even when families accept the fact of the hearing loss, putting on hearing aids and taking a child out in public and to family gatherings can be difficult. Many parents will find excuses to limit hearing aid use. As children get older, they sometimes also find excuses to limit hearing aid use.
A number of factors limit a child’s hearing aid use. Children may remove the hearing aids or they may not stay on the child’s ears. All children remove hearing aids at one time or another. Suddenly hearing when a child has been in a quiet world can be a surprise, causing a child to remove the hearing aid. Young children may remove hearing aids for a number of reasons. Infants are exploring their world and may remove hearing aids as part of exploration. Toddlers may remove hearing aids exploring their environment and may attempt to take them apart. Preschoolers may remove them as part of a power struggle with parents, especially when having a temper tantrum.
One significant problem is the difficulty of keeping hearing aids on the head. With infants, the pinna is soft and will often bend causing hearing aids to fall off. Using a pediatric ear hook and short earmold tubing, the hearing aid may fall off if not fit well. Both infants and older children encounter problems keeping hearing aids on the head when they are active. When hearing aids flop around or fall off, parents may feel that it is easier to remove them while the child is active. Whenever the hearing aid is off—even for a few minutes—the child is missing language and listening input, which should be avoided.

Figure 1. Data from the Jones and Launer study1 showed that 40% of children wear their hearing aids only 4 hours or less each day and only 10% achieve full-time hearing aid wear.

Figure 2. Number of hours hearing aids are worn by severity of hearing loss.
Survey
In an effort to explore the problem of hearing aid retention, the Pediatric Hearing Aid Retention Project Survey was developed by the authors and sent to parents and audiologists to determine what retention devices they find most useful.
A total of 286 parents and 101 audiologists responded to the survey. Products were listed and all respondents were asked to rate each product on the following:
- Effectiveness;
- Child safety;
- Durability;
- Ease of use;
- Keeping the device on and working (parent questionnaire); and
- Level of compliance by families (audiology questionnaire).
Results 
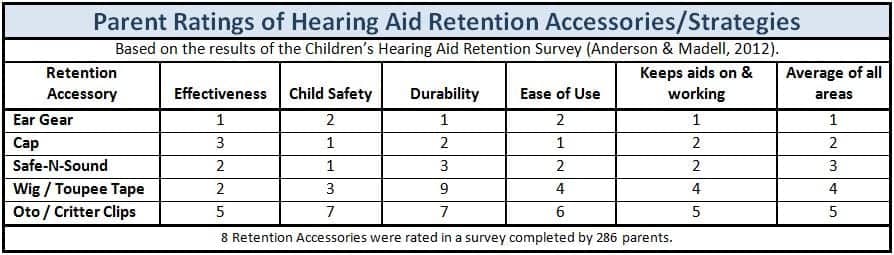
Table 1 illustrates the combined responses provided by parents and audiologists for rating hearing aid retention accessories. The results of the survey clearly illustrated that the families who use retention devices typically have a significantly different view of the effectiveness and safety of the devices as compared to how audiologists rate these features.
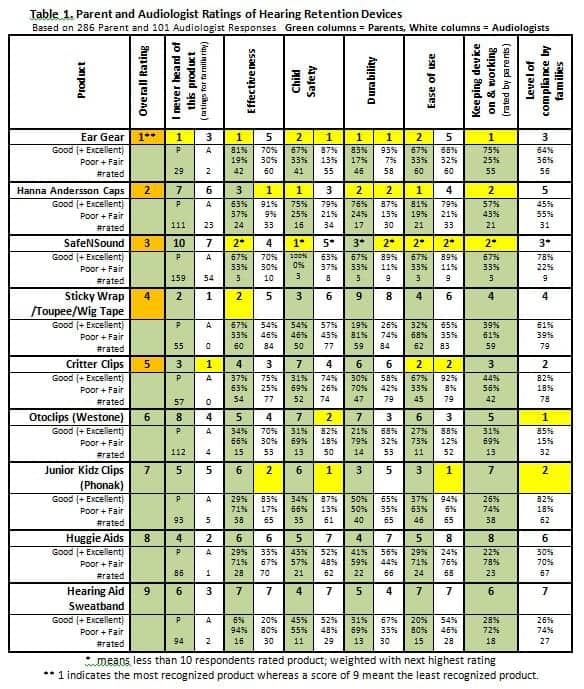
Table 1. Parent and Audiologist Ratings of Hearing Retention Devices, based on 286 Parent and 101 Audiologist Responses. Gray columns = Parents, White columns = Audiologists. *means less than 10 respondents rated product; weighted with next highest rating; **1 indicates the most recognized product whereas a score of 9 meant the least recognized product.
