

Anthony Ricci, PhD, professor of otolaryngology-head and neck surgery, Stanford University School of Medicine.
A study in mice conducted at the Stanford University School of Medicine has shown that a commonly used antibiotic can be modified to eliminate the associated risk of hearing loss. Treatment with aminoglycosides, the most commonly used class of antibiotics in the world, is often a lifesaving necessity. However, an estimated 20% to 60% of all patients who receive these antibiotics suffer partial or complete hearing loss as a side effect of treatment.
In a study article that was published online in the January 2, 2015 edition of the Journal of Clinical Investigation, Stanford University researchers report that they have developed a modified version of an aminoglycoside that works effectively in mice without the risk of causing deafness or kidney damage, another common side effect. According to a news announcement from Stanford University, the researchers hope to test versions of the modified antibiotic in humans as soon as possible.
“If we can eventually prevent people from going deaf from taking these antibiotics, in my mind, we will have been successful,” said Anthony Ricci, PhD, professor of otolaryngology-head and neck surgery at Stanford University School of Medicine, and co-senior author of the study. “Our goal is to replace the existing aminoglycosides with ones that aren’t toxic.”
Revising a Common Antibiotic Takes Time
A revised version of sisomicin, a popular aminoglycoside antibiotic, reportedly took four years. The newly patented version of the antibiotic that was derived from sisomicin is called N1MS. The research team used N1MS in their study and found that it cured urinary tract infection in mice just as well as sisomcicin, without causing deafness. Co-senior author Ricci says their results offer a promising new approach to generating a new class of novel antibiotics that are not toxic to the ear (ototoxic).

Alan Cheng, MD, associate professor of otolaryngology-head and neck surgery, Stanford University School of Medicine.
In 2007, Ricci joined forces with Alan Cheng, MD, associate professor of otolaryngology-head and neck surgery, to explore the idea of creating improved versions of these antibiotics based on a simple idea stemming from Ricci’s research on the biophysics of how hearing works within the inner ear. Ricci is an expert on the process by which sound waves open ion channels within the sensory hair cells of the inner ear, allowing their conversion to electrical signals that eventually reach the brain.
Because aminoglycoside antibiotics cause deafness by killing these non-regenerating sensory hair cells, Ricci approached Cheng with a proposal to investigate whether they could prevent the molecules of the antibiotics from entering the cells’ channels.
“As a clinician-scientist, I treat kids with hearing loss,” said Cheng. “When a drug causes hearing loss it is devastating, and it’s especially disturbing when this happens to a young child as they rely on hearing to acquire speech. “When I came to Stanford seven years ago from the University of Washington, I was exploring the angle that maybe we could add drugs to protect the ear from toxicity. Tony brought up this new idea: Why don’t we just not let the drug get in? Great idea, I thought. When do we start to work?”
Why an Ototoxic Antibiotic Remains Popular

Figure 1. Novel aminoglycosides have diminished ototoxicity in vitro.
Despite many alternative antibiotics that have come to market over the past 20 years, aminoglycosides have remained a popular choice worldwide for treating many bacterial diseases, including pneumonia, peritonitis, and sepsis. Aminoglycosides are often used when other antibiotics have failed to treat infections. Their popularity is due, in part, to their low cost, no need for refrigeration, and effectiveness at treating bacterial infections at a time when the declining potency of antibiotics is a major public health concern.

Figure 2. Sisomicin and its novel derivatives exhibit antibacterial activities.
“The toxicity of these drugs is something we accept as a necessary evil,” said Daria Mochly-Rosen, PhD, director of SPARK, a program at Stanford that assists scientists in translating their research into clinical applications.
SPARK reportedly worked closely with Ricci and Cheng, providing both the funding and the expertise necessary as they navigated the territory of drug development. Dr Mochly-Rosen believes that Dr Ricci was in a unique position to help design a better drug, given his expertise in the science of the inner ear.
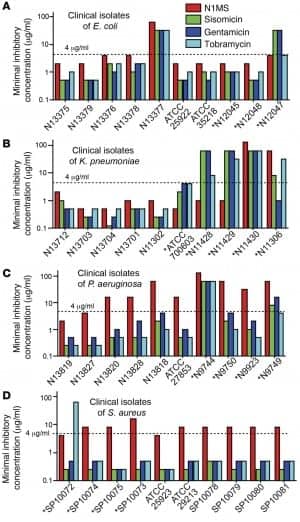
Figure 3. Sisomicin and its novel derivatives inhibit growth of different bacterial species.
Ricci said in the announcement that researchers have worked for decades looking for ways to prevent aminoglycosides like sisomicin killing off the hearing cells of the inner ear.
“So many approaches have failed,” Ricci said. “The main problem has been that if you succeeded in stopping the drug from killing hair cells, then you also stopped its antimicrobial effect. The drug just doesn’t work anymore.”
