The majority of cochlear implant recipients develop new bone formation that adversely affects long-term hearing preservation, according to a study appearing in Radiology. An article summarizing the study appears on the Radiological Society of North America (RSNA) website.
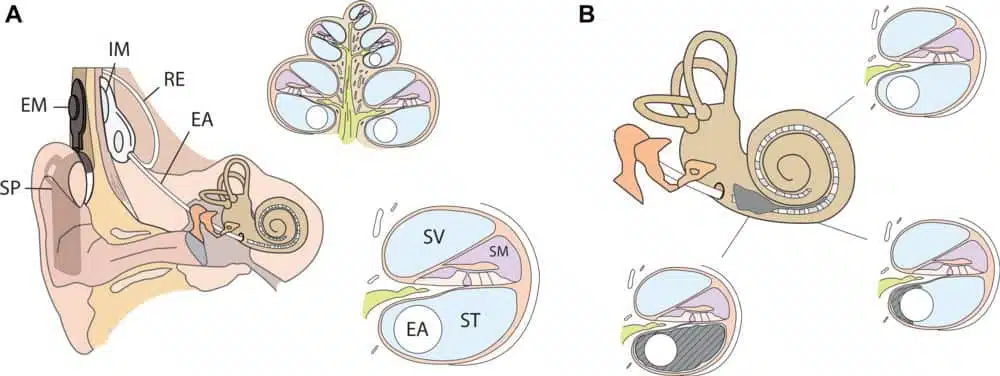
Cochlear implantation is a well-established means to treat severe hearing loss. The device consists of an external part that sits behind the ear and a second part surgically implanted under the skin that stimulates nerves in the cochlea, a fluid-filled, spiral structure in the inner ear that transmits sound across sensory nerves to the brain. Cochlear implants don’t restore normal hearing, but they can help a person recognize words and better understand speech.
While complications from cochlear implants are rare, post-mortem studies have linked them with inflammation, fibrosis, and new bone formation. The potential clinical implications of new bone formation make it desirable to visualize and possibly prevent development, but in-vivo—or within the body—detection has not yet been described.

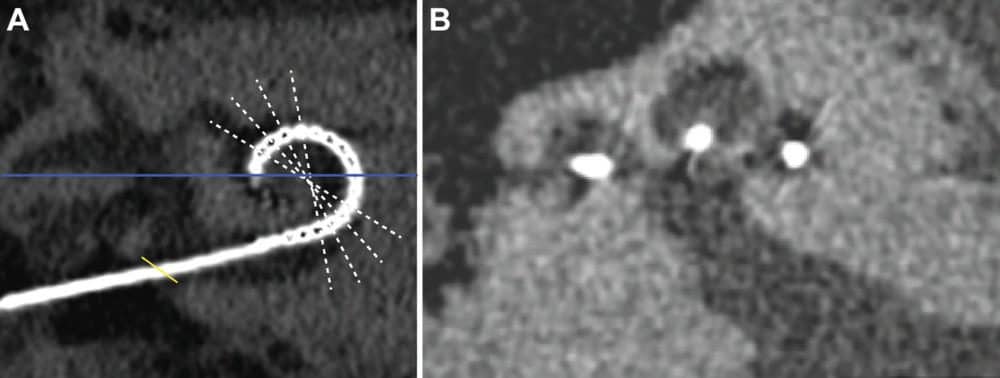
“Such subtle changes are challenging to visualize in vivo, in particular in the vicinity of a metallic implant causing artifacts on computed tomography images,” said study co-lead author Floris Heutink, MD, MSc, from the Department of Otorhinolaryngology at Radboud University Medical Center (Radboudumc) in Nijmegen, the Netherlands. “However, through the new availability of an ultra-high-resolution CT scanner, we were encouraged to investigate this.”
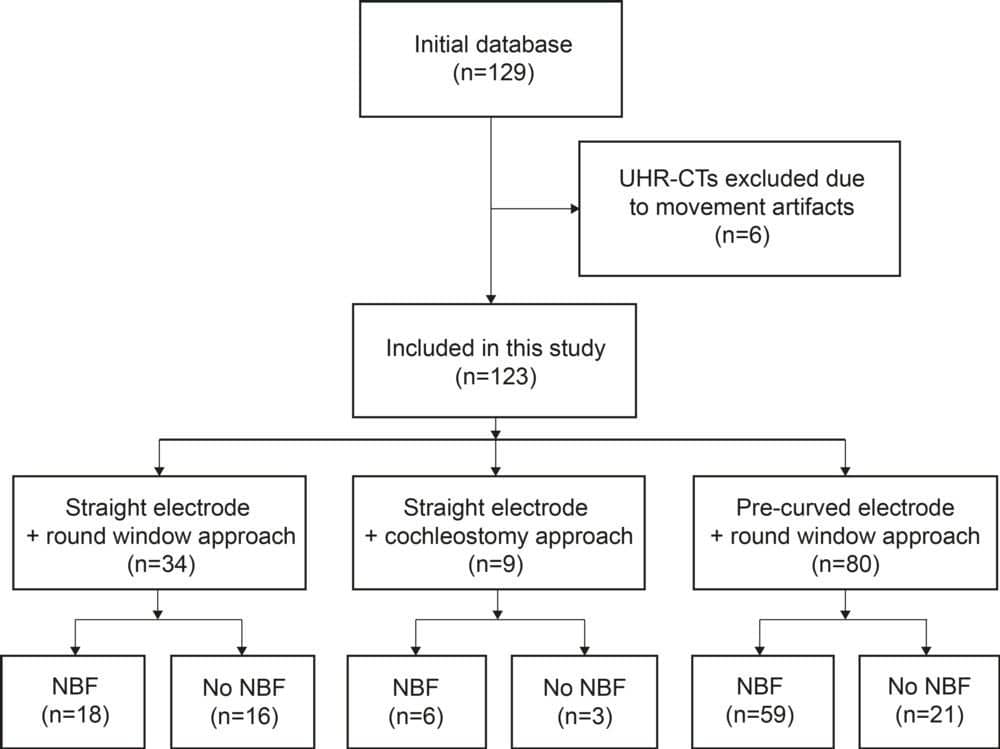
Dr Heutink and colleagues used ultra-high spatial resolution CT (UHRCT) to assess new bone formation and its implications in 123 patients with cochlear implants.