Acoustic Transparency Study
A valid concern exists about the acoustic transparency of hearing aid retention accessories that cover the microphone of hearing devices. The acoustic transparency of Ear Gear, Hanna Andersson pilot cap, Silkawear cap, and the Hearing Henry Headband was determined via electroacoustic evaluation with an AudioScan analyzer and Phonak Piconet2 hearing aid. With the volume control taped in a position just below full on, the response 50, gain at 50 dB and 60 dB SPL, SSPL90, frequency range, and harmonic distortion were obtained for the hearing aid alone, the hearing aid on a false ear (to obtain the pinna effect), and the hearing aid with each accessory.
The Ear Gear was positioned as it would be when typically worn. The Hanna Andersson cap and Silkawear cap were placed so that the material of the cap that would typically be over the ear was wrapped tightly over the hearing aid case and microphone to simulate typical wear. The Hearing Henry Headband, if worn appropriately, will not cover a hearing aid microphone. However, active children can easily dislodge the placement of a headband. Therefore, the Hearing Henry Headband was placed over the hearing aid microphone to simulate acoustic response if the headband placement was inappropriate.
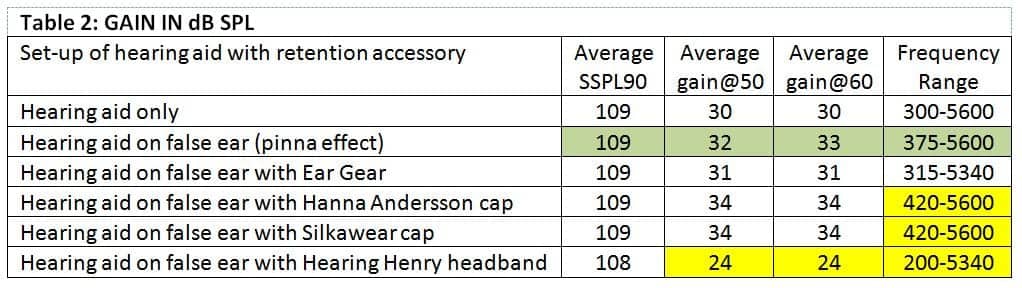
Table 2. Frequency response of the conditions listed in Table 2.
Harmonic distortion results were within 1% of the hearing aid only condition. Gain and frequency range response are shown in Table 2. Ear Gear minimally changed the frequency range (low and high) when compared to the response when the hearing aid alone was on the false ear. The caps reduced the reception of low frequency sound only. The Hearing Henry Headband increased the low frequency range when the microphone was covered. The gain with Ear Gear and both caps was within 1-2 dB of that found with the hearing aid on the false ear. Ear Gear decreased gain by 1 dB and the caps increased gain by 1-2 dB. Only the Hearing Henry Headband, when positioned across the microphone, reduced gain (8-9 dB gain reduction).
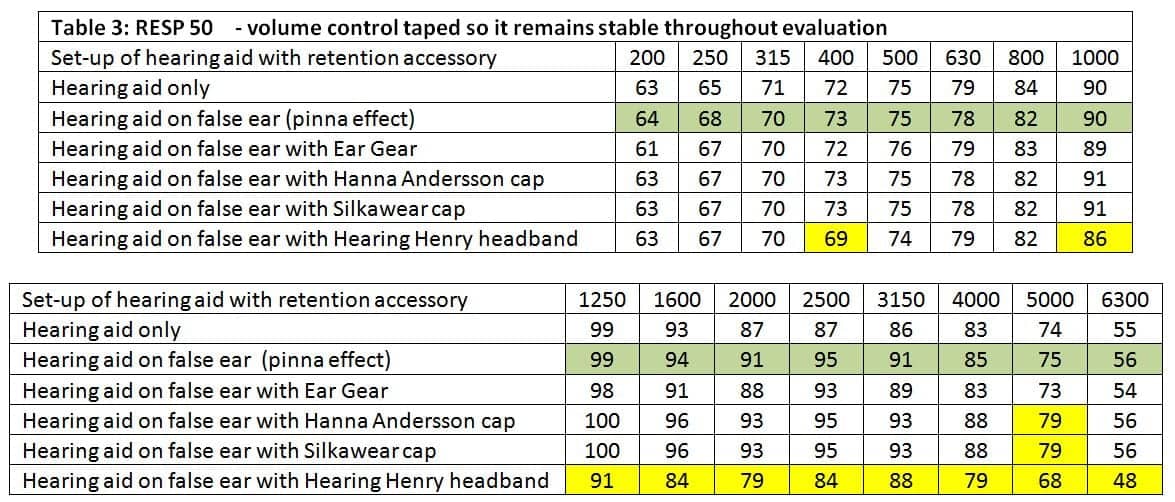
Table 3. Gain and frequency range response for hearing aid (HA) only, hearing aid on false ear (with pinna effect), and four hearing aid retention products. Ear Gear minimally changed the frequency range, while the caps reduced reception of low frequency sounds only.