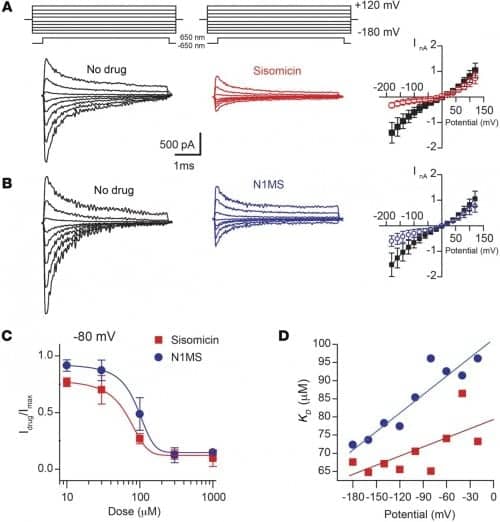
Figure 4. Hair cell MET responses at different membrane holding potentials after sisomicin and N1MS treatment.
The goal of the study led by Ricci and Cheng was to keep the antibacterial properties of the drug intact while preventing it from entering the inner-ear cell’s ion channels.
The research team used data from structural biologists at Stanford who better understood how the antibiotics fought off infection. They targeted sites on the drug molecule that were not involved in the antimicrobial activity that kills off infection, which allowed them to reduce toxicity to the ear while retaining antimicrobial action.
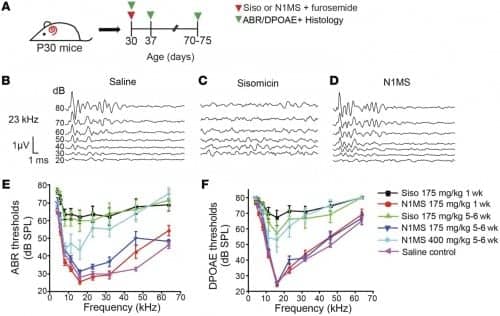
Figure 5. Modified aminoglycoside prevents hearing loss.
The researchers made nine different compounds derived from sisomicin. All nine were significantly less toxic than sisomicin to hair cells when tested in the laboratory. Three of the nine were comparable to sisomicin in combatting E. coli bacteria.
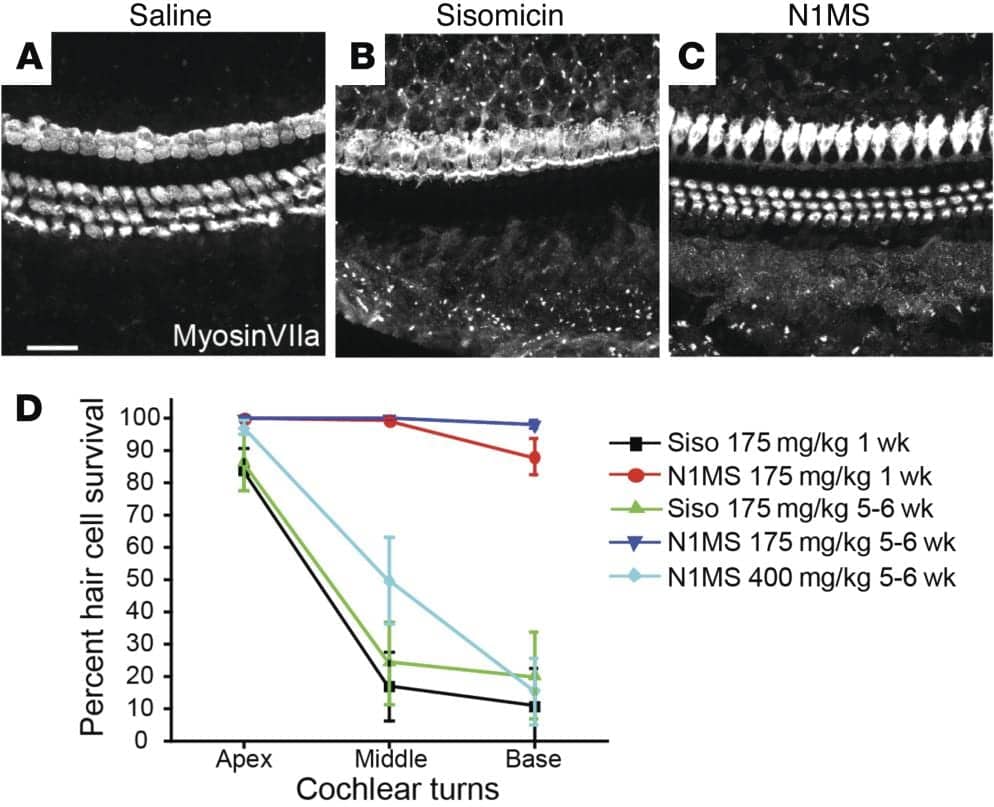
Figure 6. Modified aminoglycoside prevents sensory cell loss in vivo.