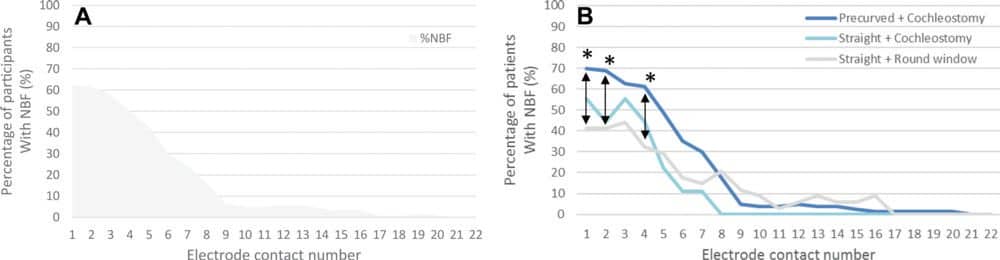
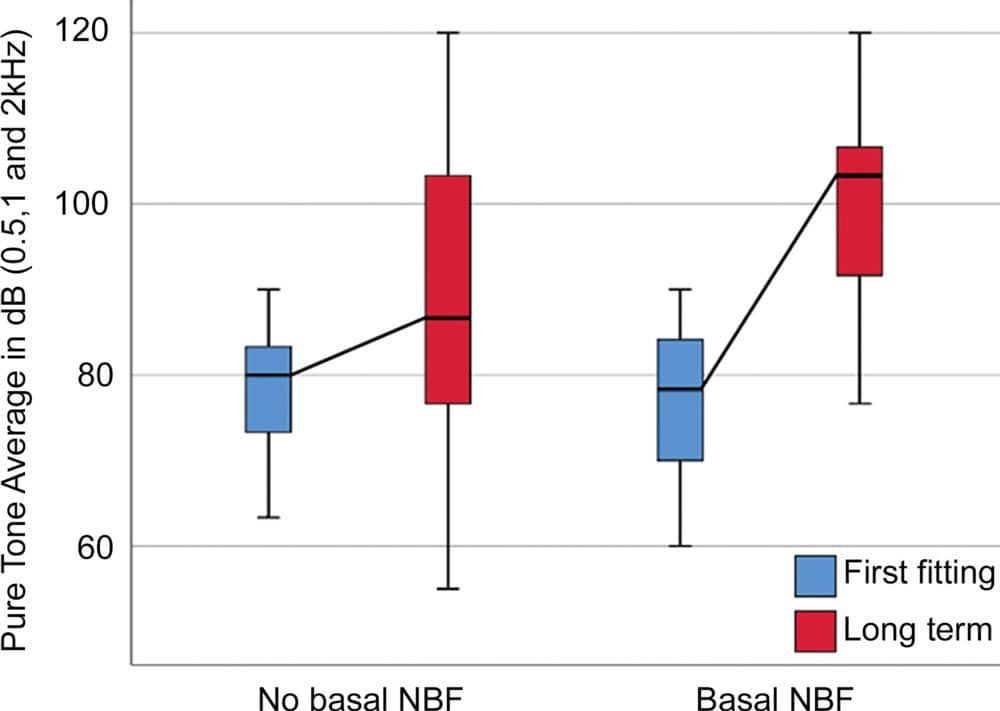
The researchers were able to detect new bone formation in vivo using UHRCT. Of the 123 patients, 83 (68%) had new bone formation, predominantly located at the base of the cochlea, within four years of implantation. Long-term residual hearing loss was significantly larger in the group with new bone formation.

“As indicated by our study, there is a correlation between new bone formation and long-term residual hearing loss,” said study co-author Berit M. Verbist, MD, PhD, from the Departments of Radiology at Radboudumc and Leiden University Medical Center in Leiden, the Netherlands.
New bone formation around the cochlear implant electrode has a number of negative consequences due to its effects on the device and the structures surrounding it. It can affect the spread of electrical current within the cochlea, leading to complex device fitting, channel interaction, and poorer overall hearing outcome. It could also complicate future therapies such as gene therapy to restore cochlear function.
“Last but not least, new bone formation may complicate reimplantation surgery,” Dr Verbist said.
The researchers noted that improvements in design and surgical techniques have made cochlear implantation available for an increasing number of people with severe to profound hearing loss. This increase in patients makes a method for detecting and monitoring new bone formation in vivo more urgent than ever. Still, many remaining questions have to be answered, Dr Heutink said, before the detection of new bone formation in an individual patient would have therapeutic consequences.
“This technique will be a valuable tool to gain insight into occurrence, time course, and the pathophysiology of this process and maybe used to evaluate still-to-be-developed treatments against new bone formation,” he said.
Original Paper: Heutink F, Klabbers TM, Huinck WJ, et al. Ultra-high-resolution CT to detect intracochlear new bone formation after cochlear implantation. Radiology. 2021;000:1-8.
Source: RSNA, Radiology
Images: RSNA