Table 3 illustrates the frequency response of all conditions. Ear Gear and Hanna Andersson and Silkawear caps had responses within 0-3 dB of the hearing aid worn on the false ear for most of the frequencies tested. Interestingly, both caps increased the frequency response at 5000 Hz by 4 dB. The Hearing Henry Headband worn inappropriately over the hearing aid microphone significantly impacted the high frequency response.
Based on the acoustic transparency evaluation results, Ear Gear is considered to be acoustically transparent, and the caps tested significantly affected the response only at 5000 Hz and that was only a 4 dB difference. The Hearing Henry Headband, and possibly all headbands, when worn inappropriately has the potential to significantly decrease gain and frequency response.
Comments by Audiologists
The survey solicited comments by audiologists to the question: In regards to working with families, what have you tried with success? The following provide a summary of the comments received:
- Parent to parent support.
- Audiologist working with early intervention providers to help establish hearing aid wear goals for the family and provide support.
- Using interpreters and connecting them with families of a similar background.
- Help families understand their child’s hearing loss and what their child is missing by not having their hearing aids on.
- Counseling in a way that makes the hearing devices meaningful to the family.
- Discussing the family’s specific challenges with them.
- Providing real-world examples of strategies to increase wear time.
- Having the family come in for frequent data logging checks.
- Not one thing works with each family. Time and patience. You must have a good working relationship to keep them coming back.
- Thinking outside the box and understanding what is holding them up gets you on the right path.
- Work with a partner agency to provide a Mother’s Day Out situation so someone else will keep the hearing aids on to show the parents it can be done.
- Encouragement by multiple audiologists as families come in for regular appointments.
- A “to do” list with achievable measures and a date of completion usually prior to our next appointment (eg, complete Early Intervention evaluation, go to dispenser to pick up hearing aids, etc).
- Keeping in close communication and not closing the door simply because the family has barriers or is taking a longer time to make choices.
Discussion

Table 4. Parent ratings of hearing aid retention accessories/strategies (8 products/strategies were rated in a survey completed by 286 parents).
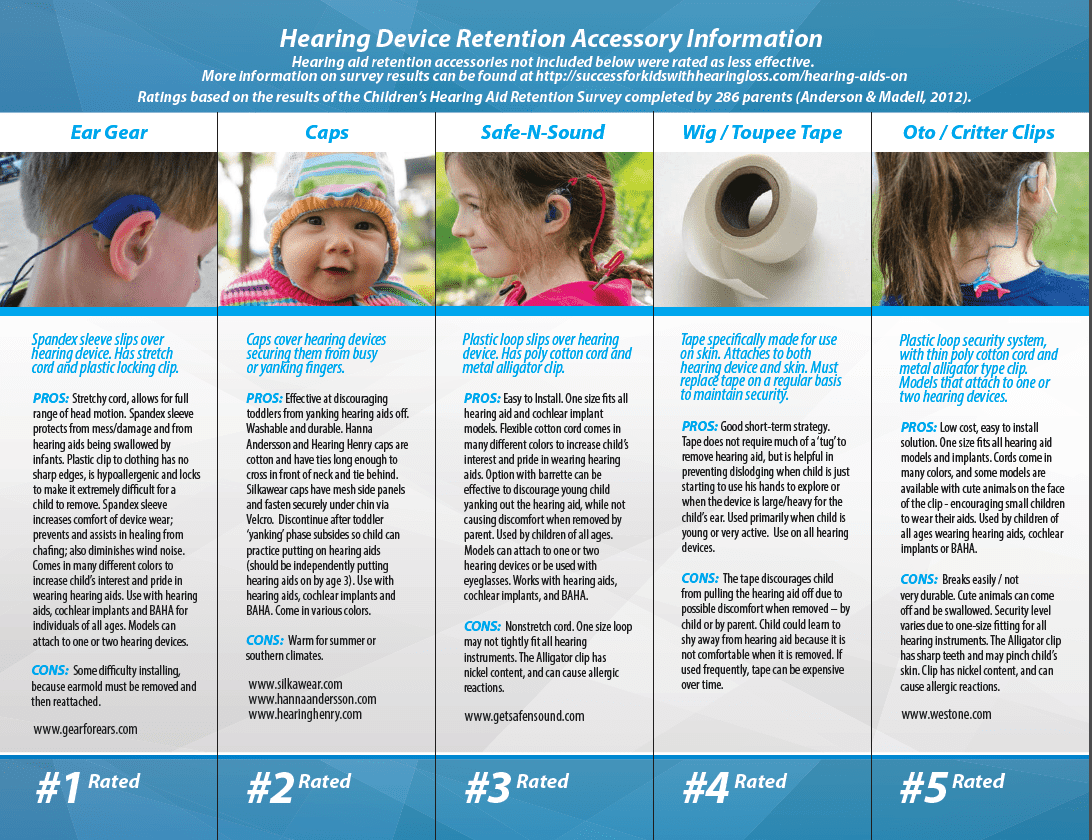
Ear Gear, Hanna Andersson Caps, and SafeNSound received the best ratings by both parents and audiologists (see Table 4 for parent ratings). Clips (Critter Clips, Phonak Junior Kidz Clips, Otoclips) received high scores from audiologists—but not parents.