Of the three derivatives, however, N1MS was the most effective against the bacteria, and the researchers used it to successfully treat E. coli-caused bladder infection in a mouse model while leaving hearing intact. They also found that, unlike the parent compound, N1MS was nontoxic to the kidneys.
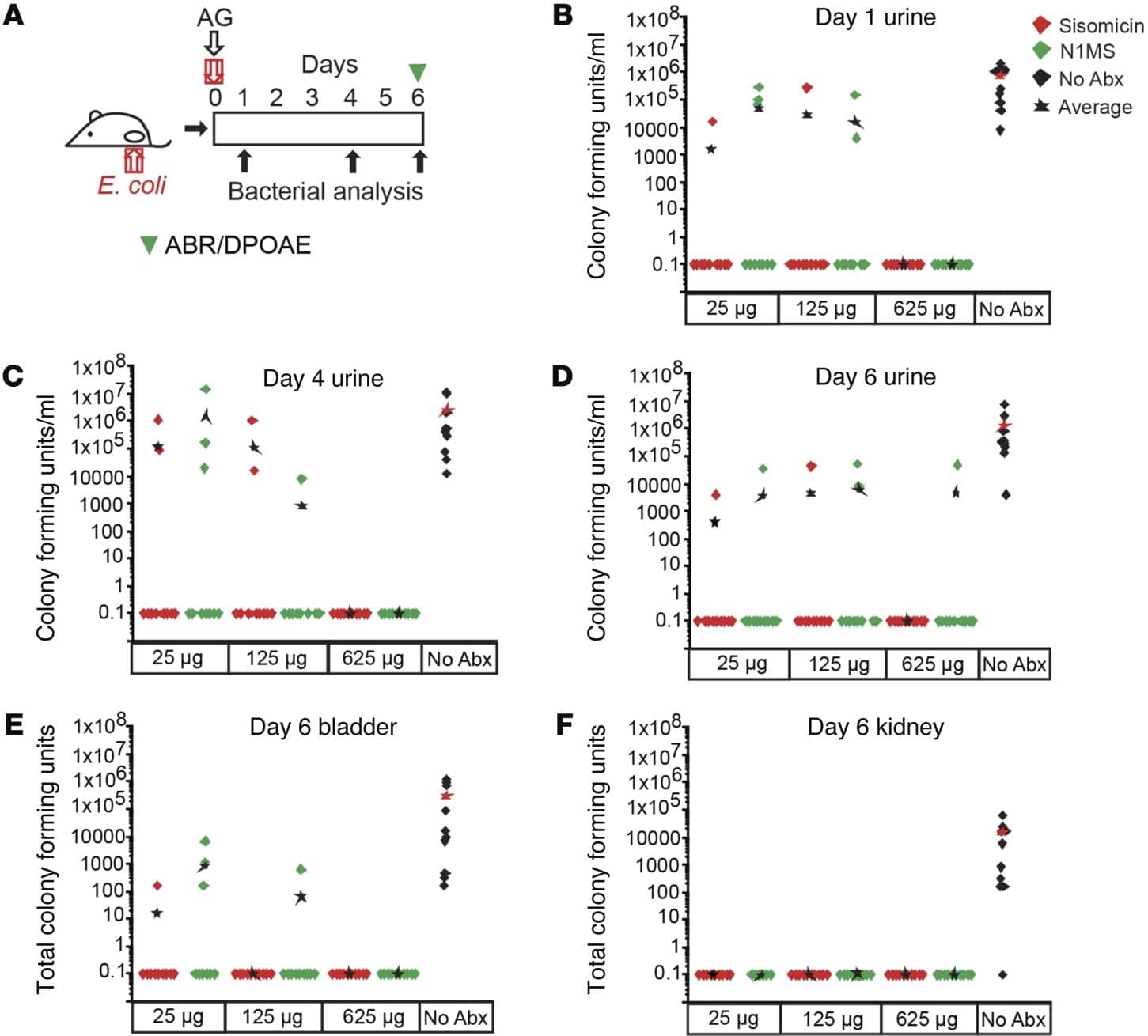
Figure 7. N1MS eradicates urinary tract infection in vivo.
“We postulate that entry into kidney cells is also through a channel, and so entry is reduced here as well,” Ricci said. “It is speculation at this point, because unlike with the hair cell, we have not measured drug entry into the kidney cells, but it seems reasonable.”
Other Stanford co-authors are postdoctoral scholars Markus Huth, MD, Yi-Ju Hsieh, PhD, Thomas Effertz, PhD, Kyu-Hee Han, MD, and Sarah Verhoeven, MD; research assistants Kayvon Sotoudeh and Andrew Vu, MD; Michael Hsieh, MD, PhD, assistant professor of urology; and SPARK chemistry consultant Robert Greenhouse, PhD.
The study was funded by the National Institutes of Health, the Swiss National Science Foundation, the Jerry Yang Faculty Scholar Fund, and SPARK.
Source: Stanford University’s Department of Otolaryngology-Head and Neck Surgery