The difference in parent and audiologist ratings is significant and may indicate that audiologists and parents are not communicating well. Audiologists may not be aware of the problems parents experience with hearing aid retention devices and may therefore be making recommendations without real practical information to draw upon.
Also of significance is the number of parents who reported never having heard of a product. Of 286 parents responding to the survey, 57 never heard of Critter Clips, 29 never heard of Ear Gear, 111 never heard of Hanna Andersson Caps, 94 never heard of hearing aid sweat bands, 86 never heard of Huggie Aids, 93 never heard of Phonak Junior Kidz Clips (this may be explained by the fact that it is only distributed with Phonak aids), 159 never heard of SafeNSound, 139 never heard of Superseals, and 53 never heard of Sticky Wrap/Toupee/Wig Tape. Audiologists had heard of most products. Of 101 audiology respondents, 23 had not heard of Hanna Andersson Caps and 54 had not heard of SafeNSound.
Figures 3a-b. The authors have created three brochures designed respectively for families of children ages 0 to 12 months, 12 to 24 months, and 2 to 5 years old that can be accessed and downloaded at:
http://successforkidswithhearingloss.com/hearing-aids-on or www.JaneMadell.com
If parents are having a problem with hearing aid retention, it would seem to be critical to have information about all products available and their effectiveness. Providing this information should be the responsibility of the audiologist. Parents should be told initially and at subsequent visits to the audiologist that there are devices available to assist in retention and given specific information to assist in selecting the appropriate product for a particular child. The audiologist needs to question the parents about problems with hearing aid retention at each visit as an important part of management of the young child with hearing loss.
One outcome of the survey was the development of free brochures for families of young children ages 0-12 months, 12-24 months, and 2-5 years (an example is shown in Figures 3a-b). These three brochures can be downloaded for use by audiologists and agencies serving families of infants and toddlers from http://successforkidswithhearingloss.com/hearing-aids-on and at www.JaneMadell.com. More information on hearing aid retention survey results, acoustic transparency, and strategies can be found at http://successforkidswithhearingloss.com/hearing-aid-retention.
By providing information about hearing aid retention strategies throughout early childhood, collecting accurate information about daily hearing aid wear challenges, and working as a team, it should be possible to find appropriate strategies to keep children “on the air” facilitating listening language and learning.
References
1. Jones C, Launer S. Pediatric Fittings in 2010: The Sound Foundations Cuper Project. A Sound Foundation Through Early Amplification. Warrenville, Ill: Phonak. Available at: http://successforkidswithhearingloss.com/wp-content/uploads/2012/01/Phonak-Data-Logging-Study-2010.pdf
2. Stovall D. Teaching Speech to Hearing Impaired Infants and Children. Springfield Ill: Charles C. Thomas; 1982
Karen L. Anderson, PhD, is an educational and pediatric audiologist, and is director of Supporting School Success for Children with Hearing Loss, Plymouth, Minn. She is also the author of many test instruments and materials, such as the SIFTERs, CHILD, LIFE, and ELF. Jane R. Madell, PhD, has a consulting practice in pediatric audiology, and is an audiologist, speech-language pathologist, and LSLS auditory verbal therapist. With 40+ years of professional experience, she has published four books and written numerous book chapters and journal articles.
Original citation for this article: Anderson K, J Madell. Improving hearing and hearing aid retention for infants and young children. Hearing Review. 2014;21(2): 16-20.



